
Abstract
Abstract
Dantrolene is currently the only drug known to specifically treat malignant hyperthermia (MH) crises. Although dantrolene attenuates Ca2+ disorders by acting mainly on the ryanodine receptor type 1 (RYR1), some patients who manifest MH without RYR1 variants have also been successfully treated with dantrolene. Thus, dantrolene appears to have an inhibitory effect on patients with and without RYR1 variants. This study aimed to investigate whether the effects of dantrolene differed depending on the presence or absence of RYR1 variants using muscle cells from MH-predisposed individuals. The study participants were individuals diagnosed with MH predisposition by the Ca2+-induced Ca2+ release rate test. They were genetically tested and divided into two groups: with and without RYR1 variants. We investigated whether these two groups showed differences in the changes in the half-maximal effective concentration (EC50) for caffeine and the resting intracellular Ca2+ concentration ([Ca2+]i) before and after dantrolene administration. Dantrolene administration significantly increased the EC50 (P < 0.0001) and decreased the resting [Ca2+]i (P < 0.0001). The inhibitory effects of dantrolene and the presence of RYR1 variants showed no statistically significant interactions related to the EC50 (P = 0.59) and resting [Ca2+]i (P = 0.21). In conclusion, the presence or absence of RYR1 variants does not appear to influence the effect of dantrolene.
Keywords
Introduction
Malignant hyperthermia (MH) is a pharmacogenetic disorder of the skeletal muscles triggered by volatile anaesthetics or the depolarising muscle relaxant succinylcholine. The pathophysiology of MH is related to malfunction of intracellular Ca2+ homeostasis, and MH symptoms manifest as a lethal hypermetabolic crisis associated with a rapid and uncontrolled increase in intracellular Ca2+ levels in skeletal muscle cells. Abnormal Ca2+ metabolism is mainly caused by functional, structural and morphological abnormalities of ryanodine receptor type 1 (RYR1), which have a significant involvement in susceptibility to MH. The gene variants of RYR1 contribute to MH susceptibility, and 48 RYR1 variants have been identified as diagnostic genetic variants by the European Malignant Hyperthermia Group (EMHG). 1
Many studies have confirmed that the muscles of MH-susceptible individuals exhibit increased sensitivity to direct RYR1 agonists, such as caffeine, halothane and 4-chloro-m-cresol (4CmC), and this increased sensitivity is also likely to be the primary underlying mechanism for triggering the clinical MH syndrome. 2 Moreover, defective or disordered RYR1 results in uncontrolled release of intracellular Ca2+ from the skeletal muscle sarcoplasmic reticulum (SR). In fact, a high resting intracellular Ca2+ concentration ([Ca2+]i) has been found in MH-susceptible patients. 3
Dantrolene is the only clinically available agent for the specific treatment of an MH crisis, and its discovery was followed by a substantial reduction in the mortality and morbidity of MH. 4 Dantrolene is a direct-acting skeletal muscle relaxant that blocks Ca2+ release from intracellular storage in the SR. Previous studies have shown that dantrolene acts mainly on RYR1 to inhibit the extent of channel activation. It also decreases Ca2+ sensitivity of channel activation and interacts with RYR1 to suppress the channel dysfunction that occurs with MH variants. 5
Despite the fact that dantrolene shows inhibitory effects on abnormal Ca2+ metabolism by acting mainly on RYR1, some individuals showing MH susceptibility without RYR1 variants have also been successfully treated with dantrolene administration. 6 Thus, dantrolene appears to have an inhibitory effect on both patients with and without RYR1 variants. If the effect of dantrolene is mainly attributable to its effect on RYR1 dysfunction, its effects may differ depending on the presence or absence of RYR1 variants. To date, no reports have examined whether the presence or absence of RYR1 variants causes differences in the potency of dantrolene in human muscle cells. In this study, we investigated whether the effects of dantrolene differed depending on the presence or absence of RYR1 variants using muscle cells from MH-predisposed individuals.
Methods
Protocol
This study was approved by the ethics committee of Hiroshima University Hospital (ヒ-151-9), and written consent was obtained from all participants before the Ca2+-induced Ca2+ release (CICR) rate test for the use of residual skeletal muscle for the experiments.
Eleven individuals diagnosed with MH predisposition by the CICR rate test were included in this study. They were genetically tested and divided into two groups: those with RYR1 variants (with RYR1 group) and those without RYR1 variants (without RYR1 group). We investigated whether these two groups showed differences in the changes in the half-maximal effective concentration (EC50) for caffeine and resting [Ca2+]i before and after dantrolene administration. Five individuals, diagnosed as MH-negative (MHN) because their CICR was not accelerated, were excluded from the dantrolene study. Thus, no genetic testing was performed on them.
CICR rate test
The CICR rate test was performed as described previously. 7 Accelerated CICR was defined as a CICR rate more than two standard deviations above the mean of the control CICR values, which were derived from 12 patients with negative results in in vitro contracture tests (IVCT; EMHG protocol) and caffeine–halothane contracture tests (CHCT; North American MH Group protocol) at two or more Ca2+ concentrations in accordance with a previous study. 8
Genetic testing
After obtaining written consent from the study participants, we asked the National Centre of Neurology and Psychiatry to conduct genetic tests to examine the gene variants in the RYR1 region. In one case (case no. 4), genetic testing was performed at Keio Hospital.
Myotube cultures
As described previously, 9 myoblasts were obtained from the surplus muscle pieces after CICR examination and cultured in Dulbecco’s modified Eagle’s medium and F12 medium (DMEM/F12; Invitrogen, Carlsbad, CA, USA) supplemented with 10% heat-inactivated fetal bovine serum (FBS; Sigma–Aldrich, St Louis, MO, USA). The myoblasts were then frozen and stored at –70°C. The frozen myoblasts were defrosted and plated on 35 mm glass-bottom culture dishes with DMEM/F12 medium supplemented with 10% FBS at 37°C under 5% CO2. At 80% confluence, the medium was changed to DMEM/F12 supplemented with 2% FBS to induce differentiation into myotubes. Seven to 14 days after the medium change, measurements were performed on cells that had morphologically changed into multinucleated and spindle-shaped cells. The following experiments were conducted multiple times using multiple myotubes cultured from the surplus muscle pieces of each case.
Ca2+ imaging
Ca2+ imaging from a single myotube was performed using the Ca2+ fluorescence indicator Fura-2/AM (Dojindo Molecular Technologies, Tokyo, Japan), as previously described.10,11 Cells were loaded on Fura2/AM at 37°C for one hour and then washed in Hank’s balanced salt solution (HBSS). The ionic composition of HBSS was as follows: 130 mM NaCl, 5.4 mM KCl, 20 mM 2-[4-(2-Hydroxyethyl)-1-piperazinyl]ethanesulfonic acid (HEPES), 2.5 mM CaCl2, 1 mM MgCl2 and 5.5 mM glucose (pH 7.4). The HBSS used in the experiment was prepared by us. The myotubes on the glass-bottom dishes were maintained for 30 minutes. The myotubes were perfused with HBSS for 30 minutes at a rate of 1.2 ml/min at 37°C prior to the experiments. The myotubes were excited at 340 and 380 nm at 37°C, and the measurements to evaluate intracellular Ca2+ changes were obtained at 510 nm using a fluorescence microscope (Nikon, Tokyo, Japan). Perfusion with HBSS was performed, and a Ca2+ image analyser (Aquacosmos 2.5; Hamamatsu Photonics, Hamamatsu City, Japan) was used to calculate the 340/380 nm wavelength ratio.
A calibration kit (Invitrogen™, ThermoFisher Scientific, Tokyo, Japan) was used to convert the 340/380 nm wavelength ratio to [Ca2+]i values. Of the myotubes that were successfully cultured, only those in which the 340/380 nm wavelength ratio increased in response to 10 mM caffeine were determined to have successfully expressed RYR1, and were included in the measurement.
Measurement of the sensitivity for 4-chloro-m-cresol and caffeine
Myotubes were perfused with HBSS containing 10 mM caffeine before measurements were obtained. The 340/380 nm wavelength ratio was measured when HBSS containing incremental levels of 4 chloro-m-cresol (4CmC) was perfused into the culture dish. Each solution was washed out for two minutes prior to adding the next incremental level of 4CmC; 4CmC was evaluated at 3, 10, 30, 100, 300, 500 and 1000 μM. The sensitivity of caffeine was measured in the same manner. Various concentrations of caffeine (0.25, 0.5, 1.0, 2.5, 5.0, 10.0 and 20.0 mM) were added to HBSS, and caffeine-induced changes in the 340/380 nm wavelength ratio were measured.
Measurement of the caffeine sensitivity following dantrolene administration
The sensitivity of dantrolene to caffeine was measured by replacing HBSS with HBSS supplemented with 5 or 15 μM dantrolene. Caffeine was added to the HBSS at increasing concentrations in the same way and at the same concentrations as described above, and the caffeine-induced changes in the 340/380 nm wavelength ratio with the addition of dantrolene were measured. After the measurements, myotubes were perfused with HBSS without dantrolene, and the 340/380 nm wavelength ratio was measured with the addition of 10 mM caffeine. When the 340/380 nm wavelength ratio reduced to < 80% of the 340/380 nm wavelength ratio measured before dantrolene addition, the values were discarded and removed from this study (Figure 1).
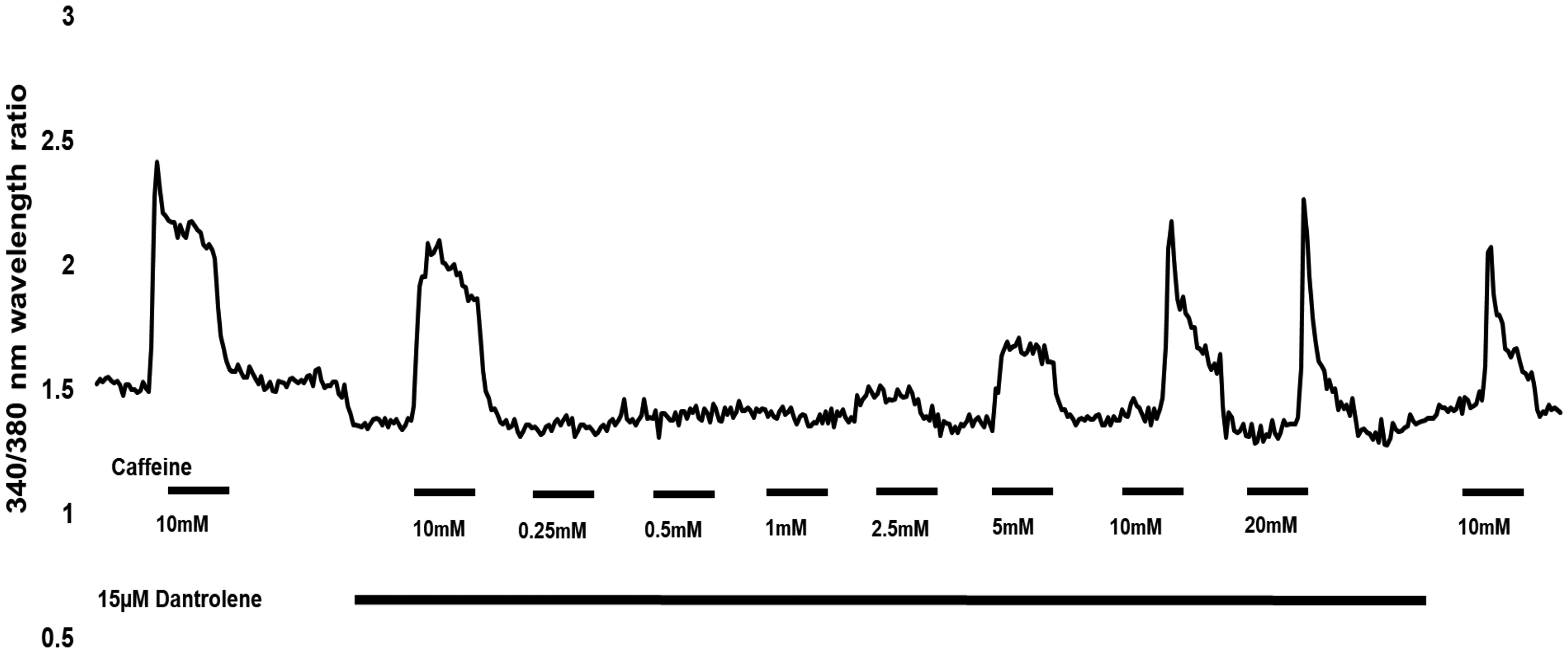
Representative recording of Ca2+ fluorescence measurement for caffeine in the myotube. The horizontal axis shows the time, and the vertical axis shows the 340/380 nm wavelength ratio of Fura-2 AM fluorescence intensity. The upper bar and the concentration below it indicate the duration of caffeine addition and its concentration. The lower bar indicates perfusion of HBSS with dantrolene. HBSS: Hank’s balanced salt solution.
Measurement of resting [Ca2+]i before and after dantrolene addition
The resting [Ca2+]i was calculated from the 340/380 nm wavelength ratio before stimulation with 10 mM caffeine. After measurement of resting [Ca2+]i, the resting [Ca2+]i with the addition of dantrolene was measured by replacing HBSS with HBSS supplemented with 50 μM dantrolene. The resting [Ca2+]i with the addition of dantrolene was calculated from the 340/380 nm wavelength ratio two minutes after replacing HBSS.
Data analysis
For both the EC50 value and the resting [Ca2+]i value, the median value of each case was used to eliminate outliers. The EC50 of 4CmC and caffeine were calculated from the dose–response curves. To trace these curves, the data were normalised to the maximal response of each myotube. With regard to changes in EC50 and resting [Ca2+]i, two-way repeated-measures analysis of variance was used to evaluate differences between the groups with and without RYR1 and between the conditions before and after dantrolene addition. For the examination of the effect of dantrolene on EC50, Tukey’s multiple comparison test was used for the post hoc test. Regression analysis was used to examine the correlation between resting [Ca2+]i and the EC50 values of caffeine. The difference was considered statistically significant when the P-value was < 0.05. The data were analysed using PRISM v8.0 (GraphPad Software, San Diego, CA, USA).
Results
Gene testing
Of the 11 cases, six showed RYR1 variants. Table 1 shows the results of gene testing and the RYR1 variants found in each case.
The RYR1 variants that were identified.
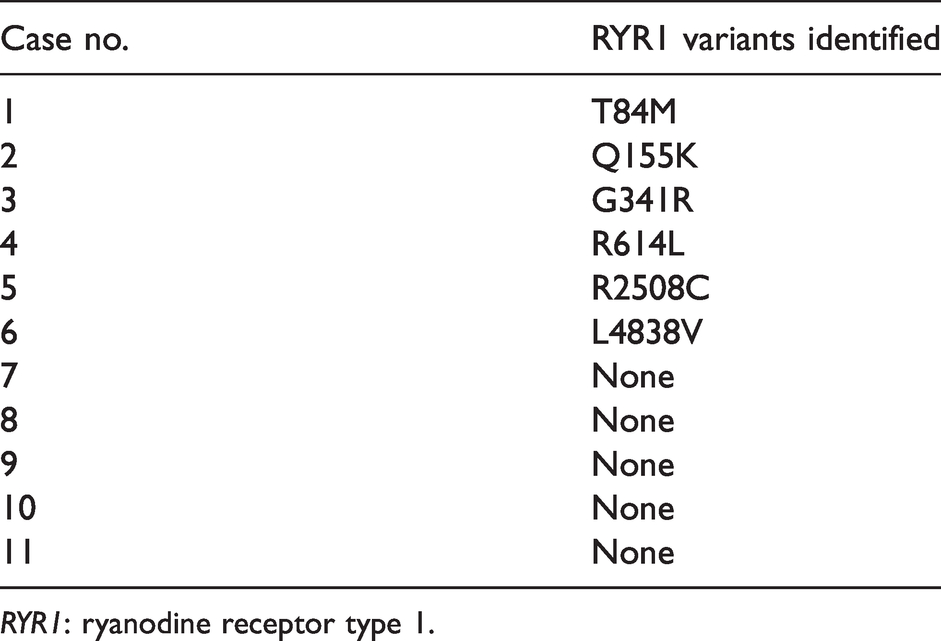
RYR1: ryanodine receptor type 1.
The median EC50 values of 4CmC and caffeine
EC50 values of 4CmC and caffeine and their statistical significance for each group and for the five individuals with MHN whose CICR rate was not accelerated are presented in Tables 2 and 3, respectively. There was no significant difference between the with RYR1 and without RYR1 groups in the EC50 for either 4CmC or caffeine. The median EC50 values of 4CmC and caffeine in the groups with and without RYR1 variants were significantly lower than those in the MHN group.
The median EC50 value of 4CmC and caffeine in each case.
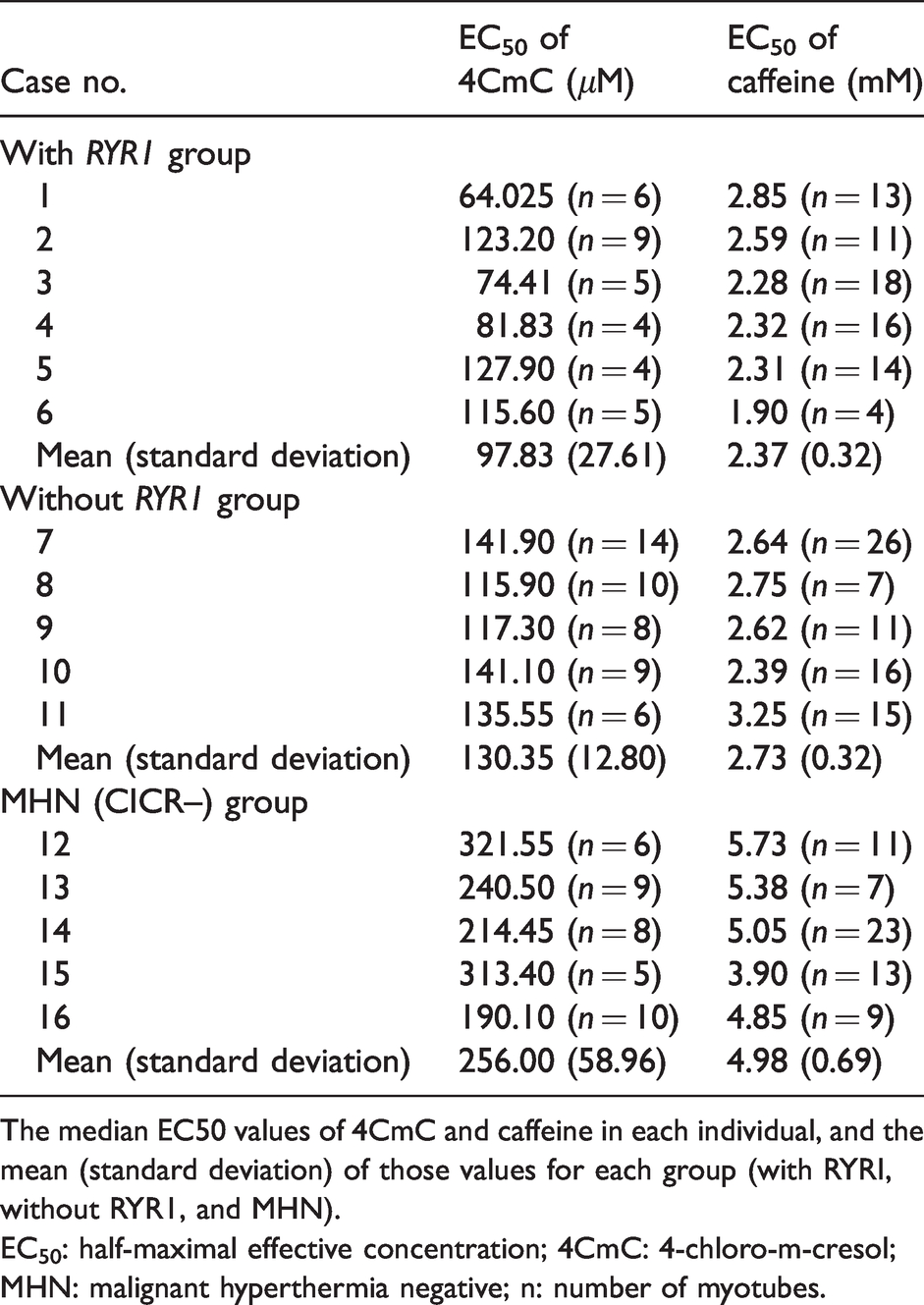
The median EC50 values of 4CmC and caffeine in each individual, and the mean (standard deviation) of those values for each group (with RYRI, without RYR1, and MHN).
EC50: half-maximal effective concentration; 4CmC: 4-chloro-m-cresol; MHN: malignant hyperthermia negative; n: number of myotubes.
Results of one-way analysis of variance for EC50 values of 4CmC and caffeine between the with RYR1 group, without RYR1 group and MHN group.
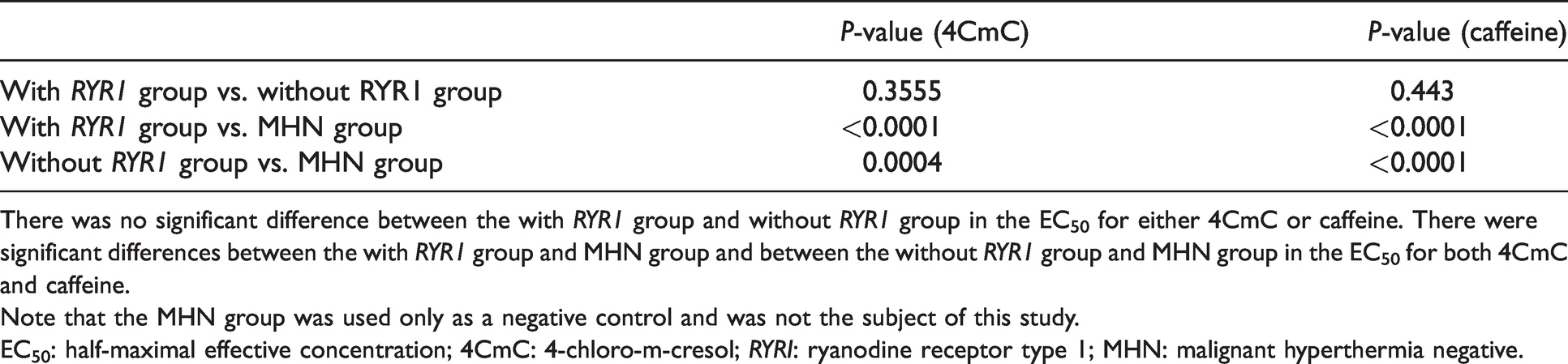
There was no significant difference between the with RYR1 group and without RYR1 group in the EC50 for either 4CmC or caffeine. There were significant differences between the with RYR1 group and MHN group and between the without RYR1 group and MHN group in the EC50 for both 4CmC and caffeine.
Note that the MHN group was used only as a negative control and was not the subject of this study.EC50: half-maximal effective concentration; 4CmC: 4-chloro-m-cresol; RYRI: ryanodine receptor type 1; MHN: malignant hyperthermia negative.
Median EC50 values of caffeine and the changes in the EC50 of caffeine with dantrolene
The median EC50 values of caffeine for the two groups before dantrolene addition and with the addition of 5 and 15 μm dantrolene are shown in Figure 2(a). The P-value for the median EC50 between the with and without RYR1 groups was 0.04 (Figure 2(b)). The EC50 of caffeine was significantly increased by the addition of dantrolene (P < 0.0001; Figure 2(c)). However, the changes in the EC50 values of caffeine did not show a significant interaction between dantrolene addition and the presence of RYR1 variants (P = 0.59). Results indicated that dantrolene had a significant effect on the changes in the EC50 values.
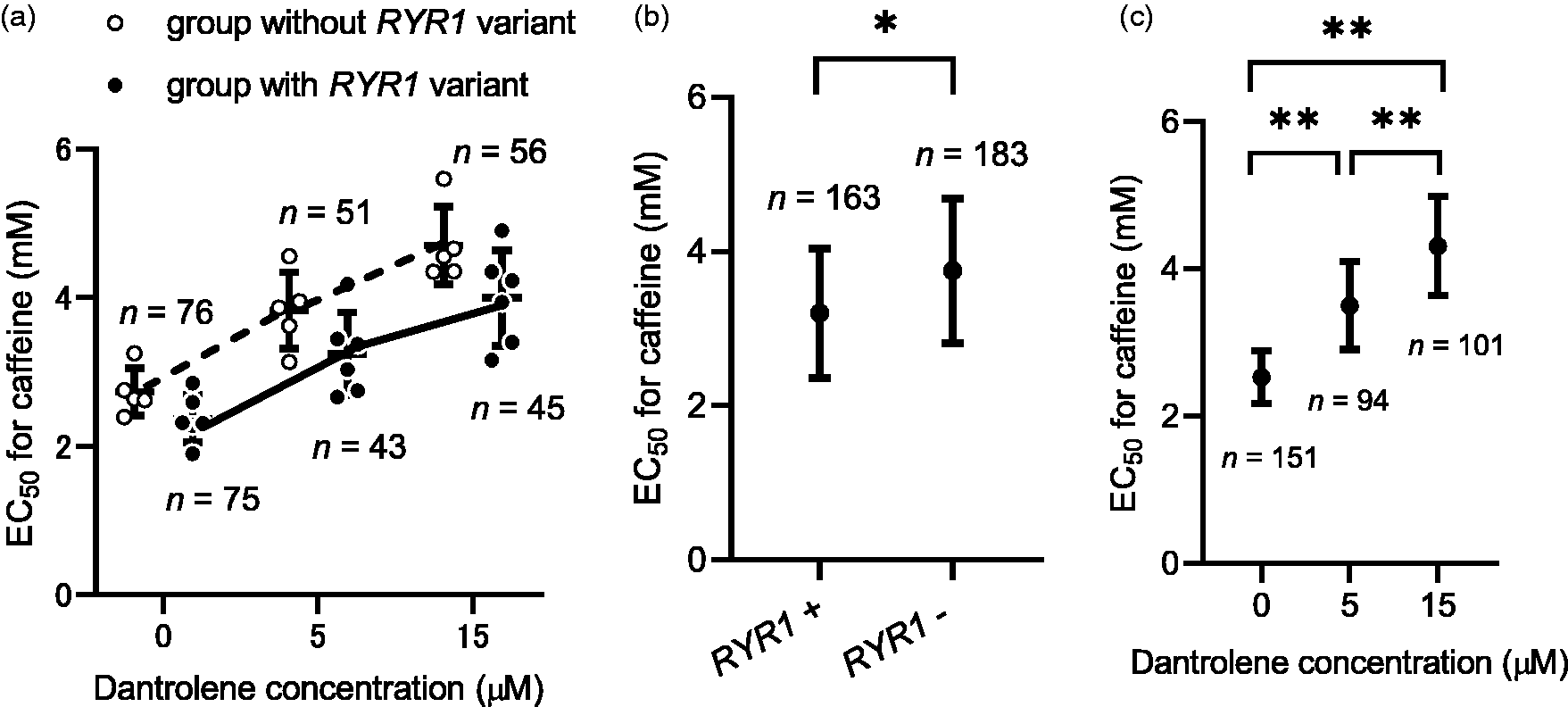
The median EC50 values for caffeine before and after dantrolene addition in individuals with and without RYR1 variants. (a) Scatter plot showing the median EC50 for each individual in both groups at each dantrolene concentration. In the two-way ANOVA, there was statistically no influence of interaction between dantrolene and RYR1 variants on the EC50 (dantrolene×RYR1 variant: P=0.59). (b) The graph shows the median EC50 of each group (with or without RYR1 variation) in the present study. In the two-way ANOVA, the factor RYR1 variant was significant (RYR1 variant: P=0.04). (c) In the two-way ANOVA, the factor dantrolene was significant (dantrolene: P < 0.0001). Tukey’s multiple comparison test showed that EC50 changed significantly depending on the dantrolene dose. Data represent mean (standard deviation). The circles and open circles show the median EC50 for each individual; n indicates the number of myotubes used. ANOVA: analysis of variance; EC50: the half-maximal effective concentration; RYR1: ryanodine receptor type 1. *P < 0.05; **P < 0.0001.
Changes in the resting [Ca2+]i with dantrolene
The median resting [Ca2+]i varied among the RYR1 variants, with the T84M and R614L variants presenting the lowest (77.04 nM) and the highest (123.75 nM) values, respectively. Similarly, the median resting [Ca2+]i varied from 57.35 to 123.33 nM in the group without RYR1 variants (Figure 3(a)). The mean (standard deviation (SD)) values of the median resting [Ca2+]i in the two groups were 104.08 (16.50) and 81.76 (26.82) nM in the with RYR1 group and without RYR1 group, respectively. The mean (SD) values of the median resting [Ca2+]i with dantrolene in the two groups were 74.05 (14.00) and 60.53 (19.49) nM in the with RYR1 group and without RYR1 group, respectively. Although there was no significant difference in the median resting [Ca2+]i values between the two groups (P = 0.15; Figure 3(b)), the addition of dantrolene significantly decreased the median resting [Ca2+]i values (P < 0.0001; Figure 3(c)). There was no significant interaction between the reduction of resting [Ca2+]i by dantrolene addition and the presence of RYR1 variants (P = 0.21). The scatter plot data (Figure 3(a)) shows comparisons between the two groups for the relative contribution of dantrolene to the resting [Ca2+]i.
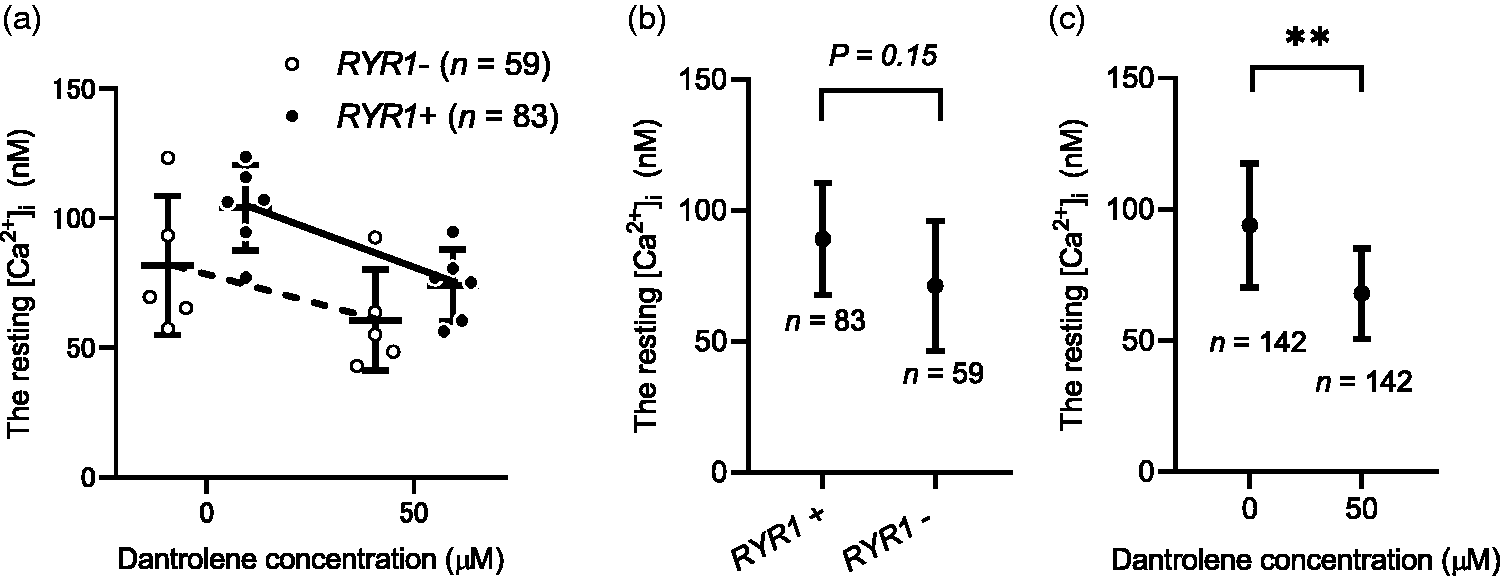
The median resting [Ca2+]i values before and after dantrolene addition in cases with and without RYR1 variants. (a) The scatter plot data showing comparisons between the groups with and without RYR1 variant for the relative contribution of dantrolene to the resting [Ca2+]i. In the two-way ANOVA, there was no significant interaction between the reduction of resting [Ca2+]i values by dantrolene administration and the presence of RYR1 variant (dantrolene×RYR1 variant: P = 0.21). (b) The graph shows the resting [Ca2+]i values of each group (with or without RYR1 variation) in this study. In the two-way ANOVA, the factor RYR1 variant was not significant (RYR1 variant: P = 0.15). (c) The graph shows the resting [Ca2+]i values before and after dantrolene administration for all participants in this study. In the two-way ANOVA analysis, the resting [Ca2+]i values were significantly decreased by dantrolene administration (P < 0.0001). Data represent mean (standard deviation). The circles and open circles show the median EC50 for each individual; n indicates the number of myotubes used. **P < 0.0001.RYR1: ryanodine receptor type 1; ANOVA: analysis of variance.
Correlation between the resting [Ca2+]i and caffeine EC50 values
Our results showed no correlation between resting [Ca2+]i and the EC50 values of caffeine (r2 = 0.08, P = 0.40).
Discussion
We have shown that the inhibitory effect of dantrolene did not differ in the presence or absence of RYR1 variants in human muscle cells with an MH predisposition. This confirms that dantrolene is an effective treatment for patients with MH, regardless of whether they have RYR1 variants.
The experimental data showed that RYR1 variants did not influence the alleviating effect of dantrolene on sensitivity to caffeine. The EC50 values for 4CmC and caffeine were significantly lower in both the with and without RYR1 groups than in the MHN group.
The median resting [Ca2+]i value varied in myotubes with or without RYR1 variants, which is consistent with the findings from a previous report in which the resting [Ca2+]i differed depending on the site of the variant. 12
According to a previous report, 13 spontaneous Ca2+ leakage through MH mutant channels can lead to changes in the resting [Ca2+]i, but compensatory mechanisms exist, leading to the rapid re-establishment of Ca2+ homeostasis. The compensatory control of resting [Ca2+]i in skeletal muscle is thought to involve the expression of sarcoplasmic/endoplasmic reticulum Ca2+ ATPase, Ca2+ pumps that take up Ca2+ from the cytoplasm into the SR, and other channels, pumps and exchangers involved in Ca2+ metabolism in both the sarcolemma and SR. The decrease in resting [Ca2+]i in all myotubes suggests that dantrolene suppresses Ca2+ leakage from the SR to the cytoplasm independent of RYR1 variants. Dantrolene has other sites of action in addition to RYR1, and previous studies using animal models have reported that dantrolene acts on Ca2+ regulatory mechanisms other than RYR1. For example, dantrolene has been previously shown to block non-specific sarcolemmal cation entry channels and it has been suggested that the action at these channels may be important for the therapeutic effects of dantrolene in MH. This result is consistent with the results of our study using human muscle cells. 14
Caffeine increases the open probability of RYR1 and facilitates Ca2+ release. 15 A reduction in the EC50 for caffeine is a sign of accelerated Ca2+ release via RYR1 variants. Tong et al. reported that the resting [Ca2+]i showed no linear correlation with caffeine sensitivity. 13 Our results also showed no correlation between the resting [Ca2+]i and the caffeine EC50 values. Thus, in assessments regarding abnormalities of the Ca2+ metabolism in MH, EC50 can be considered as an independent factor of resting [Ca2+]i.
A limitation of this study is that the presence of MH predisposition was determined by the CICR rate test rather than the more widely accepted CHCT/IVCT. However, the CICR rate test can reveal abnormalities associated with Ca2+ release from the SR, a process mainly controlled by RYR1 in skeletal muscle. 9 The EC50 values of 4CmC and caffeine in participants with accelerated CICR rates in this study were lower than the previously reported cut-off values to diagnose MH, 9 which confirmed that the participants in this study had MH predisposition. The RYR1 variants identified in this study are shown in Table 1. Of these, G341R, R614L, R2508C and L4838V have been recognised as diagnostic MH variants by EMHG. 1 T84M and Q155K were functionally analysed in a previous study and have been suggested to contribute to MH crisis.16,17 Using a modified version of the American College of Medical Genetics and Genomics guidelines, 18 the T84M and Q155K variants can be classified as uncertain significance and likely pathogenic, respectively.
Another major limitation of this study was the limited number of samples. Therefore, care should be taken in interpreting the results of the statistical tests in this study.
Another limitation is that RYR1 expression was not consistent in all the cultured and differentiated myotubes. Since RYR1 expression itself significantly increases the resting [Ca2+]i, 19 differences in the degree of differentiation of the sample myotubes may have resulted in differential expression of RYR1 and affected the assessment of the resting [Ca2+]i. Because of the limited number of myotubes that could be cultured from muscle biopsies, it was difficult to evaluate the RYR1 expression by western blotting in this study.
In the present study, the resting [Ca2+]i was calculated by converting the 340/380 nm wavelength ratio to [Ca2+]i. The calibration curve was constructed by adding Fura-2 to the Ca2+ buffer, of known Ca2+ concentration, measuring the fluorescence intensity ratio of the buffer and then plotting the Ca2+ concentration against the ratio value. However, it has been reported that fluorescence indicators in cells, such as Fura-2, interact with high concentrations of intracellular proteins and cell membranes, altering their fluorescence properties and chelation constants and changing their fluorescence spectra with Ca2+ buffer.20,21 Reportedly, when the protein concentration increases, [Ca2+]i produced by the calibration curve using Ca2+ buffer is measured to be lower than the actual [Ca2+]i concentration. Furthermore, it is difficult to make a buffer with the exact intracellular composition, and therefore an accurate calibration curve cannot be plotted. Thus, it should be noted that the resting [Ca2+]i in this study may differ from the actual values.
In skeletal muscle, the resting [Ca2+]i is determined by Ca2+ movement between the cytosol, SR and the extracellular matrix. Both RYR1 and dihydropyridine receptor (DHPR) are involved in Ca2+ release from SR, and mutations in calcium channel, voltage-dependent, L type, α1S subunit (CACNA1S), which encodes DHPR, have been implicated in MH. The influx of extracellular Ca2+ occurs through store-operated Ca2+ entry (SOCE), transient receptor potential and excitation-coupled Ca2+ entry. Orai1 and stromal interaction molecule 1 are Ca2+ proteins mainly responsible for SOCE in skeletal muscle. Therefore other factors aside from RYR1 variants may influence resting [Ca2+]i in myotubes from individuals predisposed to MH.
In addition to RYR1, CACNA1S and STAC3 have also been associated with MH susceptibility and severe dysregulation of skeletal muscle Ca2+ homeostasis, which results in the clinical features of an MH reaction under anaesthesia. The relationship between genetic variants in these genes and the effects of dantrolene should be investigated in the future.
In conclusion, as there was no significant interaction between the inhibitory effect of dantrolene and the presence or absence of the RYR1 variants in either EC50 for caffeine or resting [Ca2+]i, these inhibitory effects of dantrolene did not differ in relation to the presence or absence of RYR1 variants.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.