
Abstract
Veno-venous extracorporeal membrane oxygenation is increasingly used for severe but potentially reversible acute respiratory failure in adults; however, there are limited data regarding long-term morbidity. At our institution, most patients requiring veno-venous extracorporeal membrane oxygenation have been followed up by a single physician. Our primary aim was to describe the serial long-term morbidity for respiratory, musculoskeletal and psychological functioning.
A retrospective audit of inpatient and outpatient medical records was conducted. A total of 125 patients treated with veno-venous extracorporeal membrane oxygenation for primary respiratory failure were included. The patients were young (mean (standard deviation) age 43.7 (4.1) years), obese (mean (standard deviation) body mass index 30.8 (10.4) kg/m2), and mostly were male (59%). Most patients (60%) had no comorbidities.
The survival rate to discharge was 70%, with body mass index and the number of comorbidities being independent predictors of survival on multiple logistic regression analysis. Over half (57%) of the Australian survivors had regular outpatient follow-up. They had a median of three reviews (range 1–9) over a median of 11.8 months (range 1.5-79) months. Breathlessness and weakness resolved in most within six months, with lung function abnormalities taking longer to resolve. Over half (60%) returned to employment within six months of discharge. Over a quarter (29%) displayed symptoms of anxiety, depression or post-traumatic stress disorder.
Keywords
Introduction
Acute respiratory failure in adults is conventionally managed with positive pressure ventilation. Extracorporeal membrane oxygenation (ECMO) uses the principles of cardiopulmonary bypass to provide gas exchange, allowing lower ventilation settings and thus less trauma to the lungs caused by mechanical ventilation. 1 This technique has been used to treat respiratory failure in infants and children since 1990; however, it was not until the influenza-A (H1N1) pandemic in 2009 that it became more widely used for adults. 2
The data on long-term outcomes for these patients are limited, and mostly include assessments at a single timepoint.3–13 There are three studies14–16 with serial outpatient assessments; however, the results are presented as a combined population of both veno-arterial (V-A) and a smaller proportion of veno-venous (V-V) ECMO patients. A recent integrative review 17 found that patients treated with V-V ECMO for respiratory failure tended to be younger and had a trend towards slightly higher Health-Related Quality of Life (HRQoL) scores compared with patients treated with V-A ECMO for cardiogenic shock, which may confound these results from a mixed population. As such, we aimed to retrospectively examine the patients treated with V-V ECMO for acute respiratory failure at Royal Prince Alfred Hospital from 2005 to 2019. All patients at our institution who have undergone V-V ECMO for severe acute respiratory failure were followed up by a single specialist in both respiratory and critical care medicine. This included the subjective assessment of dyspnoea, functional limitation and psychological symptoms as well as a comprehensive clinical examination, including neurology and serial lung function.
Through this audit we hope to add to the understanding of the long-term sequelae of V-V ECMO patients and how this changes following hospital discharge. Our primary aim was to describe the long-term morbidity for respiratory, musculoskeletal and psychological functioning, and to describe any trends from serial measurement. Our secondary aims were to describe the demographics and inpatient characteristics of patients treated with V-V ECMO for severe respiratory failure and to compare those to the international literature. Our hypothesis is that although survivors have significant disability at the time of hospital discharge, they improve over time to have minimal disability and good functional status.
Methods
This single-centre retrospective study was conducted at the Royal Prince Alfred Hospital, Sydney, Australia, following approval from the local human research ethics committee. The need for informed consent for the retrospective collection of inpatient and outpatient data was waived.
We studied all patients who had received V-V ECMO (Cardiohelp System, Getinge, Germany) for primary respiratory failure at our institution, since the programme’s inception in August 2005 until February 2019. This included patients who were commenced on ECMO at another institution by our retrieval team and then transported on ECMO to our institution. Patients were retrospectively identified from the institution’s prospective ECMO database. Patients were excluded if V-V ECMO was used intra-operatively or postoperatively (except when the indication was aspiration during induction of anaesthesia), as a bridge to transplantation, or following significant chest trauma. Patients were also excluded if they were less than 18 years of age at the time of admission to hospital.
There were two components to this study: the review of inpatient medical records for all patients who received V-V ECMO and met the inclusion criteria; and the review of outpatient medical records, correspondence, and investigation results for those patients who had at least one outpatient appointment recorded.
Inpatient data
Patients’ inpatient medical records were reviewed for demographic details, diagnosis (patients classified as to their primary diagnosis, i.e. viral pneumonia with subsequent bacterial infection were classified as viral pneumonia), pre-ECMO details (including mechanical ventilation, gas exchange and Murray score), ECMO details (including cannulation and ECMO-specific complications), intensive care unit (ICU) details (including use of renal replacement therapy, tracheostomy, development of critical illness neuromyopathy or delirium) and hospital outcomes (including survival and discharge destination).
All patients commenced on V-V ECMO, either in hospital or by the retrieval team, were cannulated percutaneously by serial dilation, with transoesophageal echocardiographic (Sparq system; Philips, Amsterdam, The Netherlands) and vascular ultrasound (Acuson Freestyle; Siemens, Munich, Germany) guidance. Four cannulation configurations were used over the 14-year period: (a) femoral–femoral (HLS Cannulae, Getinge, Gothenburg, Sweden); (b) femoral–jugular (HLS Cannulae, Getinge, Gothenburg, Sweden); (c) single bicaval dual lumen cannula (Avalon Elite, Getinge, Gothenburg, Sweden); and (d) femoral plus jugular–femoral (high flow multi-cannulae bicaval access; HLS Cannulae, Getinge, Gothenburg, Sweden). Most patients received inpatient Doppler ultrasounds (Logiq E9; GE Healthcare, Chicago, IL, USA) of cannulation sites and distal limbs to assess for thrombosis or vascular damage prior to discharge.
Outpatient data
At our institution, all patients who are treated with V-V ECMO for primary respiratory failure are admitted under a single physician, trained in both respiratory and critical care medicine. This physician is involved in patient care while they are in intensive care and then on the hospital ward. All patients who survive to hospital discharge, including those retrieved from another hospital within Australia, are provided with an outpatient appointment with this physician. Time from hospital discharge was recorded along with serial information on patient-reported symptoms. Although no standardised forms were used, the same clinician was assessing and documenting serial information on all patients.
Symptoms in the domains of respiratory, musculoskeletal and general functioning were discussed. A physical examination of the chest as well as power and sensation in the upper and lower limbs was performed. No formal cognitive assessment was performed; however, the time from hospital discharge to the patient returning to their previous employment was recorded. Spirometry was either performed in the office using a Pony FX desktop spirometer (COSMED, Rome, Italy) or in the hospital laboratory (CPFS/D; MGC Diagnostics, Saint Paul, MN, USA) using global lung initiative predictors for height, race and gender. Nerve conduction studies were performed if clinically indicated.
Statistical analysis
Continuous variables were expressed as mean and standard deviation (SD) if normally distributed, or median and interquartile range (IQR) or range if non-normally distributed. Multiple logistic regression was used to assess the associations between survival and categorical and continuous predictive variables. Longitudinal follow-up data were analysed using Kaplan–Meier analysis. Prism 9 for macOS (version 9.1.1 (223) 16 April 2021, GraphPad) was used for analysis and P< 0.05 was considered statistically significant.
Results
A total of 158 patients were treated with V-V ECMO from August 2005 until February 2019 at our institution. Thirty-two patients were excluded (Figure 1). An additional patient treated with V-V ECMO in 2005 had their inpatient paper medical record unavailable for review. Thus 125 adult patients treated at our institution with V-V ECMO for primary respiratory failure over a 14-year period were analysed.
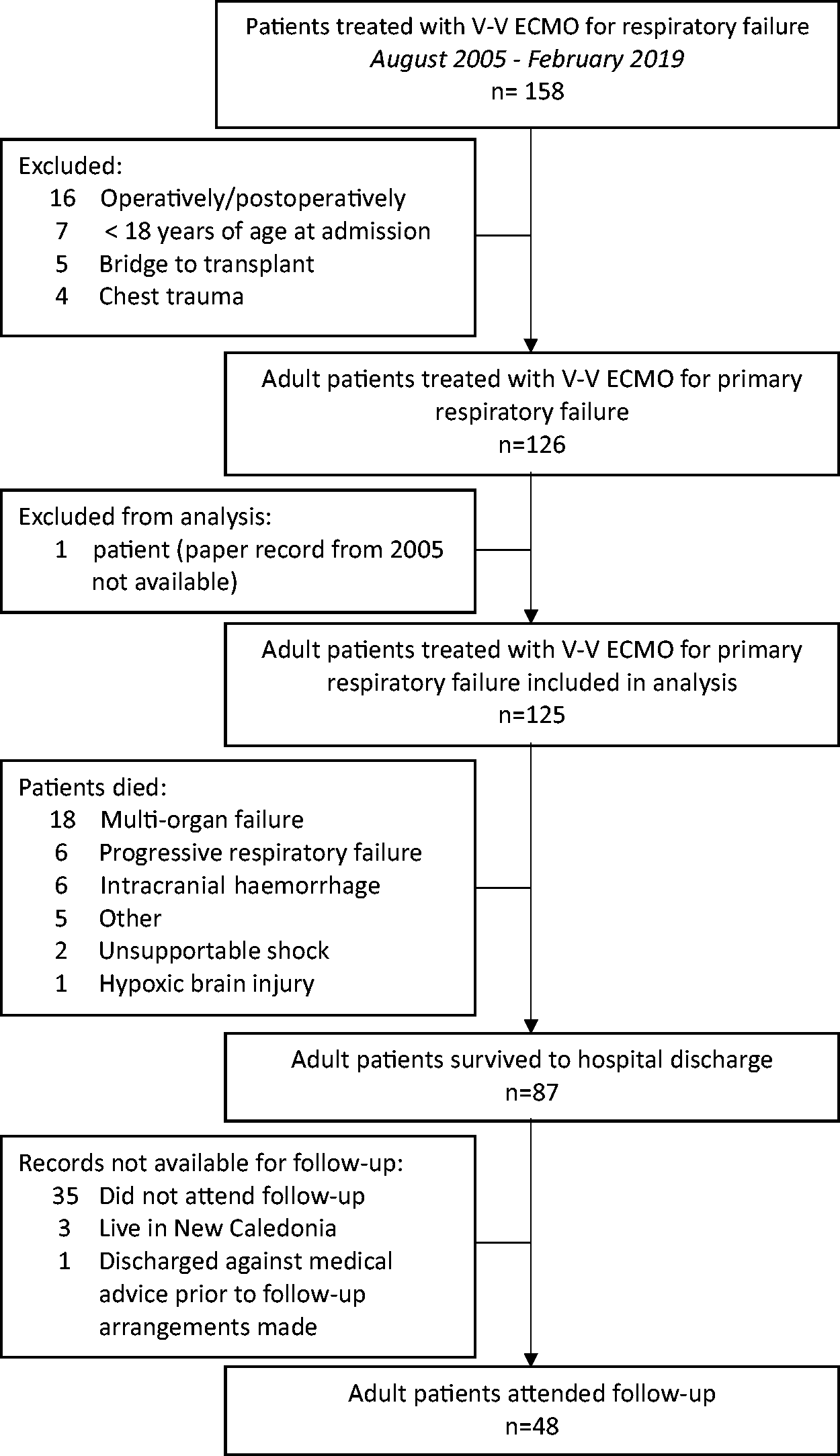
Flow diagram.
The average age of our cohort was 43.7 (14.1) years, they were obese with an mean (SD) body mass index (BMI) of 30.8 (10.4) kg/m2, (n=120), and and over half were male (Table 1). Most patients (60%) had no medical comorbidities.
Demographics of patients treated with veno-venous extracorporeal membrane oxygenation for primary respiratory failure.
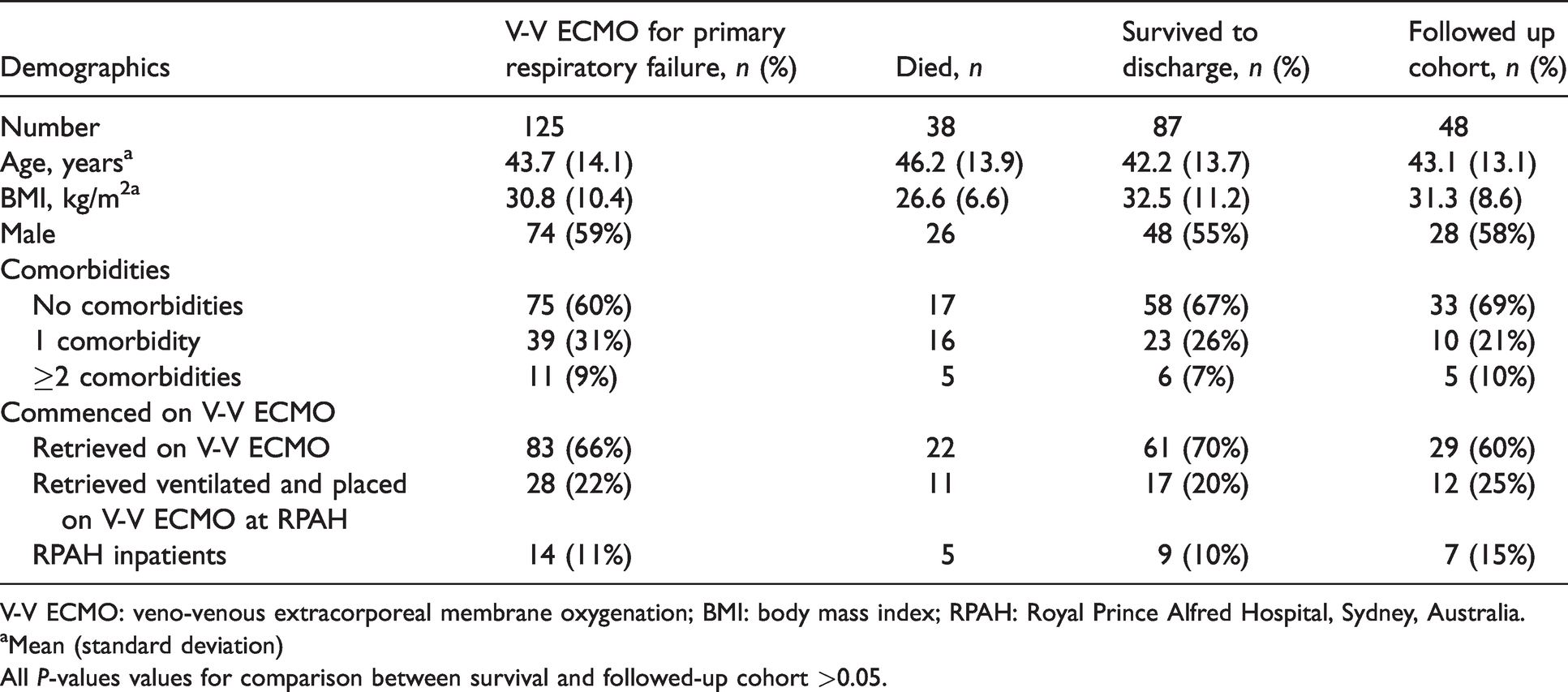
V-V ECMO: veno-venous extracorporeal membrane oxygenation; BMI: body mass index; RPAH: Royal Prince Alfred Hospital, Sydney, Australia.
aMean (standard deviation)
All P-values values for comparison between survival and followed-up cohort >0.05.
The most common indications for V-V ECMO were viral pneumonia (39%; 33/49 patients had influenza A (H1N1)) and bacterial pneumonia (36%; 10/45 had Streptococcus pneumoniae) (Table 2).
Survival of patients according to aetiology of respiratory failure.
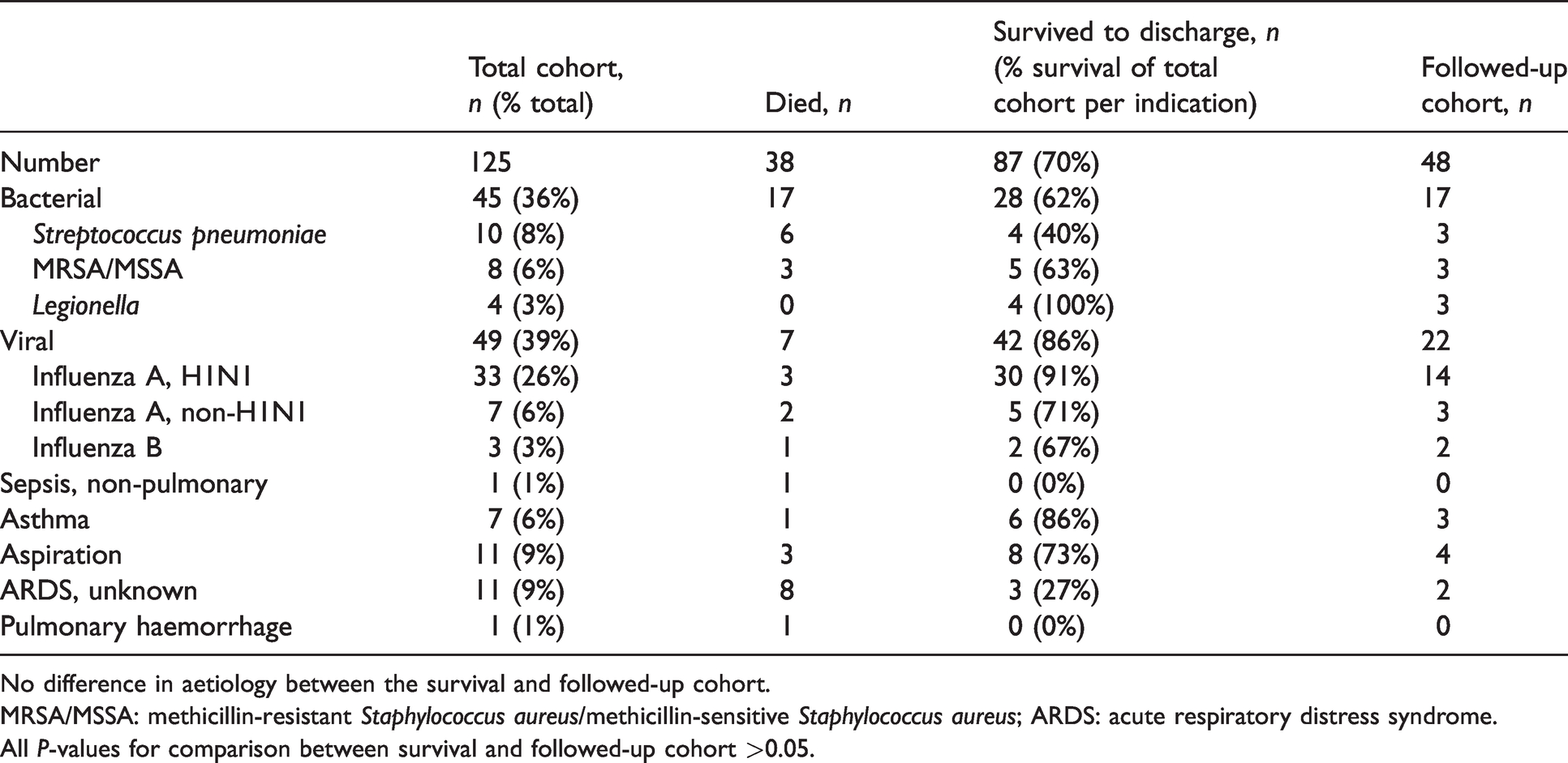
No difference in aetiology between the survival and followed-up cohort.
MRSA/MSSA: methicillin-resistant Staphylococcus aureus/methicillin-sensitive Staphylococcus aureus; ARDS: acute respiratory distress syndrome.
All P-values for comparison between survival and followed-up cohort >0.05.
Only BMI and the number of comorbidities were significantly associated with survival in the multiple logistic regression analysis. Patients’ probability of survival from the logistic model is equal to e^X/(1+e^X) where X = –1.02 + 0.08*BMI–0.6*(number of comorbidities). For every increase of 1 kg/m2 in BMI the odds of surviving increased 1.1 (95% confidence intervals (CI) 1.03 to 1.16) and for every additional comorbidity the odds of surviving decreased 0.5 (95% CI 0.30 to 0.89) (area under the receiver operating characteristic curve (ROC AUC) 0.70, 95% CI 0.60 to 0.81, P < 0.0005). Age, gender and aetiology of respiratory failure were not independent predictors of survival.
Patients were ventilated for a median of 1.6 (IQR 0.7–four) days prior to ECMO and had severe lung injury with a median ratio of arterial partial pressure of oxygen to inspired fractional concentration of oxygen of 65 (IQR 52–82) and median Murray score of 4 (IQR 3–4). They were on ECMO for a median of eight (IQR five–13) days, ventilated for 21 (IQR 11–31) days, had an ICU length of stay of 27 (IQR 16–37) days and hospital length of stay of 35 (IQR 20–48) days. There was no difference in survival for those treated with prolonged ECMO (
Significant outcomes occurring both in the ICU and on the hospital ward are shown in Table 3. Thirteen of 85 patients (15%) were found to develop an unexplained sinus tachycardia, with a normal echocardiogram, that persisted to hospital discharge. The development of the tachycardia was not associated with the patients’ length of time on ECMO or in the ICU.
Intensive care and hospital ward outcomes.
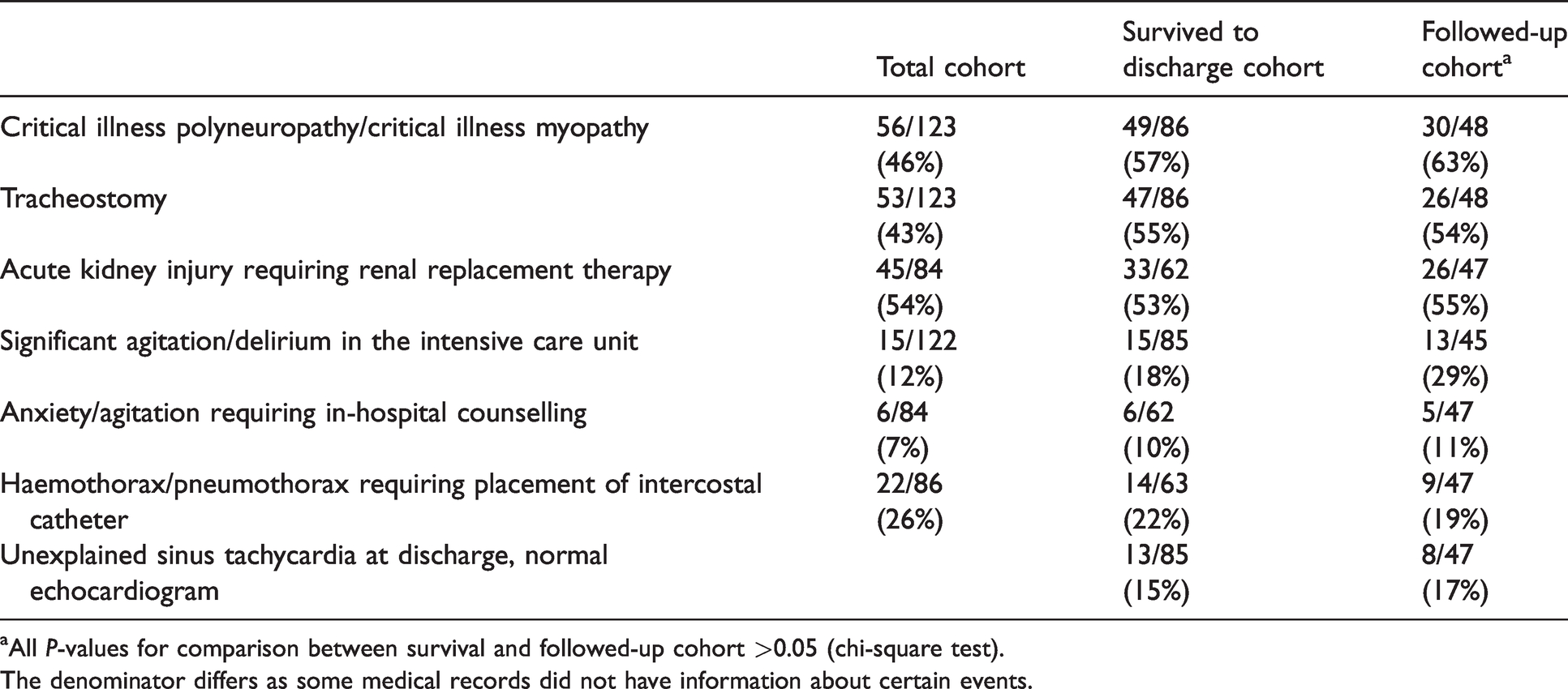
aAll P-values for comparison between survival and followed-up cohort >0.05 (chi-square test).
The denominator differs as some medical records did not have information about certain events.
One patient was transferred to their referral hospital still intubated. Seventy percent of patients were discharged from the ICU alive, and all then survived their hospital admission. Of those that survived to hospital discharge 41% were discharged directly home, 44% to another acute hospital, 14% to a rehabilitation hospital and 1% were against medical advice.
Outpatient data
Of the 87 patients who survived to discharge, 84 patients live in Australia and 48 (57%) patients had regular outpatient appointments. They had a median of three (range 1–9) reviews over a median of 11.8 (range 1.5–79) months. The followed-up cohort was similar to the survival cohort in terms of demographics (Table 1) as well as rates of ECMO complications and ICU outcomes (Table 3).
Figure 2 shows the probability of the resolution of respiratory, musculoskeletal and neurological symptoms and signs as expressed as a function of time from hospital discharge.
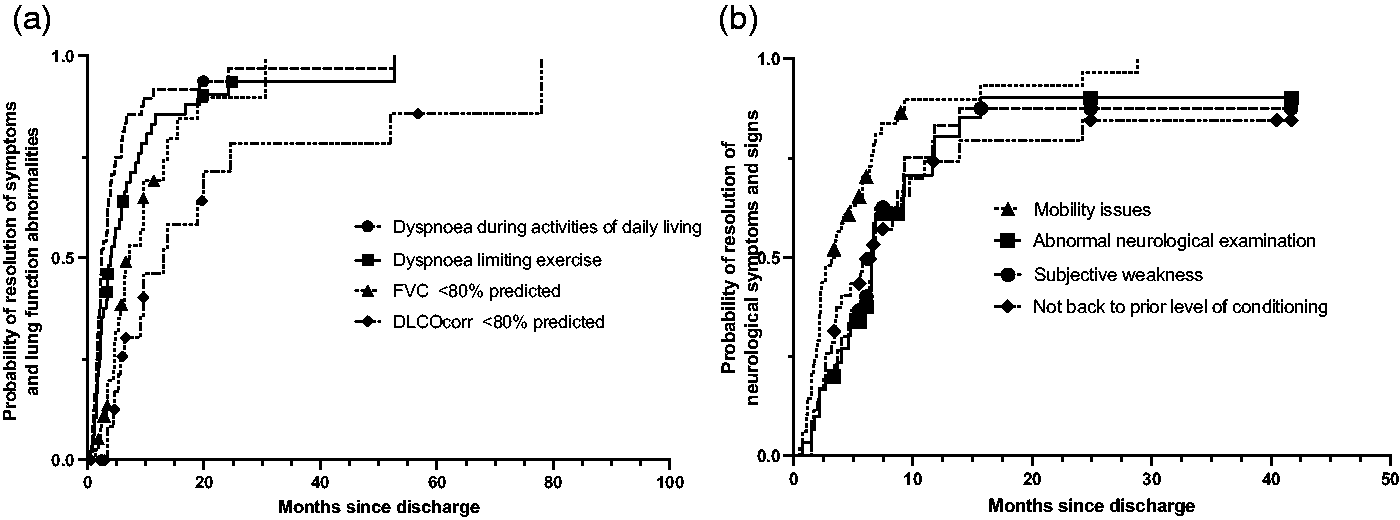
Probability of the resolution of symptoms and signs as a function of time since discharge from hospital. (a) Probability of freedom from respiratory symptoms and lung function abnormalities. (b) Probability of freedom from neurological and musculoskeletal symptoms and signs. Kaplan–Meier analysis. Censored points are shown and indicate the presence of ongoing abnormalities at the time of final outpatient appointment.FVC, Forced vital capacity. DLCOcorr, Diffusion Capacity For Carbon Monoxide Corrected For Haemoglobin.
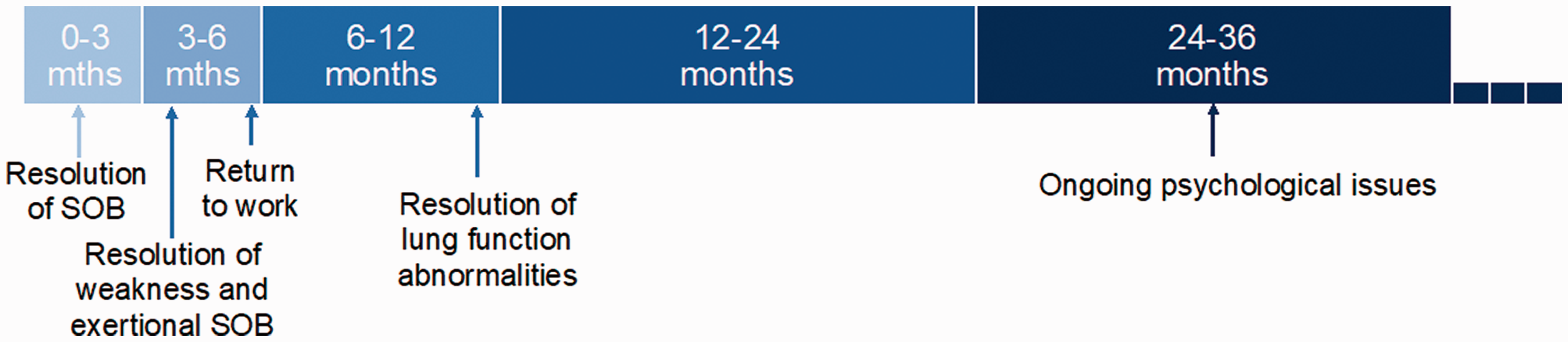
Median time to resolution of symptoms and signs in the domains of respiratory, musculoskeletal and neurological functioning. SOB = shortness of breath.
Cardiac arrhythmias occurred in 10 (21%) of our followed-up cohort. An unexplained tachycardia was present in eight (17%) of our followed-up patients at discharge with seven of these eight patients (88%) having resolved the tachycardia with no cause found at a median of 6.1 (range 1.5–15.9) months. One further patient developed new atrial fibrillation and required warfarin and direct current cardioversion. Another had several episodes of supraventricular tachycardia requiring successful ablation.
Data regarding employment were available for 32 patients. Nine patients (28%) were pre-morbidly unemployed or retired and remained so following their admission. Of the 23 patients who were previously employed, 19 patients (83%) had returned to any work at a median of 5.5 (range 1.2–17.5) months, with 16 patients (70%) returning to full-time employment at a median of 5.6 months. Four patients (17%) who were previously employed had not returned to work by a median of 17.6 months.
A total of 14/42 (33%) of patients had symptoms of anxiety, depression or post-traumatic stress disorder (PTSD) identified by the physician, with six of these patients (43%) having a previously documented history of anxiety or depression. There was no relationship found between the presence of these symptoms and the time in the ICU, time on ECMO, presence of ICU delirium or agitation or the need for in-hospital counselling. Symptoms were still present in all these patients at their last review up to 54 months following discharge.
Discussion
This retrospective review is to characterise serial long-term outcomes following discharge in the domains of respiratory, neurological and musculoskeletal functioning as well as mental health for patients who have undergone V-V ECMO for primary respiratory failure (Figure 3).
Our patients tended to have resolution of dyspnoea with their activities of daily living within the first three months following discharge, and resolution of exertional dyspnoea by six months, with lung function abnormalities taking longer to resolve (see Figure 3). These findings are consistent with other studies assessing lung function and symptoms using the St George’s Respiratory Questionnaire (SGRQ), 3 with ECMO survivors having improved SGRQ compared with conventionally ventilated patients at 12 months, 3 but still higher than normal subjects with no known respiratory disease. 18 However, diffusion capacity of the lungs for carbon monoxide (DLCO) has been shown consistently to take longer to resolve with 75% of 37 H1N1 survivors (12 ECMO, 25 conventional ventilation) having a reduced DLCO with similar outcomes between the groups. 7 Another study of 38 V-V ECMO patients at a median of nine years following discharge described a decreased DLCO in 47%. 12 This is also the most common residual impairment described in conventionally treated acute respiratory distress syndrome (ARDS) patients, described in up to 80% of patients at a year following discharge. 19
Neurological problems related to intensive care stay were common but resolved in most of our patients by seven months following discharge. This is consistent with a Taiwanese qualitative study of 14 ECMO patients (11 V-A ECMO, three V-V ECMO) that found on serial semi-structured interviews that half experienced lower limb weakness or paraesthesia during the first six months, with most resolving by six months. 14 An Australian study again looking at a combined V-V and V-A ECMO population showed 39% had persistent problems with mobility and usual activity as measured by the EQ-5D-5L (EuroQol) at a median of 606 days following discharge. 16 The only other study to perform clinical examinations on patients examined the muscular strength of 25 non-ECMO and 12 ECMO ARDS survivors at a year following discharge and found no difference between the groups and no significant muscle weakness (Medical Research Council scores <48). 7 All patients were walking without an aid in 38 ECMO patients at a median of nine years following discharge. 12
Most of our patients who were previously employed returned to employment (83%), and did so at a median of 5.5 months. These levels of employment are similar to three European studies. A Swedish study of 21 ECMO patients showed 76% were back in their former occupation at a median of 26 months. 6 A French study of H1N1 survivors (12 ECMO, 25 non-ECMO H1N1) showed 83% returned to work at a median of 4.2 (2.6–8.3) months following discharge. 7 The PRESERVE trial (PRedicting dEath for SEvere ARDS on VV-ECMO), a French multicentre study, showed 41/57 (72%) of patients had returned to work, with 52% at their prior level of work at six months following discharge. 10 An Australian study of 15 V-V ECMO survivors at a median of 8.4 (6–16) months following discharge, showed 52% had returned to work, with only 26% to their prior work levels. 4 Interestingly, all patients in the study described bilateral limb weakness that continued beyond discharge, and may have represented a population with more significant sequelae from their treatment with ECMO. A more recent Australian study showed that 20/33 ECMO (mixed V-V and V-A population) patients were in prior employment, and of them 19 (95%) returned to work between 12 months and six years following discharge. 16
A third of our patients (33%) were identified as having symptoms consistent with anxiety, depression or PTSD. A Swedish cohort showed similar rates of anxiety (22%), depression (14%) and symptoms of PTSD (14%) on the Hospital Anxiety and Depression Scale (HADS, Swedish version) and the Trauma Screening Questionnaire (Swedish version); this was screened for at a median of nine (range 3.1–17.1) years following discharge, 12 and may relate to improvements over time. In the large PRESERVE trial, anxiety, depression and PTSD symptoms were reported by 34%, 25% and 16% of patients, respectively, using the HADS and Impact of Event Scale at six months following ICU discharge. 10 Despite this our rates are likely to be an underestimate of the true burden of mental health problems for these patients. A recent prospective study over seven years in Italy assessed 33 ECMO survivors at a median of 2.7 years following hospital discharge with the 36-Item Short Form (SF-36) health survey questionnaire and found high rates of mental health problems in both the patients and their caregivers. Anxiety was found in 42% of patients and 39% of carers, depression in 39%–42% patients and 39%–52% of caregivers and interestingly PTSD in 47% of patients but 61% of caregivers. 9
Our ECMO population had an overall survival to discharge rate of 70%, which is in line with the latest Extracorporeal Life Support Organisation Registry data of 60%, published in July 2020. 20
Of interest was the relatively high prevalence of ongoing new cardiac arrhythmias among our V-V ECMO survivors and followed-up cohort. In particular, a new sinus tachycardia, with a normal transthoracic echocardiogram, that was prolonged until at least hospital discharge was seen in 13 of 85 (15%) hospital survivors and eight of 47 (17%) followed-up patients. Although these patients’ heart rates did decrease with time, they did so at a median of 6.1 (range 1.5–15.9) months. A prolonged elevated heart rate has been variably shown to be associated with decreased survival in acutely ill patients in the ICU; 21 , 22 however, its presence beyond hospital discharge has not been investigated to our knowledge.
There are several limitations to our study including it being from a single centre, the lack of standardised forms for outpatient assessment, and only 55% survivors followed up. However, despite this the results appear to be consistent with other studies that have used HRQoL forms, indicating that the use of a single physician assessing the same patients over time ensures uniformity of result reporting. Ultimately, our results would need to be tested in larger multicentre prospective outpatient programmes using standardised testing and forms to assess the respiratory, musculoskeletal and neurological, as well as mental health of these patients.
Conclusions
This is the largest serial study to our knowledge of a pure V-V ECMO for primary respiratory failure population followed up to assess the long-term outcomes in several domains. It emphasises the complex medical nature and varying ongoing physical and mental health complaints that arise from this rescue treatment. Despite this, the clear majority of patients at one year following discharge had managed to resume their normal life following such a critical illness admission. Our results highlight the need for long-term medical review of these patients up to at least a year following discharge by clinicians familiar with the nuances of ECMO and its effect on the body and mind.
Footnotes
Author contributions
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.