
Abstract

The review of Erstad and Barletta 1 on the question of the choice of weight scalar for the dosing of neuromuscular blocking agents (NMBAs) recommends different scales for non-depolarising and depolarising drugs. The use of lean body mass (LBM) in pharmacokinetics is interesting, as despite its theoretical advantages, it is very rarely used in clinical practice. Reasons include the number of different formulae available to calculate LBM and the complexity of using these. Several medical calculator apps do perform this function but the formula chosen is not always made apparent.
The underlying concept in the calculation of LBM is the difference between actual body weight and body fat content. LBM is considered roughly equivalent to fat free mass, which can be evaluated in a number of different ways. To investigate the differences between some of the more commonly quoted formulae, I modelled the calculation of LBM using a hypothetical set of heights and weights that covered a range of body mass index (BMI) values that are not uncommonly encountered in clinical practice. I chose several different formulae that are available in a number of different settings, including the one quoted by Erstad and Barletta. 1 These were developed from a range of backgrounds and for a range of purposes, date from 1966 to 2005, and can be found in a summary form on the website https://www.calculator.net/lean-body-mass-calculator as well as the paper by Erstad and Barletta.2–5 One limitation of all of these formulae is that the populations from which they were developed included few patients with BMIs over 30 kg/m2. 6 Table 1 shows the results of this modelling exercise.
Modelling of lean body mass of hypothetical patients.

BMI: body mass index; LBM: lean body mass.
Figure 1 shows a graph of the LBM mapped against actual body weight for men and women, and Figure 2 plots LBM against BMI. It can be seen that the values for LBM are fairly similar at lower weights, and start to diverge at a weight of about 150 kg in men and 130 kg in women. Similarly, the LBM returned by the various formulae diverge at a BMI of over about 50 kg/m2 in men and 45 kg/m2 in women. The obvious outlier is the James formula. This incorporates height in the denominator of the calculation, which explains its parabolic curve as weights become more extreme. A negative value is possible with this formula. Even though the other three formulae track more closely together with increasing weight, there is still a discrepancy between them; for example, for hypothetical patient 5 with a BMI in the 60s, there is a difference of 17 kg in men and 12 kg in women between the lowest and highest calculated LBM, with even larger differences for the larger patient 6.
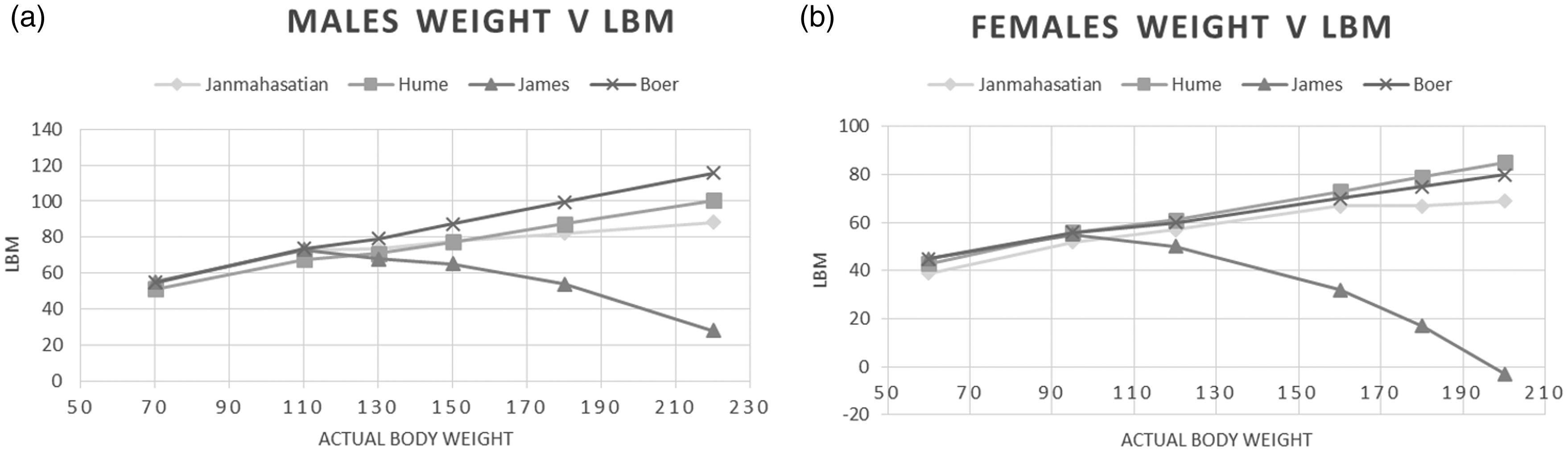
Lean body mass (LBM) versus actual body weight. Weight and LBM in kilograms. (a) Men; (b) women. Modelled from Janmahasatian2, Hume3, Boer4 and James5.

Lean body mass (LBM) versus body mass index (BMI). LBM in kilograms, BMI in kg/m2. (a) Men; (b) women. Modelled from Janmahasatian2, Hume3, Boer4 and James5.
Fortunately in anaesthesia, with the exception of NMBAs for induction, we give most drugs as a dosage calculated by titration to effect. Calculating an exact dose based on a selected body weight scalar is not always necessary. In contrast to one point made by Erstad and Barletta, LBM calculations become more variable with increasing BMIs over about 45 kg/m2, and results should be interpreted with caution in these patients. For drugs that require a single pre-calculated dose, the use of an ideal body weight, with or without an adjustment of some sort, is likely to be more reliable and helpful.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.