
Abstract
Anaesthetic choice for large joint surgery can impact postoperative outcomes, including mortality. The extent to which the impact of anaesthetic choice on postoperative mortality varies within patient populations and the extent to which anaesthetic choice is changing over time remain under-explored both internationally and in the diverse New Zealand context. In a national study of 199,211 hip and knee replacement procedures conducted between 2005 and 2017, we compared postoperative mortality among those receiving general, regional or general plus regional anaesthesia. Focusing on unilateral (n=86,467) and partial (n=13,889) hip replacements, we assessed whether some groups within the population are more likely to receive general, regional or general plus regional anaesthesia than others, and whether mortality risk varies depending on anaesthetic choice. We also examined temporal changes in anaesthetic choice over time. Those receiving regional alone or general plus regional for unilateral hip replacement appeared at increased risk of 30-day mortality compared to general anaesthesia alone, even after adjusting for differences in terms of age, ethnicity, deprivation, rurality, comorbidity, American Society of Anesthesiologists physical status score and admission type (e.g. general plus regional: adjusted hazard ratio (adj. HR)=1.94, 95% confidence intervals (CI) 1.32 to 2.84). By contrast, we observed lower 30-day mortality among those receiving regional anaesthesia alone compared to general alone for partial hip replacement (adj. HR=0.86, 95% CI 0.75 to 0.97). The latter observation contrasts with declining temporal trends in the use of regional anaesthesia alone for partial hip replacement procedures. However, we recognise that postoperative mortality is one perioperative factor that drives anaesthetic choice.
Introduction
There are a number of factors that influence the choice of anaesthetic for large joint surgeries, including hospital protocols, surgeon preferences, patient choice and patient factors such as age and comorbidity. With nearly 90% of all musculoskeletal procedures performed under general anaesthesia (see Supplemental Material S1), hip and knee arthroplasty are two of the relatively few procedures that are fairly interchangeably performed under regional/neuraxial (hereafter regional) anaesthesia. 1 Among those receiving regional compared to general anaesthesia, there is some evidence of reduced risk of postoperative infection,2– 5 reduced unplanned intubations, 6 reduced risk of blood transfusion,5,7 reduced rates of stroke, cardiovascular and other pulmonary complications,2,6 reduced opioid consumption 8 and reduced postoperative pain. 8 Evidence from propensity score analyses, in which patients are matched based on a host of factors that might influence anaesthetic choice, suggests that there may be some postoperative mortality benefit to the use of regional anaesthesia over general anaesthesia in hip or knee arthroplasty,9,10 although this has not been observed across all studies that have compared this factor between anaesthetic types. 1
The impact of anaesthetic type on risk of postoperative mortality for large joint surgeries remains unexplored in the New Zealand context, as does the extent to which anaesthetic choice varies by patient subgroup (age, ethnicity, comorbidity, etc.). Additionally, the extent to which the impact of anaesthetic type on risk of postoperative mortality varies by patient subgroup (e.g. age, comorbidity, ethnicity) also remains under-explored internationally.
In this article, we use comprehensive, high-quality national-level data to compare postoperative mortality outcomes among those receiving general versus regional anaesthesia in the context of hip and knee arthroplasty within New Zealand. First, we describe the main procedure types performed under each anaesthetic type, and then describe the age-adjusted rates of 30- and 90-day death for each procedure type. Next, using common procedures as exemplars, we assess (a) whether some groups within the population are more likely to receive regional anaesthesia than others, and (b) whether mortality risk varies within these specific strata depending on the choice of anaesthetic–adjusting for the impact of other factors that may contribute to both anaesthetic choice and risk of mortality following surgery (age, comorbidity, etc.).
Methods
Participants and data sources
Our study cohort included all individuals who underwent a hip or knee arthroplasty (International Classification of Diseases (ICD)-10-AM/ACHI (Australian Classification of Health Interventions) 3rd edition codes: hip arthroplasty 114,925; knee arthroplasty 84,286; see procedure codes in Supplemental Material S2) between 1 January 2005 and 31 December 2017. This cohort are a subset of a larger pan-procedure cohort which we have previously described, 11 with the methods of the current study overlapping with the methods used in that broader study. National-level hospitalisation data (National Minimum Dataset; NMDS12) were used to find eligible hospital admissions over the study period that included procedures. The NMDS is a record of all publicly funded (and most privately funded) inpatient events in New Zealand (a country with universal healthcare). Clinical coders code diagnoses and procedures at a regional level, and these data are then reported to the central NMDS collection. 12 To allow for patients who had more than one hip or knee arthroplasty during their admission, admissions were further divided into the individual days that procedures were performed during the admission. It was possible for individuals to have both a hip and a knee procedure during the study period, including during the same procedure–in which case, the two procedures were treated as separate events for the purposes of our analyses. We restricted our analysis to New Zealand residents to ensure follow-up for postoperative death.
Patient comorbidity at the start of each admission (see Variables below) was measured using data on recorded diagnoses from public and private hospital admission records for the five-year period prior to the admission. Date of death was defined using the date of death variable that appears on the National Health Index dataset. 13
Variables
All variables were derived from the NMDS dataset. Primary anaesthetic type was defined using ICD codes (general anaesthesia 9251410–9251499; regional anaesthesia 9250610–9251299). Regional anaesthesia included both neuraxial block (9250610–9250899) and regional block (9250910–9251299). For a given procedure, primary anaesthesia was defined as that which occurred on the day of the surgical procedure. We created three separate anaesthetic groups: those who received general anaesthesia only, those who received regional anaesthesia only and those who received both a general and regional anaesthesia.
Patient age was defined at the time of procedure (categorised as < 55, 55–64, 65–74 or 75+ years). This age categorisation balanced clinical relevance against the size of the individual age groups, the latter of which will influence the statistical precision of our findings. Patient sex was defined at the time of the surgical procedure and categorised as either male or female, as only these two categories were recorded in the hospital data. Ethnicity data were sourced from NMDS (time of admission) and prioritised into mutually exclusive categories of Māori, Pacific, Asian, European or Middle Eastern/Latin American/African/other. 14 NMDS ethnicity data collections are guided by ethnicity data protocols, which ideally require patient self-identification.
Area deprivation for each patient at the time of procedure was determined using New Zealand’s 2013 Deprivation Index (NZDep) for each individual’s residential address (and subsequent domicile code). 15 NZDep deciles were collapsed into quintiles ranging from 1 (least deprived) to 5 (most deprived). NZDep data were missing for 1456 hip procedure patients (1% of cohort) and 1585 knee procedure patients (1% of cohort). Patient rurality was defined using a modified version of the Urban/Rural Profile Classification (URPC), 16 with the area where the patient lived at the time of the procedure classified as urban (main urban area+satellite urban area), independent urban or rural. Rurality data were missing for 1080 hip procedure patients (1% of cohort) and 1187 knee procedure patients (1% of cohort).
Patient comorbidity was defined using the M3 Index. 17 For each patient, NMDS data from the five-year period prior to the date of admission for the given procedure were searched for the presence of any of the 61 conditions included in the M3 Index using ICD-10 codes, and a final comorbidity score was calculated (see Stanley and Sarfati 17 for weights and more information about the M3 Index). For descriptive analysis, M3 scores were categorised as 0, >0–1, >1–2, >2–3 or 3+, while for regression models, M3 score was included as a splined variable 17 with knots placed at the 0th, 90th and 95th percentiles. 18 American Society of Anesthesiologists (ASA) physical status score was determined from ICD anaesthesia codes and categorised as either 1–2, 3, 4–5 or unknown. 19 In those instances where more than one ASA score was coded on a given procedure day, a give-way rule was applied wherein the worst ASA score was retained for that procedure day. All procedures were assigned an admission type, depending on the reason for their hospital admission, with admission type categorised as either acute or elective/waiting list. Postoperative mortality was defined as death from any cause recorded within either 30 or 90 days of that procedure, inclusive of the date of the procedure.
Statistical analysis
Descriptive analyses included crude counts and age-standardised rates (per 100 procedures). Because of the possibility that there might be differences in age distribution between those given general anaesthesia and those given regional anaesthesia, we age standardised rate data to the age structure of the entire combined arthroplasty population, in order to account for changes in population age structure over time.
In order to establish the independent relationship between anaesthetic type and risk of 30-day mortality within each of our patient subgroups (‘covariates’), we conducted Cox proportional hazards regression modelling. Within the Cox model, we censored procedures when either (a) no death occurred within 30 days of the procedure, or (b) if a prior procedure occurred within a 30-day period from the date of the original procedure. 19 As such, for those who had multiple procedures within a given 30-day period, the first procedure was used as the index procedure. Hazard ratios (HR) and their 95% confidence intervals (CI) were determined for the risk of 30-day mortality between anaesthetic types for each modelled variable (age, sex, ethnicity, deprivation, rurality, M3 score, ASA score and admission type), giving the risk of mortality within each stratum of each covariate, adjusted for all other covariates in the model (with the exception of M3 and ASA, which were not mutually adjusted for each other due to possible collinearity).
Finally, we determined temporal trends in the crude proportion of procedures that were conducted under each of the anaesthesia types over the study period. To test for notable increases or decreases in the rate of a given anaesthesia type over time, we fitted a linear regression model to each procedure, separately for each anaesthetic group stratum, with procedure year as the independent variable and the number of procedures as the dependent variable. We output P-values from the resulting parameter estimates to augment our assessment of changes in anaesthetic use over time for each procedure. We repeated these analyses with further stratification by age group to assess whether changes over time were occurring consistently across age groups.
Data management and analysis was performed using SAS v9.4 (SAS Institute, Inc., Cary, NC, USA), Stata v16 (StataCorp LLC, College Station, TX, USA) and Microsoft Excel 2016 (Microsoft Corp., Redmond, WA, USA). The study sought and received ethical approval from the University of Otago Human Ethics Committee (reference: H18/085).
Results
The total number of hip or knee procedures and the deaths that occurred within 30 or 90 days of these procedures are presented in Table 1. The vast majority of the 114,925 hip procedures performed over the study period were unilateral hip replacements (72%), followed by hip revisions (14%), partial hip replacements (also known as hemiarthroplasty; 12%), bilateral hip replacements (1%) and hip excisions (1%). The vast majority of the 84,286 knee procedures were unilateral knee replacements (77%), followed by knee revisions (10%), partial knee replacements (9%) and bilateral knee replacements (4%).
Numbers of procedures and deaths by anaesthetic type, further stratified by procedure type.
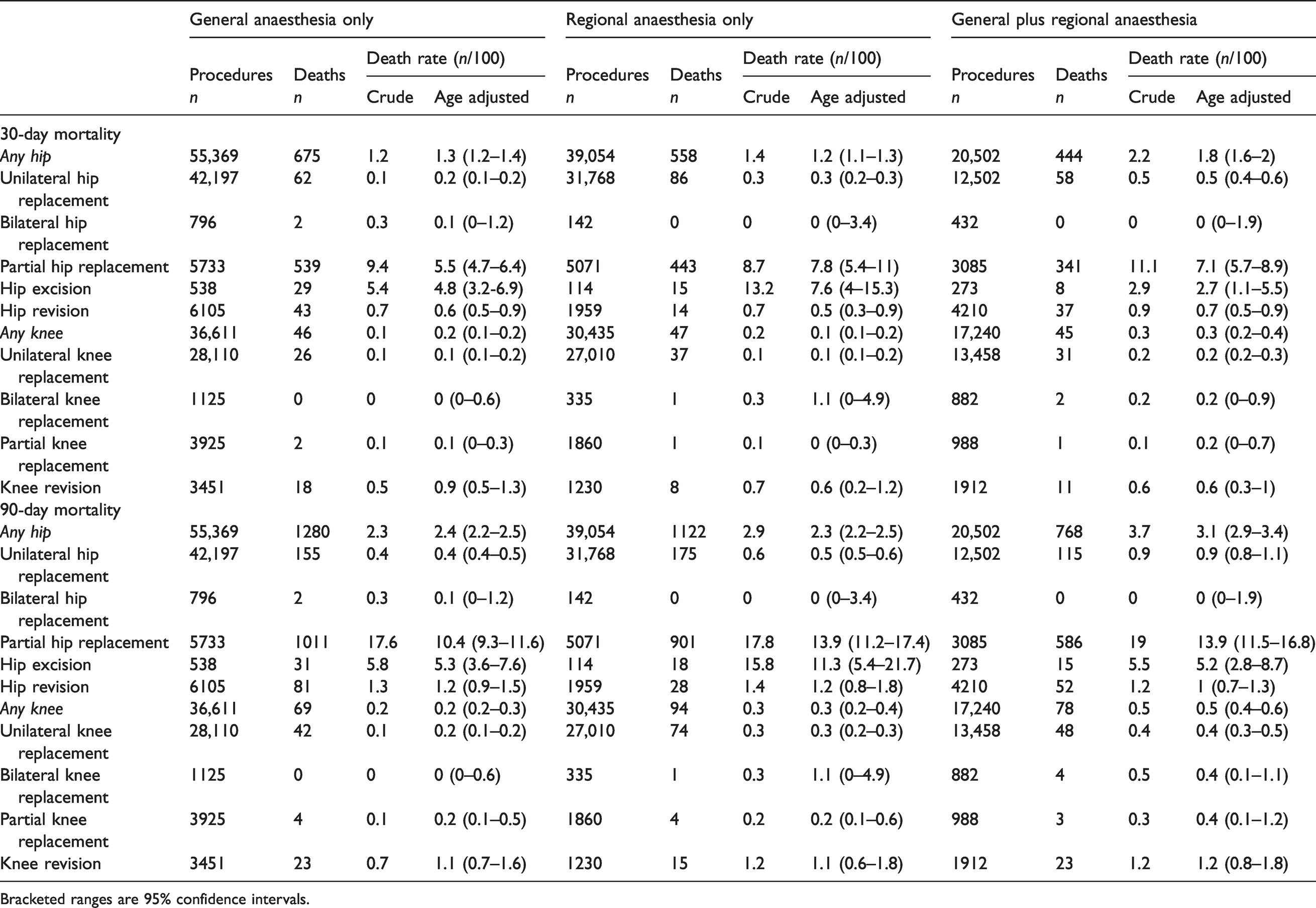
Bracketed ranges are 95% confidence intervals.
With respect to rate of postoperative death, hip procedures could broadly be described as having either a lower rate of postoperative mortality (uni/bilateral hip replacement and hip revision; age-adjusted rates 0.1–0.7 deaths within 30 days/100 procedures) or higher rate (partial hip replacement and hip excision; 4–8 deaths within 30 days/100 procedures; Table 1). The pooled ‘any hip’ rate of 30- or 90-day mortality did not reflect the mortality profile of any of the individual procedures (1.2–1.8 deaths within 30 days/100 procedures), minimising its value as a representative measure of mortality risk following hip arthroplasty. All of the individual knee procedures carried a risk of postoperative death between 0.1 and 1.1 deaths within 30 days/100 procedures.
Due to low numbers of deaths for most individual procedures, it was difficult to establish patterns of differential mortality risk between anaesthetic type and arthroplasty procedure (Table 1). However, there was some evidence of differences between anaesthesia types for unilateral hip procedures (e.g. age-standardised rate of 30-day mortality: general 0.2/100 procedures, regional 0.3/100, general plus regional 0.5/100), as well as partial hip procedures (e.g. 30-day mortality: general 5.5/100 procedures, regional 7.8/100, general plus regional 7.1/100). There was a large shift in partial hip 30-day mortality rates once adjusted for age (and little shift for unilateral hip).
The lower mortality rates seen with bilateral hip replacements (age standardised rate of 30-day mortality: general anaesthesia 0.1/100 procedures, regional anaesthesia 0/100 procedures, general plus regional 0/100 procedures) compared to unilateral hip replacements (general 0.2/100, regional 0.3/100, general plus regional 0.5/100) likely reflects the relatively young healthy cohort that are offered bilateral hip replacements.
Because most procedures had a relatively low number of deaths, we restricted our subsequent covariate-stratified analyses to those procedures that were both commonly performed and had a high absolute number of deaths within 30 or 90 days. As such, subsequent reported results are limited to unilateral hip replacements (relatively low risk of mortality but common procedure) and partial hip replacements (less common procedure but relatively high risk of mortality).
Unilateral hip replacement
For all unilateral hip procedures, general anaesthesia was most common (49%), followed by regional anaesthesia (37%). Only 14% were done with a combination of general and regional anaesthesia (Table 2). There was some variation in anaesthetic type (general, regional or general plus regional) used for unilateral hip replacements across patient subgroups. The oldest age group (>75 years) was equally split across general and regional anaesthesia for their unilateral hip replacements (41% versus 43%). In comparison, those in the youngest cohort were more likely to have general anaesthesia than a regional anaesthesia (57% versus 27%). Māori and Pacific patients were more likely to receive regional anaesthesia than the European or Asian populations (age-adjusted proportion: Māori 54%, Pacific 50%, European 37%, Asian 33%). The use of regional anaesthesia also increased with increasing levels of deprivation (e.g. NZDep quintile 1 (least deprived): 27%; NZDep quintile 5: 49%). Those with ASA scores of 1–3 were more likely to have regional anaesthesia (52%–55%) than those with an ASA score of 4–5 (44%) or no recorded ASA score (12%). There was little difference in anaesthesia type by sex, comorbidity (M3 index) or acute/elective status.
Age-adjusted proportions of general or regional anaesthesia receipt, stratified by covariates and further stratified by procedure type.
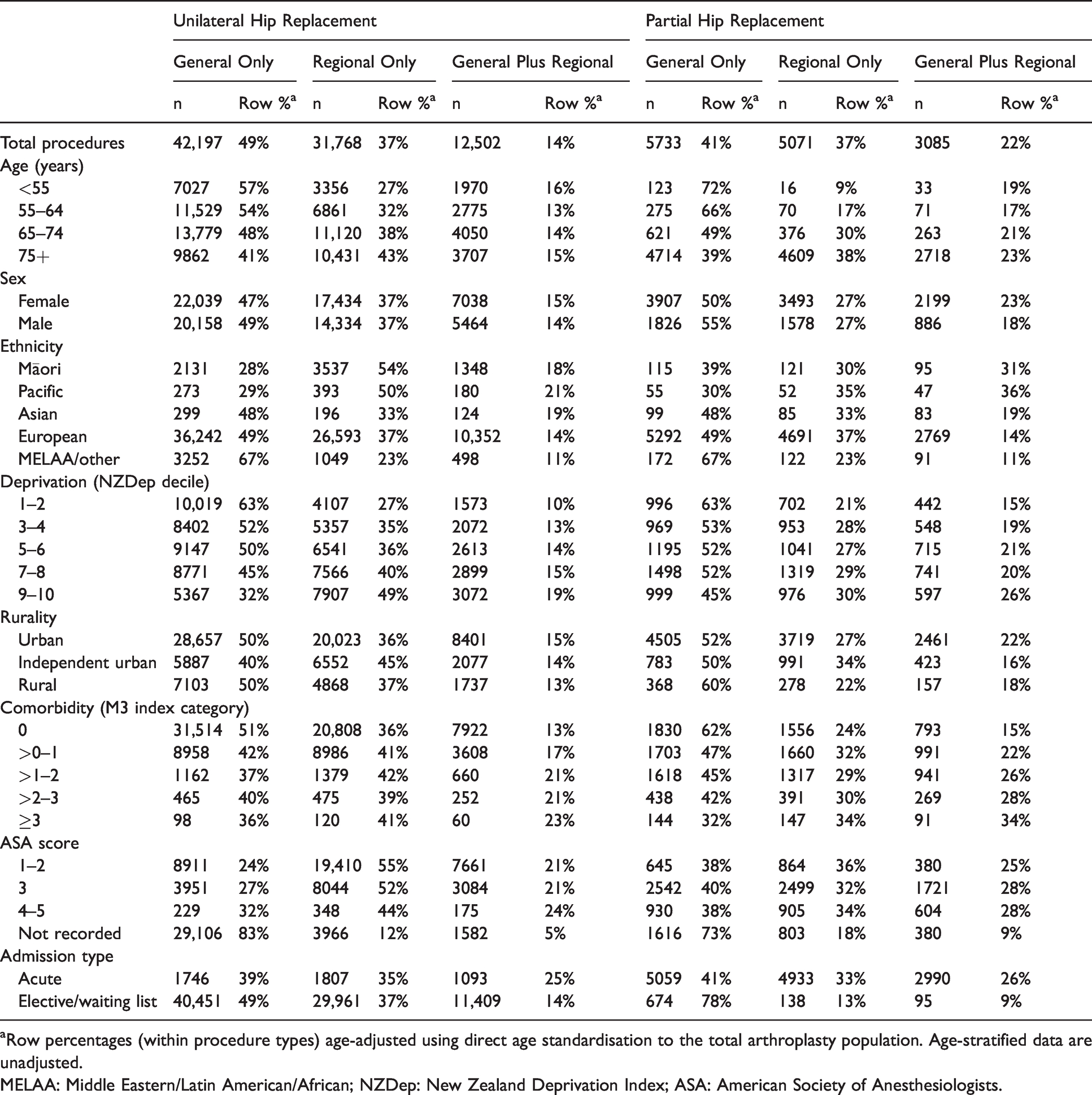
aRow percentages (within procedure types) age-adjusted using direct age standardisation to the total arthroplasty population. Age-stratified data are unadjusted.
MELAA: Middle Eastern/Latin American/African; NZDep: New Zealand Deprivation Index; ASA: American Society of Anesthesiologists.
Once adjusted for age, sex, ethnicity, deprivation, rurality, comorbidity, ASA score and admission type, there was an increased risk of 30-day postoperative mortality following unilateral hip replacement among those receiving regional anaesthesia (adjusted (adj.) HR=1.35, 95% CI 0.95 to 1.92) or a combination of general plus regional (adj. HR=1.94, 95% CI 1.32 to 2.84) compared to those receiving general anaesthesia only (Table 3). Similar patterns of higher mortality from regional and even higher mortality for the combination of general and regional compared to general anaesthesia alone were seen across strata of age, sex and deprivation (Table 3). These differences in mortality risk attenuated somewhat for 90-day mortality (regional only: adj. HR=1.11, 95% CI 0.88 to 1.40; general plus regional: adj. HR=1.53, 95% CI 1.19 to 1.98; Supplemental Material S3).
Numbers of deaths and likelihood of 30-day mortality within patient subgroups, stratified by procedure type.
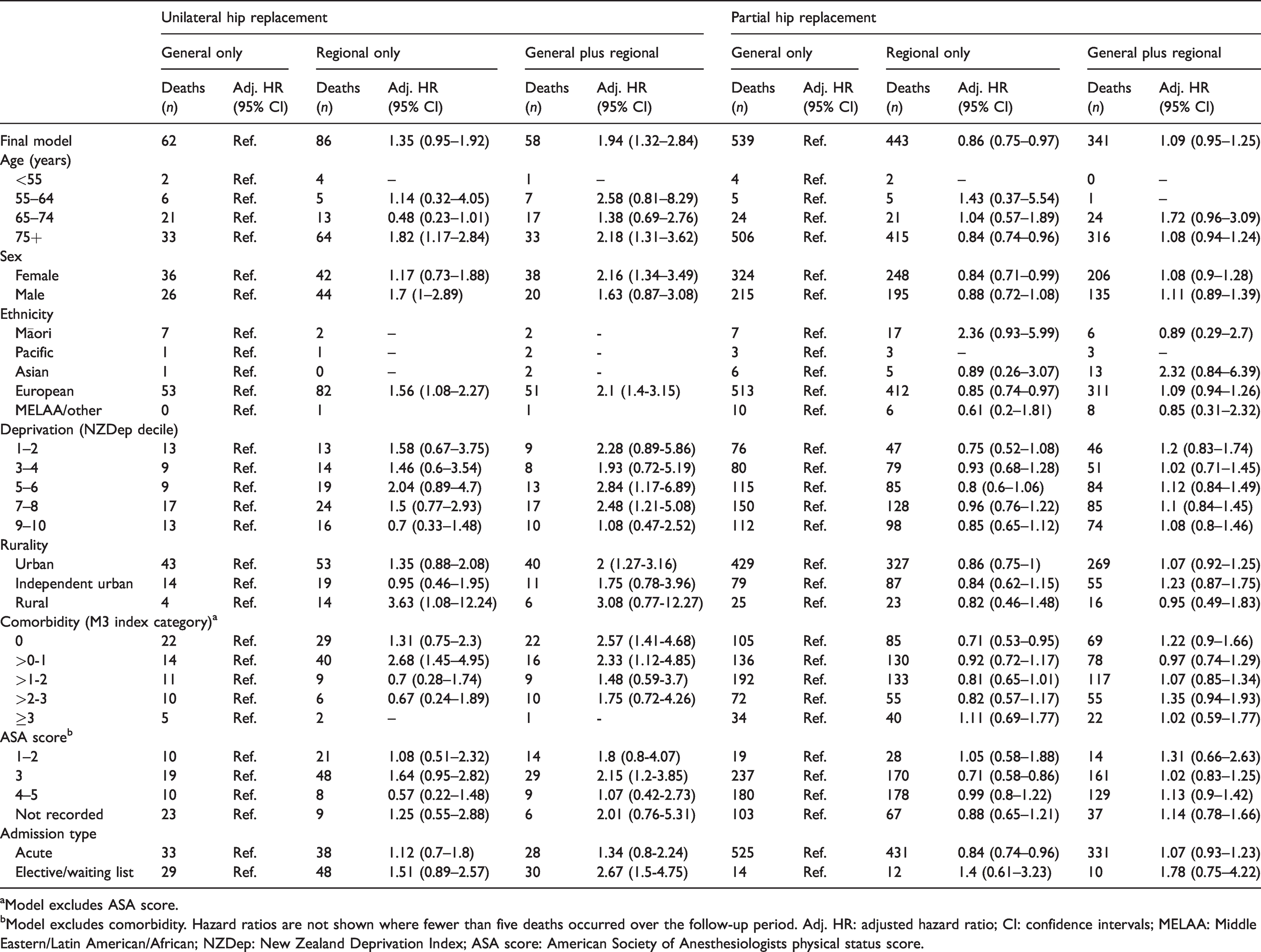
aModel excludes ASA score.
bModel excludes comorbidity. Hazard ratios are not shown where fewer than five deaths occurred over the follow-up period. Adj. HR: adjusted hazard ratio; CI: confidence intervals; MELAA: Middle Eastern/Latin American/African; NZDep: New Zealand Deprivation Index; ASA score: American Society of Anesthesiologists physical status score.
Partial hip replacement
Overall, partial hip replacements were most commonly performed under general or regional anaesthesia (41% versus 37%) and less commonly with a combination of general and regional anaesthesia (22%). The majority of partial hip replacements occurred in those aged >75 years of age, and for this age group, these were equally likely to be completed under general or regional anaesthesia (39% versus 38%) and less likely to be completed under the combination of general and regional (23%). In contrast, the small number of partial hip replacements occurring in the youngest cohort were largely done under general anaesthesia (77%), with only 9% under regional and the remaining 19% under a combination of general and regional. Māori and Pacific patients were less likely to have general anaesthesia only and more likely to have general plus regional than their European counterparts (e.g. age-adjusted proportions of general plus regional: Māori 31%, Pacific 36%, European 14%). Like unilateral hip replacement, the rate of regional only and general plus regional increased with increasing levels of area deprivation. The proportion of patients receiving general plus regional anaesthesia increased markedly with increasing comorbidity, with a corresponding reduction in general anaesthesia alone. Those admitted acutely for partial hip replacement were far more likely to have a regional only (33%) or general plus regional (26%) compared to elective/waiting list procedures (regional 13%, general plus regional 9%).
In contrast to the findings for unilateral hip replacements, overall, those receiving regional anaesthesia for partial hip replacements were around 15% less likely to die than those receiving general anaesthesia alone, after adjusting for all measured covariates (adj. HR=0.86, 95% CI 0.75 to 0.97; Table 3). There was little difference in the mortality risk between those receiving general anaesthesia alone and general plus regional anaesthesia for their partial hip replacements once adjusted for measured covariates (adj. HR=1.09, 95% CI 0.95 to 1.25). In stark contrast to the overall pattern of reduced mortality risk for regional anaesthesia for partial hip replacement, Māori had two and a half times the risk of 30-day postoperative mortality from partial hip surgery from regional anaesthesia compared to general anaesthesia after adjusting for the other measured confounders (adj. HR=2.51, 95% CI 1.16 to 5.43).
Temporal trends in anaesthetic use
Temporal trends in the use of the three anaesthetic types are shown in Figure 1 for both unilateral and partial hip replacements. For unilateral hip replacements, there was an increase in the use of both general anaesthesia alone and regional anaesthesia alone over the study period, with a corresponding substantial reduction in the use of general plus regional anaesthesia (P < 0.0001). This pattern occurred consistently across all age groups (P < 0.001; data not shown). For partial hip replacement, there was a reduction in the use of regional anaesthesia alone over time (P < 0.001), and a corresponding increase in both general anaesthesia alone (P < 0.05) and general plus regional anaesthesia (P < 0.001).
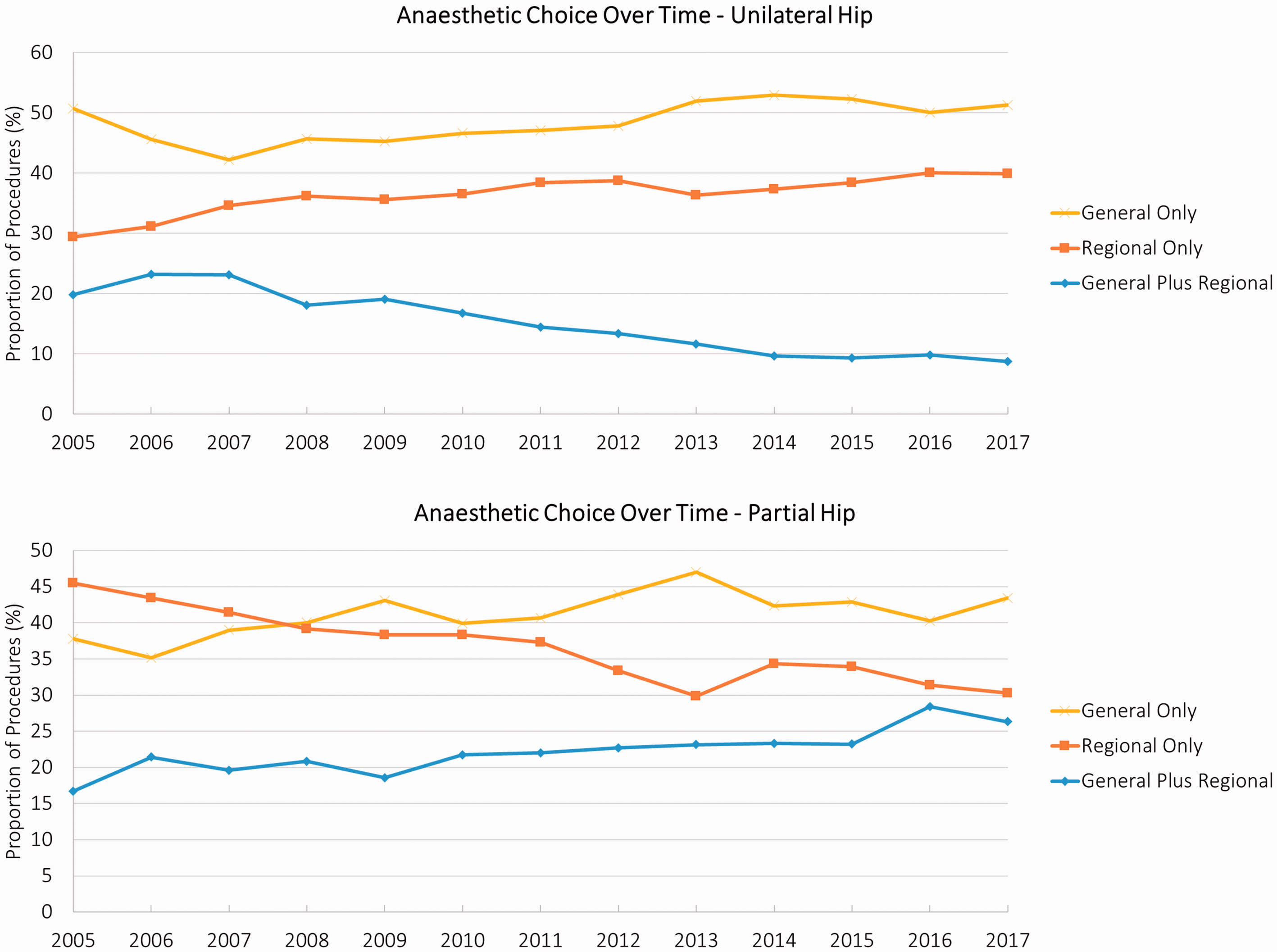
Temporal trends in anaesthetic use over time for unilateral (top) and partial (bottom) hip replacement.
Discussion
Using national-level data in the context of universal healthcare, we found that over the 2005–2017 period, those unilateral hip replacement patients who received regional anaesthesia alone or general plus regional appeared at increased risk of 30-day mortality compared to those receiving general anaesthesia alone. In contrast, there was lower 30-day mortality among those receiving regional anaesthesia alone compared to general anaesthesia alone for partial hip replacements.
Our finding of greater risk of 30-day postoperative mortality for unilateral hip replacements under regional anaesthesia alone (adj. HR=1.35, 95% CI 0.95 to 1.92) and for those receiving a combination of general and regional anaesthesia (adj. HR=1.94, 95% CI 1.32 to 2.84) compared to general anaesthesia alone is in contrast to the findings of a previous US study of 180,000 total hip replacements by Memtsoudis et al. 10 After adjusting for similar factors to those that we adjusted for (age, sex, ethnicity, deprivation, rurality, comorbidity, ASA score and admission type), Memtsoudis et al. found evidence of elevated mortality risk among those receiving general anaesthesia alone (general versus regional (reference): adjusted odds ratio (OR)=1.28, 95% CI 0.70 to 2.37; general versus general plus regional: OR=1.55, 95% CI 0.88 to 2.70). We remain uncertain why this difference may exist, although it may be related to differences in the populations under study (e.g. the Memtsoudis study included patients from 400 select hospitals across the USA, 10 and so findings may not be generalisable to whole-population studies such as the current one). There may have been other (unmeasured) differences between the studies (including both populations and study design) that reduce the comparability of our results.
In contrast to the reduced likelihood of mortality among those receiving general anaesthesia alone for unilateral hip replacements, the evidence for partial hip replacement is mixed. We found a 14% mortality benefit for the use of regional anaesthesia alone versus general anaesthesia alone for partial hip replacements (adj. HR=0.86, 95% CI 0.75 to 0.97). This pattern was observed across most patient subgroups. A crucial exception to this was observed for Māori patients, who appeared more than twice as likely to die following regional compared to general anaesthesia (adj. HR=2.36, 95% CI 0.93 to 5.99). We note that the precision of these results will be substantially impacted by the low absolute numbers of Māori deaths following partial hip replacement (seven for general anaesthesia alone; 17 for regional anaesthesia alone). They are a further suggestion that the Māori experience of postoperative outcomes contrasts to that encountered by other New Zealanders. By way of background, we know that Māori have higher postoperative mortality following hip arthroplasty than non-Māori (adjusted OR=2.60, 95% CI 1.20 to 5.62), 20 with this higher postoperative mortality occurring across many other procedure types, including acute and elective coronary artery bypass graft21 and acute and elective colorectal procedures.20,22 The differential mortality experience of Māori receiving regional anaesthesia alone (compared to Māori receiving general anaesthesia alone) may indicate that the factors that could impart a protective effect among those receiving regional anaesthesia–such as reduced risk of postoperative infection, 2 –5 unplanned intubations, 6 blood transfusion,5,7 stroke, cardiovascular and other pulmonary complications2,6–are not equally shared by Māori receiving regional anaesthesia. There may also be differential perioperative management of comorbid conditions among those Māori receiving regional anaesthesia (compared to those receiving general), as well as differential surgeon or anaesthetist experience and the overall quality of perioperative care received among these patients. These factors require further focused investigation.
We note that our overall observations of an apparent association with lower mortality with regional anaesthesia alone contrast with two recent systematic reviews and meta-analyses of hip fracture procedures, where the authors found either no difference between anaesthesia type in terms of 30-day mortality 23 or a marginal mortality benefit to general anaesthesia (pooled OR=1.15, 95% CI 1.01 to 1.32). 24 However, the authors of the latter review warned that the included studies had a high risk of confounding. This is relevant when we consider that, in our own study, 30-day mortality was higher for regional (7.8/100) compared to general anaesthesia (5.5/100; crude rate ratio 1.4) before we adjusted for the confounding impact of our included covariates. The two randomised controlled trials that were included in their review 24 found a similar protective effect of regional anaesthesia as found in our study, although statistical precision was impacted by small sample sizes (pooled OR=0.74, 95% CI 0.26 to 2.14). We note that a larger randomised controlled trial entitled REGAIN (REgional versus General Anesthesia for promoting INdependence after hip fracture) is currently underway, 25 which has mortality as a secondary outcome and should be reporting in late 2021.
Temporal trends in anaesthetic use
For unilateral hip replacement, the use of general anaesthesia alone and regional anaesthesia alone increased substantially over the study period, while the use of general plus regional anaesthesia dropped. In light of the apparent increased mortality risk of general plus regional anaesthesia compared to general anaesthesia, this temporal shift appears in keeping with best practice. By contrast, the apparent reduced likelihood of mortality with regional anaesthesia alone for partial hip replacement is at odds with the clear and substantial temporal shift towards increased use of general anaesthesia for this procedure over our study period (either alone or in combination with regional anaesthesia). Since we have adjusted for age and comorbidity within our analysis, this temporal shift should not be confounded by population ageing and increased comorbid burden over time (although residual confounding is still feasible, as noted below). This temporal change towards general anaesthesia has been observed for other hip procedures and may reflect improvements in the availability of short-acting intravenous anaesthetics and laryngeal mask airway technology, and the increased use of peripheral nerve blocks. 26 In addition, the use of regional anaesthesia fixes the time available to complete the procedure from the moment it is administered, whereas this factor can be modulated when using general anaesthesia. From a morbidity perspective, this temporal change may also reflect the movement towards earlier mobilisation as part of Enhanced Recovery After Surgery (ERAS) protocols. Collectively, these factors might help to explain why we have observed a gradual movement towards general anaesthesia over time. However, the contrast between temporal trends in regional anaesthesia use for partial hip replacement and the apparent reduced likelihood of mortality for patients receiving this anaesthetic type require us to consider whether continuing this temporal trend is in the best interests of the patient. As recognised above, postoperative mortality is one perioperative factor that drives anaesthetic choice, and the protocols that govern anaesthetic choice should prioritise patient outcomes (including mortality and morbidity outcomes).
Strengths and limitations
The current study used high-quality national-level data across a relatively wide time interval, allowing us to look at both overall and temporal trends. We acknowledge that the current study does not capture within- or between-practice variation in anaesthesia use. Rather, it presents a national ‘average’. A more nuanced investigation of practice variation, and how this has changed over time, is of interest but was beyond the scope of the current study. We also acknowledge that there are other limitations to the data used for this study–for example, this study does not discern whether a given individual died of factors directly relating to their procedure, their underlying comorbidities or other reasons.
While our study includes data for a number of important confounding factors, including level of comorbidity, it is possible that we have not adequately controlled for potentially important differences between anaesthesia groups in terms of factors that might independently influence mortality risk. Factors such as surgeon and anaesthetist experience and techniques, as well as preoperative optimisation and the quality of postoperative care (including perioperative blood pressure management), 27 could vary between groups, and this will not have been captured within our study.
Conclusions
In a national study of nearly 200,000 hip and knee replacement procedures conducted between 2005 and 2017, we found some key differences in the risk of postoperative mortality between those receiving general anaesthesia only, regional anaesthesia only and general plus regional anaesthesia. We found that those receiving regional alone or general plus regional for unilateral hip replacement appeared at increased risk of 30-day mortality compared to those receiving general anaesthesia, even after adjusting for differences between anaesthesia groups in terms of age, ethnicity, deprivation, rurality, comorbidity, ASA score and admission type (e.g. general plus regional: adj. HR=1.94, 95% CI 1.32 to 2.84). By contrast, we observed lower 30-day mortality among those receiving regional anaesthesia alone compared to general alone for partial hip replacements (adjusted HR=0.86, 95% CI 0.75 to 0.97). This finding is at odds with declining temporal trends in the use of regional anaesthesia alone for partial hip replacement procedures. However, we recognise that postoperative mortality is one perioperative factor that drives anaesthetic choice. Protocols that govern anaesthetic choice should prioritise patient outcomes, including mortality and morbidity.
Footnotes
Author Contribution(s)
Acknowledgements
We would like to acknowledge Chris Lewis from the Ministry of Health’s National Collections team for assistance with data extraction.
Declaration of conflicting interests
The authors declare no competing interests.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by the Health Research Council of New Zealand (HRC reference # 18/037).
Supplemental material
Supplemental material for this article is available online.