
Abstract

Clinicians may wish to assess differences in diaphragmatic excursion between the right and left lung at the point of care, in order to exclude diaphragmatic pathology (e.g. phrenic nerve palsy), particularly if a chest X-ray is not available. We conducted an exploratory study comparing the accuracy of lung auscultation against lung ultrasound for point-of-care assessment of the extent of basal lung excursion during maximal inspiration (Austin Human Research Ethics Committee approval LNR/21/Austin/19). A height difference of more than one intercostal space (ICS) between diaphragmatic domes during maximal inspiration on chest X-ray is a commonly used ‘rule of thumb’ suggesting reduced basal lung ventilation on the affected side. 1 We compared the most caudad point of audible breath sounds by stethoscope auscultation to the most caudad point of visible ‘sliding lung’ sign using B-mode ultrasound (US) at the bases of both lungs on 25 healthy consenting volunteers at maximal inspiration, along bilateral parallel lines drawn on the skin at 5 cm from the line of the spinous processes (Figure 1). This most caudad point of visible ‘sliding lung’ sign is known as the ‘lung point’ when used to diagnose pneumothorax, defining an interface at which mobile apposition of the parietal and visceral pleura is lost. US was considered the reference standard for data analysis. Anecdotally, we had previously observed that US detected reduced basal lung expansion by loss of lung point descent and a more cranial lung point at maximal inspiration in two patients scanned pre and post interscalene block. To identify a reference height difference comparable to measurements using a chest X-ray, we measured the perpendicular height of the ICS at the ICS cranial to the lung point in each volunteer. Measurements were taken from the cranio-caudal midline of the stethoscope bell at the last point where breath sounds were heard and at the cranio-caudal midline of the linear ultrasound probe (Sonosite X-Porte HFL38xi; Fujifilm Sonosite, Bothell, WA, USA) where the lung point was seen at the centre of the US sector. Our primary outcome measure was quantification of bias and precision between the two methods; secondary outcome measures were agreement between methods on which side had the most caudad diaphragmatic excursion, and comparison of the height difference between sides when measured by both methods. All volunteers had bilateral descent of the lung point during inspiration. Auscultation assessed most caudad lung ventilation at mean (standard deviation, SD) 2.6 (1.7) cm more caudad than US, with mean bias –1.5 cm and precision of 2.7 cm by Bland–Altman analysis. US and auscultation agreed poorly, however, on whether right- or left-sided basal lung ventilation was most caudad (Cohen’s kappa 0.07, i.e. slight agreement). The height difference between the most caudad extent of left and right basal lung ventilation by both methods in individual patients was small (US mean (SD) 1.2 (1.2) cm; auscultation mean (SD) 1.6 (1.3) cm) and clinically and statistically insignificant (paired t-test P = 0.33), given the measured intercostal space distance between subjects of mean (SD) 2.1 (0.7) cm. Within the limitations of our small sample size and exploratory study design, our data suggest that there is little difference between auscultation and US estimation of the caudad extent of basal lung ventilation during maximal inspiration. Established chest X-ray data estimate average ICS height at 2 cm; this is closely approximated by our US data of ICS distance of 2.1 cm. However, the height difference between sides as measured by both US and auscultation in our study (mean 1.2 and 1.6 cm difference, respectively) does not appear consistent with the normal range of height difference of diaphragmatic domes observed by established chest X-ray data (within one ICS and ribs, approximately 2 cm). 2 We recommend that further studies be undertaken to assess the accuracy of both auscultation and US in identifying differences in basal lung excursion. Our preliminary experience suggests that such studies are feasible with minimal additional resources. However, future studies should ideally use chest X-ray as the reference standard.
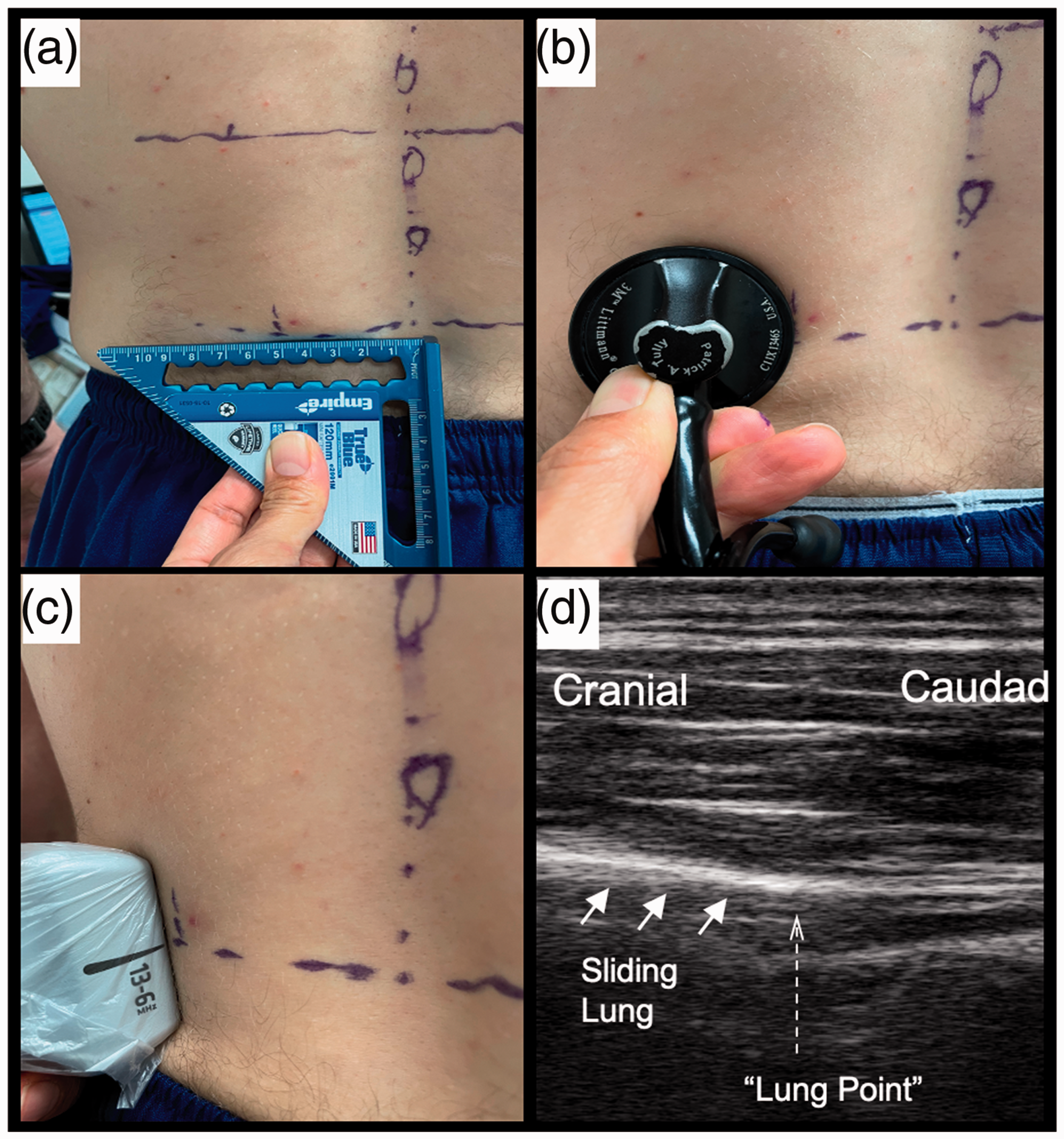
(a) All measurements of lung excursion were taken 5 cm from the midline as measured by a set square. (b) The most caudad point at which lung auscultation remains audible 5 cm from the midline is marked. (c) The most caudad point of visible diaphragmatic excursion 5 cm from the midline is identified using a linear ultrasound probe. (d) Ultrasound demonstration of termination the ‘sliding lung’ sign, representing the most caudad point at which the apposition of parietal and visceral pleura is lost.
Footnotes
Author contributions
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.