
Abstract
Tracheostomy tubes are chosen primarily based on their internal diameter; however, the length of the tube may also be important. We performed a prospective clinical audit of 30 critically ill patients following tracheostomy to identify the type of tracheostomy tube inserted, the incidence of malpositioning and the factors associated with the need to change the tracheostomy tube subsequently. Anthropometric neck measurements, distance between the skin and tracheal rings and the position of the tracheostomy cuff relative to the tracheal stoma were recorded and analysed. Malpositioning of the tracheostomy tube was noted in 20%, with a high riding cuff being the most common cause of malpositioning, resulting in an audible leak and a need to change the tracheostomy tube subsequently. A high riding cuff was more common when a small tracheostomy tube (e.g. Portex (Smiths Medical Australasia, Macquarie Park, NSW) ≤8.0 mm internal diameter with length <7.5 cm) was used, with risk further increased when the patient’s skin to trachea depth was greater than 0.8 cm. Identifying a high riding cuff relative to the tracheal stoma confirmed by a translaryngeal bronchoscopy strongly predicted the risk of air leak and the need to change the tracheostomy tube subsequently. Our study suggests that when a small (and short) tracheostomy tube is planned for use, intraoperative translaryngeal bronchoscopy is warranted to exclude malpositioning of the tracheostomy tube with a high riding cuff.
Introduction
Percutaneous tracheostomy is a common procedure performed in intensive care units (ICUs) to facilitate sputum clearance, oral hygiene care and long-term mechanical ventilation. Clinicians often choose the size of a tracheostomy tube based on its internal diameter, which can affect the ease of its insertion, airflow resistance and the size of suction catheter that can be used subsequently. In addition, for a given internal diameter, different types of commercially available tubes have slightly different outer diameters and lengths. These two latter tube characteristics are often not considered as pivotal by many clinicians when they choose a tube for their adult patients.
Tracheostomy tubes do not pass through the vocal cords, the narrowest part of the upper airway, and hence the size of the tracheostomy tube should be chosen such that the tube occupies between two-thirds and three-quarters of the tracheal diameter to avoid excessive cuff inflation or air leak. 1 The length of a tracheostomy tube is obviously important in determining the position of the tip of the tube relative to the carina. An excessively long tube can increase airway resistance, 2 impinge on the carina causing airway irritation, or end up endobronchially. Conversely, a tracheostomy tube that is too short may cause the tip to impinge on the posterior wall of the trachea with the cuff partially herniating through the tracheal stoma, increasing the risk of air leak, accidental decannulation and aspiration. Previous studies have shown that malpositioning of tracheostomy tubes occurred in about 10% of patients, and that this complication prolonged the duration of mechanical ventilation.3–5
Various tracheostomy tubes with fixed length have been shown to be 1 cm too short for the average critical care patient. 6 If this is true, malpositioning of a tracheostomy tube with the cuff not completely located within the trachea can be quite common. We hypothesised that inserting a tracheostomy tube with an inadequate length relative to the patient’s pretracheal tissue depth can result in malpositioning of the tube with the potential to cause an inadequate air seal. In this prospective clinical audit, we aimed to identify the incidence of malpositioning of tracheostomy tubes, and whether this problem was related to the size (and type) of tracheostomy tubes and patient characteristics.
Materials and methods
Setting of the study
After obtaining approval from both Royal Perth and Sir Charles Gairdner Hospital Clinical Safety and Quality Units, we recruited 30 critically ill adult patients who required a surgical or percutaneous tracheostomy between January 2020 and June 2020, in either of the two tertiary multidisciplinary adult ICUs. The approvals included waiver of consent for obtaining de-identified data and an intention to publish the results. Patients younger than 15 years of age or those who were not admitted to the ICU after tracheostomy were excluded in this prospective cohort study. Standard surgical and anaesthetic procedures were followed in all study patients.
Data collection
Airway and anthropometric details including height, weight, sternomental/thyromental/cricosternal distance, neck circumference just below the cricoid cartilage and distance between skin and anterior tracheal wall at the level of the first tracheal ring, were measured by the same investigator and standardised with the patient’s neck in a neutral position because some patients required cervical spine immobilisation (Figure 1). All patients underwent bronchoscopy after insertion of the tracheostomy tube, both translaryngeal and through the tracheostomy tube.
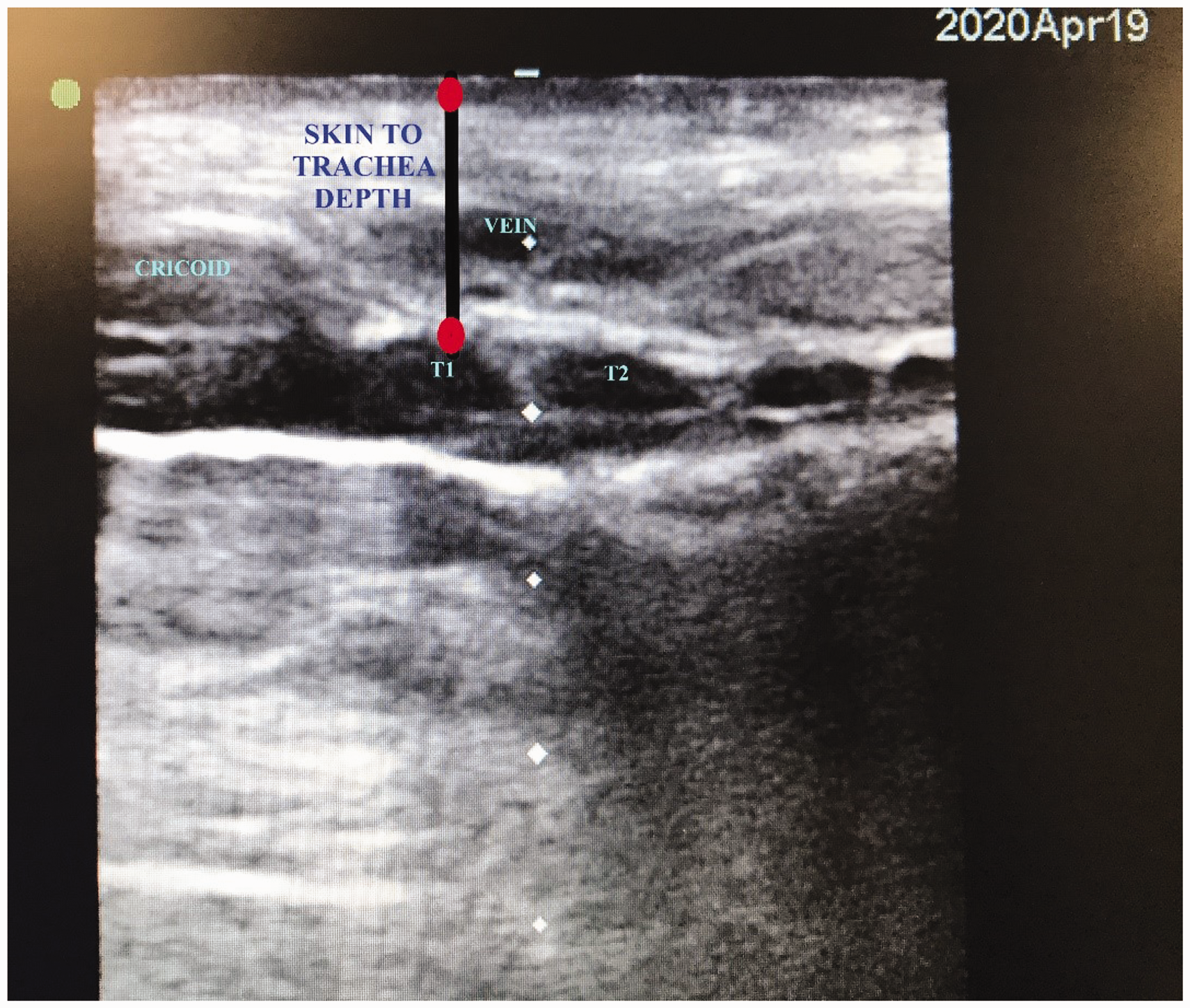
Ultrasound scan of the neck showing the distance between the skin and first tracheal ring (T1). T2, second tracheal ring.
The position of the tracheostomy cuff relative to its entry point at the trachea was assessed by bronchoscopy through the vocal cords (translaryngeal bronchoscopy). When the proximal end of the tracheostomy cuff was not located within the trachea, it was classified as having a high riding cuff (Figure 2(a)). When a short segment of the tracheostomy tube proximal to the cuff could be seen through the translaryngeal bronchoscope, it was classified as proximal end seen (Figure 2(b)). When the tracheostomy cuff was far below the tracheal entry point and could not be seen through the bronchoscope, it was classified as cuff deep-seated. A tracheostomy with a high riding cuff was considered to be malpositioned in this study.
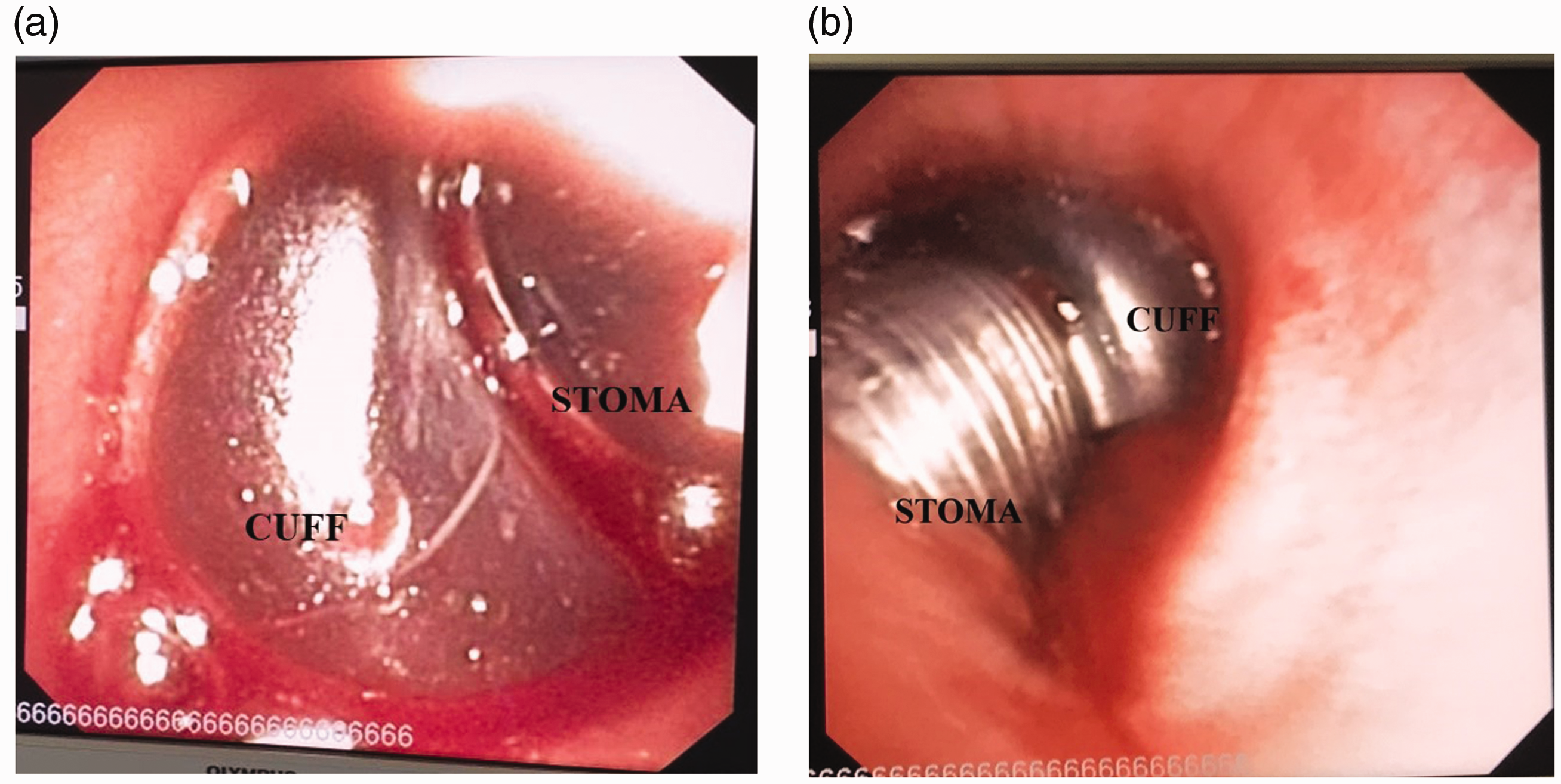
Translaryngeal upper airway bronchoscopy view. (a) A high riding cuff; (b) proximal end of the cuff fully seen inside the tracheal lumen.
The distance between the tip of the tracheostomy tube and carina measured by bronchoscopy, and the orientation of the tube with respect to the tracheal lumen, were recorded. A tube directed anteriorly or posteriorly such that more than 50% of the tube lumen was obstructed or obscured by the tracheal wall was also considered as malpositioned. The distance between the carina and the tip of the tracheostomy tube was measured again on a chest X-ray after the procedure.
Events related to tracheostomy such as difficulty in ventilation, audible air leak, need for higher than normal cuff pressure (>30 mmHg) to achieve adequate seal and loss of tidal volume on the ventilator were recorded within the first 48 hours after insertion of the tracheostomy. Any new issues related to the tracheostomy requiring medical attention beyond the first 48 hours after the procedure were also recorded.
Statistical analyses
Categorical and continuous data were summarised in frequency and median with interquartile range (IQR), and compared by chi-square and Mann–Whitney U tests, respectively. All statistical tests were two-sided, and an alpha value of less than 5% was considered statistically significant.
Results
Eighty percent of our patients were men; the median age and body mass index of the cohort were 49 years and 26.4 kg/m2, respectively. The patient characteristics are described in Table 1. Portex™ (Smiths Medical Australasia, Macquarie Park, NSW) tracheostomy tubes (with or without a subglottic suction port) and UniPerc™ (Smiths Medical Australasia, Macquarie Park, NSW) (adjustable flange tubes) were first inserted in 22 patients (73%) and eight patients (27%), respectively. A 9.0 mm internal diameter Portex tube was the commonest and about half of all tubes were 8.5 mm or greater internal diameter Portex tubes. According to the surgical operators, the choice of tube used was based on their subjective assessment of the patient’s body habitus (thin built, standard adult or obese) in 70% of the patients.
Characteristics of the study patients (N=30).
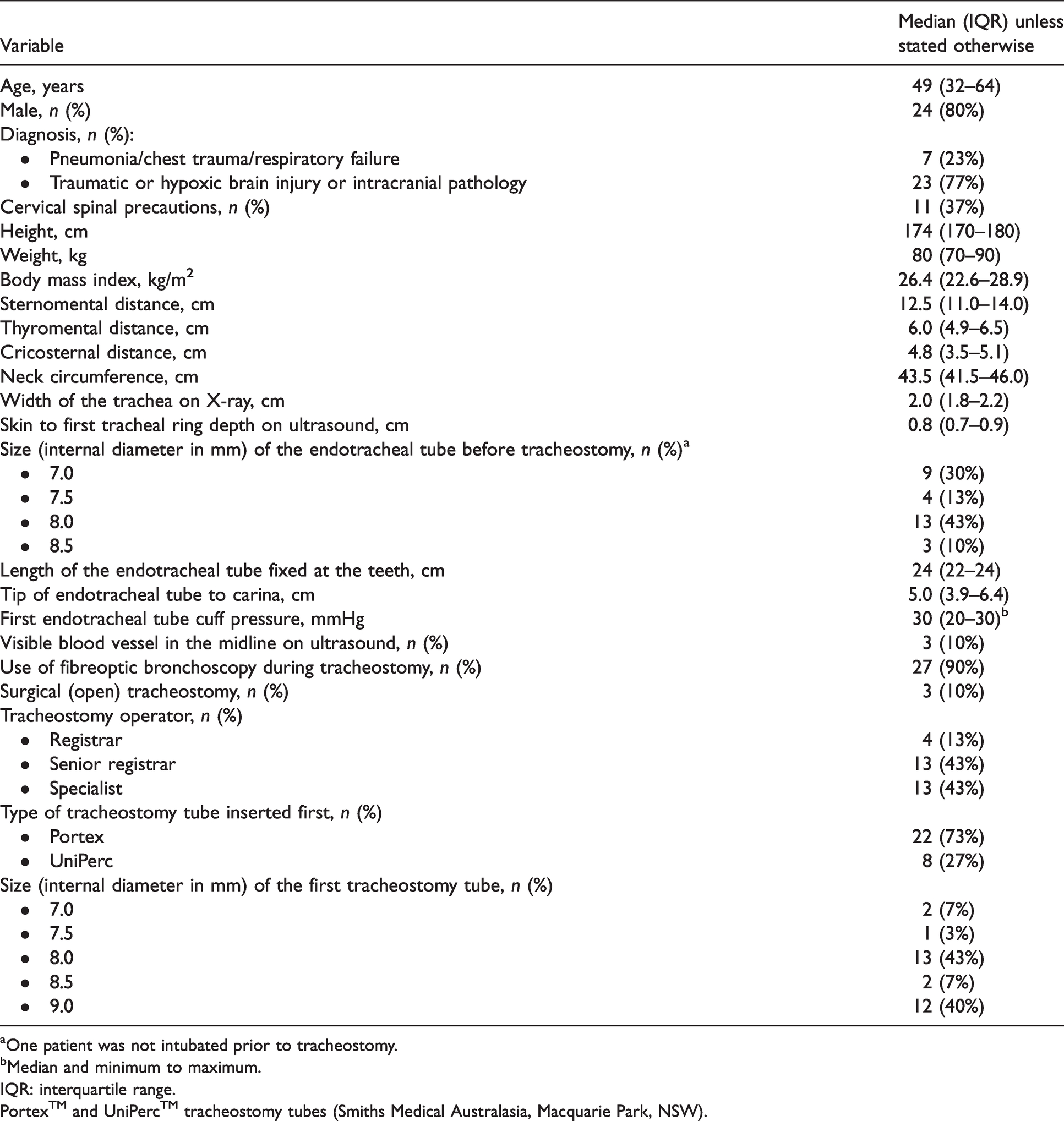
aOne patient was not intubated prior to tracheostomy.
bMedian and minimum to maximum.
IQR: interquartile range.
Portex™ and UniPerc™ tracheostomy tubes (Smiths Medical Australasia, Macquarie Park, NSW).
Incidence of malpositioning and audible air leak
Malpositioning of tracheostomy tube was observed in six patients (20%). A high riding cuff was observed in three patients (10% of all patients) all of whom had a Portex tube (one 7.0 and two 8.0 mm internal diameter tubes) (Table 2). Significant audible leak during positive pressure ventilation was subsequently observed in these three patients. After excluding patients who had an adjustable flange UniPerc tube initially, 13.6% of those with a Portex tube had a high riding cuff. A tracheostomy tube lumen facing the tracheal wall anteriorly was observed in two patients (7%, one with a Portex and one with a UniPerc tube), and in another patient (3%) the tip of the tube was considered too close to the carina (<1.5 cm). Air leak was not observed in these latter three patients.
Malpositioning and audible air leak outcomes (N=30).
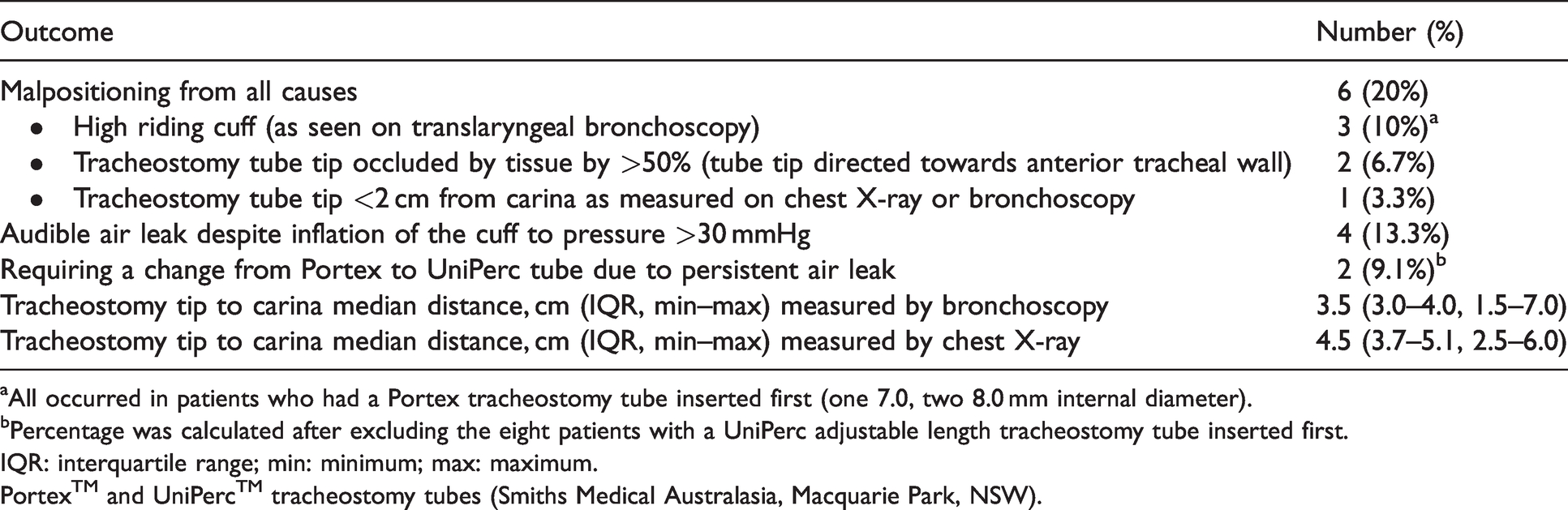
aAll occurred in patients who had a Portex tracheostomy tube inserted first (one 7.0, two 8.0 mm internal diameter).
bPercentage was calculated after excluding the eight patients with a UniPerc adjustable length tracheostomy tube inserted first.
IQR: interquartile range; min: minimum; max: maximum.
Portex™ and UniPerc™ tracheostomy tubes (Smiths Medical Australasia, Macquarie Park, NSW).
Audible air leak (cuff pressure up to >30 mmHg) was observed in four patients (13.3%), and all of them had a Portex tube (two 7.0 and two 8.0 mm internal diameter tubes). After excluding patients who had a UniPerc tube, the incidence of air leak was 18.2%. Three out of these four patients also had a high riding cuff, of whom two had associated difficulty in ventilation. Only the three patients who had a high riding cuff along with persistent air leak required a change of the tracheostomy tube. Two patients had their Portex tube changed to a UniPerc tube to facilitate better seal and ventilation, while the third patient was deemed suitable for decannulation, but due to concerns re secretion clearance, and following a failed attempt at inserting a larger size tube, a 7.0 was changed for a 6.0 mm internal diameter Portex tube. After excluding patients who originally received a UniPerc tube, the incidence of patients requiring a change from a Portex tube to a UniPerc tube due to persistent air leak was 9.1%.
Predictors of air leak, high riding cuff and the need to change the tracheostomy
A high riding cuff was significantly more common among those with air leak than those without air leak (P = 0.001). The average depth from the skin to the first tracheal ring on ultrasound was 0.8 cm, and the use of a tracheostomy tube of 8.0 mm or less internal diameter in patients with skin to first tracheal ring depth greater than 0.8 cm was strongly associated, compared to patients without this combination, with subsequent audible air leak (3/6 (50%) versus 1/24 (4%), P = 0.003), a high riding cuff (3/6 (50%) versus 0/24 (0%), P = 0.001) and a need to change the tube (3/6 (50%) versus 0/24 (0%), P = 0.003). The use of an 8.0 or smaller tube alone (without considering skin to tracheal depth) was also associated with a higher risk of air leak compared to larger than 8.0 tubes (≤8.0: 4/16 (25%) versus ≥8.5: 0/14 (0%), P = 0.044).
Body mass index (P = 0.746), sternomental distance (P = 0.198), cricosternal distance (P = 0.930) and neck circumference (P = 0.198) were not significantly associated with air leak. Similarly, the distance between the tip of the tracheostomy tube and the carina, measured either on chest X-ray (P = 0.617) or by bronchoscopy (P = 0.157), were not significantly associated with the air leak.
Comparing lengths of UniPerc and Portex tubes
The average depth of a UniPerc tube from the skin entry point to the tip of the tube was 8.95 cm (minimum 8 cm to maximum 10 cm), which was longer than the longest Portex tube (9.0 mm internal diameter tube, 8.1 cm). The standard lengths of tubes are summarised in Table 3.
Differences in length and outer diameter between the Portex and UniPerc tracheostomy tubes.
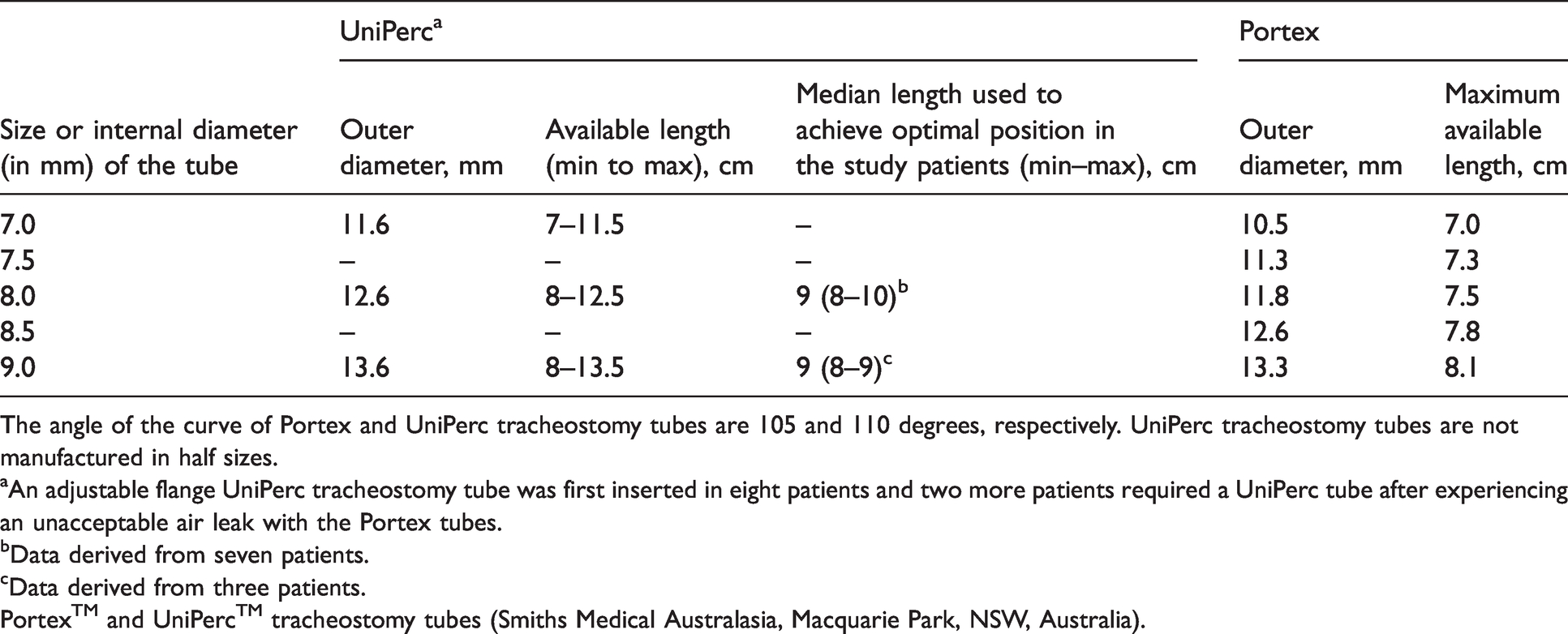
The angle of the curve of Portex and UniPerc tracheostomy tubes are 105 and 110 degrees, respectively. UniPerc tracheostomy tubes are not manufactured in half sizes.
aAn adjustable flange UniPerc tracheostomy tube was first inserted in eight patients and two more patients required a UniPerc tube after experiencing an unacceptable air leak with the Portex tubes.
bData derived from seven patients.
cData derived from three patients.
Portex™ and UniPerc™ tracheostomy tubes (Smiths Medical Australasia, Macquarie Park, NSW, Australia).
Discussion
In this prospective cohort study, we observed a 20% incidence of tracheostomy malpositioning with half of these due to inadequate depth of insertion with a short Portex tube, resulting in audible air leak and inadequate ventilation necessitating a change in tube. These findings have some clinical implications and require further consideration.
First, we confirmed that Portex tubes, especially those 8.0 mm internal diameter or smaller (with a length <7.5 cm), are inadequate for many adult critically ill patients in Western Australia. This is particularly problematic if the patient also has a thick layer of soft tissue in front of the tracheal ring (>0.8 cm skin to tracheal ring distance). Although a smaller tube may induce less injury and a smaller scar to the skin and trachea, there is a trade-off with smaller internal diameter tubes also being shorter (Table 3), increasing the risk of having a high riding cuff. A high riding cuff is not completely harmless as it can cause persistent air leak, inadequate ventilation, aspiration, and a failure to position the subglottic port of the tracheostomy tube completely within the tracheal lumen. Our results support the results of the study by Mallick et al., 6 which concluded that commonly used tracheostomy tubes are too short, and a length of at least 7.8 cm between the skin and the tip of the tube is needed to avoid a high riding cuff in adult critically ill patients.
Second, inspecting the tracheostomy cuff position (relative to the tracheal entry point) through the native upper airway after its placement has been described previously in the LUNAR study, 7 in which a grading system of the translaryngeal views was developed to describe the positioning of the tube. Our findings are supportive of this previous study and this technique should be seriously considered if a small and short tracheostomy is inserted.
Third, an ultrasound examination of the soft tissue depth anterior to the first tracheal ring may be useful in determining whether a UniPerc tube should be used instead of a Portex tube, especially when the use of an 8.0 mm internal diameter or smaller tube is planned. The Australian and New Zealand Intensive Care Society consensus statement on percutaneous tracheostomy advises the use of ultrasound to determine the size of the tube based on skin to tracheal distance. 8 Our study provides objective evidence to support this statement by confirming that the distance between the trachea and the skin measured by ultrasound predicted tube malpositioning and the need for a longer length tube. Obese patients have been shown to have a greater skin to tracheal depth compared to non-obese patients, 9 and using a longer tube in patients with a tracheal depth of more than 1 cm could reduce the incidence of accidental decannulation and air leak. 10 In our study, the three patients who needed a change of tracheostomy tube within the first week of insertion due to a high riding cuff with persistent air leak were overweight. Hence, measuring the skin to first tracheal ring depth for patients who are undergoing tracheostomy and who are overweight may be advisable; and a UniPerc tube (or a Portex tube ≥8.5 mm internal diameter) would be preferable if the skin depth is greater than 0.8 cm. It is tempting to suggest that we should use a UniPerc tube for all adult critically ill patients as this would solve the problem of inadequate length. Nonetheless, many doctors and nurses, particularly those working in hospital wards as opposed to ICUs, may not be familiar with the UniPerc tubes or know how to manage them safely without accidental dislodgement. In addition, the UniPerc tubes have wire reinforcement which can create image artefacts on, for example, a magnetic resonance imaging cervical spine scan.
Finally, we need to acknowledge the limitations of this study. The sample size was small and our results may not be generalisable to shorter/smaller patients. Using translaryngeal bronchoscopy to determine cuff position by a single observer is not as accurate as objective measurement of the distance between the stoma and cuff. Nonetheless, inter-rater agreement in rating the position of a tracheostomy tube cuff translaryngeally was reasonable according to previous studies. 7 The size of tracheostomy tubes used in one centre was significantly larger (and longer) than those used in the other centre. This would have reduced the incidence of a high riding cuff and, hence, the statistical power of the study in determining the predictors of air leak.
Conclusion
Malpositioning of a tracheostomy tube with a high riding cuff due to inadequate length was common in adult critically ill patients, especially when a small (and short) tube was used in patients with a thick layer of soft tissue anterior to their tracheal rings (>0.8 cm). A larger (and longer) or adjustable flange tracheostomy tube will be more appropriate for such adult patients. If a smaller and shorter tube is still preferred, intraoperative upper airway translaryngeal bronchoscopy should be considered after placement to exclude a high riding cuff.
Footnotes
Author contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.