
Abstract
The Ambu® AuraGain™ (Ambu A/S, Ballerup, Denmark) is a newer phthalate-free, single-use supraglottic device with the advantage of a facility for tracheal intubation if necessary intraoperatively. We compared the oropharyngeal leak pressures and other performance variables between the AMBU AuraGain and the LMA® Supreme™ (Teleflex Medical, Athlone, Co. Westmeath, Ireland) in patients undergoing laparoscopic cholecystectomy and preperitoneoscopic inguinal herniorrhaphy with carbon dioxide insufflation under controlled ventilation. We recruited 120 American Society of Anesthesiologists physical status class I–3 patients between the ages of 21 and 80 years undergoing laparoscopic cholecystectomy or preperitoneoscopic inguinal herniorrhaphy into this single-centre randomised controlled trial. The primary outcome measure was the oropharyngeal leak pressures. Secondary outcomes included insertion parameters, ventilatory characteristics and postoperative sequelae. The AuraGain had slightly but significantly higher oropharyngeal leak pressures than the LMA Supreme (mean (standard deviation) 26.1 (6.9) versus 21.4
Introduction
The improved safety profiles and oropharyngeal leak pressures (OLPs) of second-generation supraglottic devices (SGDs) allow anaesthetists to push the envelope and expand the utility of SGDs, including their use in laparoscopic surgery.1–4 SGDs are associated with lower haemodynamic and metabolic stress responses compared to tracheal intubation.5,6 Increased intra-abdominal pressure from carbon dioxide (CO2) pneumoperitoneum does not affect ventilation through SGDs,7–10 and the gastric channel allows timely gastric decompression.
The Ambu® AuraGain™ (Ambu A/S, Ballerup, Denmark) (AG) is a phthalate-free, single-use SGD. Its design is similar to the LMA® Supreme™ (Teleflex Medical, Athlone, Co. Westmeath, Ireland) (LS), consisting of an anatomically curved airway tube and a built-in gastric access port. Different from the LS, the AG has a further advantage of direct intubating capability which facilitates tracheal intubation intraoperatively when necessary.
We aimed to evaluate the performance of the AG against the LS in laparoscopic surgery with controlled ventilation. The primary outcome was oropharyngeal leak pressures, while secondary outcomes included insertion parameters, ventilatory characteristics and postoperative sequelae.
Methods
Ethics approval for this study was provided by the National Healthcare Group Domain-Specific Institutional Review Board (NHG DSRB). Approval number 2015/00989. Prospective trial registration was performed with the Australian New Zealand Clinical Trials Registry (www.anzctr.org.au, trial number: ACTRN12616000762459). We recruited 120 patients into this single-centre, single-blinded randomised controlled study performed in our tertiary institution. Written informed consent was obtained from patients who met the inclusion criteria of the American Society of Anesthesiologists (ASA) physical status class 1 to 3, aged 21–80 years, and required general anaesthesia for laparoscopic cholecystectomy and preperitoneoscopic inguinal herniorrhaphy. Exclusion criteria were age <21 or >80 years; body mass index (BMI) >35 kg/m2; body weight <30 kg; predicted difficult airway (history of difficult airway, inter-incisor distance <40 mm, cervical spine pathology, modified Mallampati score 4, thyromental distance <60 mm); contraindication to SGD use (high risk of regurgitation or aspiration, such as gastro-oesophageal reflux disease or hiatus hernia); respiratory tract pathology; refusal to participate; or inability to give informed consent.
Following recruitment, each subject was randomly allocated into one of two groups, AuraGain (AG) or LMA Supreme (LS), using a software-generated block randomisation procedure (www.randomization.com). Allocation concealment was achieved with consecutively numbered sealed opaque envelopes.
Pre-anaesthetic airway assessment was performed by the study investigators. Patient demographics such as age, gender, ASA physical status, BMI, inter-incisor distance, thyromental distance, Mallampati score, type of surgery, and length of surgery were collected. Prior to induction of general anaesthesia, the envelope was opened by the enrolling investigator to reveal the device to be inserted. Patients were blinded to their group allocation. Manufacturers’ recommendations were followed in regard to the size, preparation, and lubrication of airway devices. Study subjects were positioned supine with neck in the neutral position and standard monitoring applied. Pre-oxygenation was performed with high flow oxygen for three minutes. Induction of general anaesthesia was carried out using intravenous fentanyl 1–2 µg/kg and propofol 1–3 mg/kg. Atracurium 0.5 mg/kg or rocuronium 0.6 mg/kg was then administered for neuromuscular blockade after confirmation of successful bag-mask ventilation. The subject was manually ventilated (100% oxygen, 2%–4% sevoflurane or 6%–8% desflurane), followed by SGD insertion after three minutes, when the jaw was subjectively relaxed.
Insertion of the device was performed according to manufacturers’ recommendations. Successful insertion was defined as the successful establishment of ventilation with the appearance of the first square end-tidal CO2 waveform. The device cuff was inflated with air to a cuff pressure of 60 cmH2O, measured with a cuff pressure gauge (VBM Medizintechnik GmbH, Sulz am Neckar, Germany). If an effective airway could not be obtained, the SGD was removed for a second attempt, using the same size or a different size when appropriate and/or with additional manoeuvres, as needed. A maximum of three attempts were allowed. Each attempt was defined as the reinsertion of the SGD into the mouth. Insertion failure was defined as three unsuccessful attempts, or if the time to insertion exceeded 120 s (inclusive of the time taken for device removal and bag-mask ventilation in between attempts). In the event of insertion failure, the patient’s airway was secured and managed at the discretion of the attending anaesthetist. The study investigator rated the ease of device insertion on a three-point scale (easy, fair, difficult).
Once the SGD was secured, its position was checked by placing a gel plug 11 on the proximal gastric drain outlet; the suprasternal notch was gently tapped to elicit a gel pulsation to confirm the SGD tip’s location behind the cricoid cartilage. The OLP was measured by closing the adjustable pressure-limiting valve of the circle system to 70 cmH2O, at a fixed gas flow of 3 l/min in manual ventilation mode. The OLP was the pressure in the circuit when an audible noise was heard at the mouth or equilibrium pressure was achieved. For safety concerns, the maximal allowable OLP was 40 cmH2O and auscultation over the epigastrium was done at the same time to rule out air leak into the stomach during measurement. A 14 Fr gastric tube was passed through the drainage port; placement was confirmed by aspiration of gastric contents and auscultation for injected air over the epigastrium. The gastric tube was then placed on passive drainage.
General anaesthesia was maintained with oxygen (O2) and air mixture, sevoflurane/desflurane and atracurium or rocuronium boluses. Initial ventilator tidal volume was set at 8 ml/kg and an inspiration:expiration (I:E) ratio of 1:2. Volume-controlled positive pressure ventilation was used with tidal volumes 7–10 ml/kg, respiratory rates 10–18 breaths per minute to achieve end-tidal CO2 35–40 mmHg and peripheral oxygen saturation (SpO2) more than 95%. Pneumoperitoneum was created in intraperitoneal surgeries, while CO2 insufflation into the extraperitoneal space was done for laparoscopic inguinal herniorrhaphy. Patient positioning was reverse Trendelenburg for laparoscopic cholecystectomy and Trendelenburg for preperitoneoscopic inguinal herniorrhaphy. Following CO2 insufflation, the intra-abdominal pressure was noted for intraperitoneal surgery (cholecystectomy), whereas the insufflation pressure achieved was recorded for extraperitoneal surgery (herniorrhaphy). Leak volume (difference between inspiratory and expiratory tidal volumes) and peak inspiratory pressure (PIP) were recorded before and after CO2 insufflation as well as 30 minutes into the surgery. Cuff pressure was recorded 30 minutes after commencement of surgery. For intraperitoneal surgeries, the surgeons reported visual assessment of the presence of gastric distension at the beginning and end of laparoscopy. At the end of surgery, neuromuscular blockade was reversed with intravenous neostigmine 0.04 mg/kg and either atropine 0.02 mg/kg or with glycopyrrolate 0.2–0.4 mg, or with sugammadex 2–4 mg/kg. The SGD was removed in the operating theatre upon return of spontaneous breathing and eye opening, and was inspected for the presence of blood. Thirty minutes after arriving in the post-anaesthesia care unit (PACU), the nurse taking care of the study subject recorded the presence of any sore throat, dysphonia or dysphagia.
Insertion of the SGDs and contemporaneous data recording was performed by all the study investigators, except WHT. All investigators had at least three years of anaesthesia experience, and at least ten LS and ten AG insertions in patients with normal airways before trial commencement. The primary outcome measure of the study was OLP. Secondary outcomes included number of attempts at device insertion, time to device insertion (from insertion of airway device into the mouth until the presence of first end-tidal CO2 waveform on capnography), ease of device insertion, intraoperative device performance, respiratory parameters (PIP, leak volume) and postoperative complications (gastric distension, regurgitation, sore throat, dysphonia and dysphagia).
On planning of this trial’s protocol, there were few published studies involving the AG in the clinical setting. One study demonstrated the mean (standard deviation, SD) OLP of the LS to be 26 (5) cmH2O in the South-East Asian population. 12 As we were going to be subjecting our patients to mechanical ventilation in the Trendelenburg and reverse Trendelenburg positions with CO2 insufflation intra- and extraperitoneally, we deemed that a difference of 10% in mean OLP between the AG and LS could likely be clinically relevant. Using a desired power of 80% and two-sided significance level of 5%, a sample size of 59 patients in each group (total of 118 patients) was calculated to be adequate for each SGD (Stata v 13.1, StataCorp LLC, College Station, TX, USA). We recruited 60 patients per group to account for drop-outs.
Data analysis was performed using IBM SPSS v 22.0 (IBM, New York, NY, USA). Continuous variables were presented as mean (SD) or median (interquartile range, IQR) where appropriate and categorical variables summarised using numbers (proportion). The independent Student’s t-test or Mann–Whitney U test was used to compare means between two groups after assessing normality. The chi-square test or Fisher’s exact test was used for comparison of categorical variables when appropriate. P-values were two-sided, and values less than 0.05 were considered statistically significant.
Results
One-hundred-and-twenty participants were recruited between June 2016 and September 2018. The data collection form of one participant could not be located after the completion of the study. Data from 119 participants were analysed according to the intention-to-treat basis (Figure 1). Table 1 shows the patient characteristics, which were similar between the two groups.
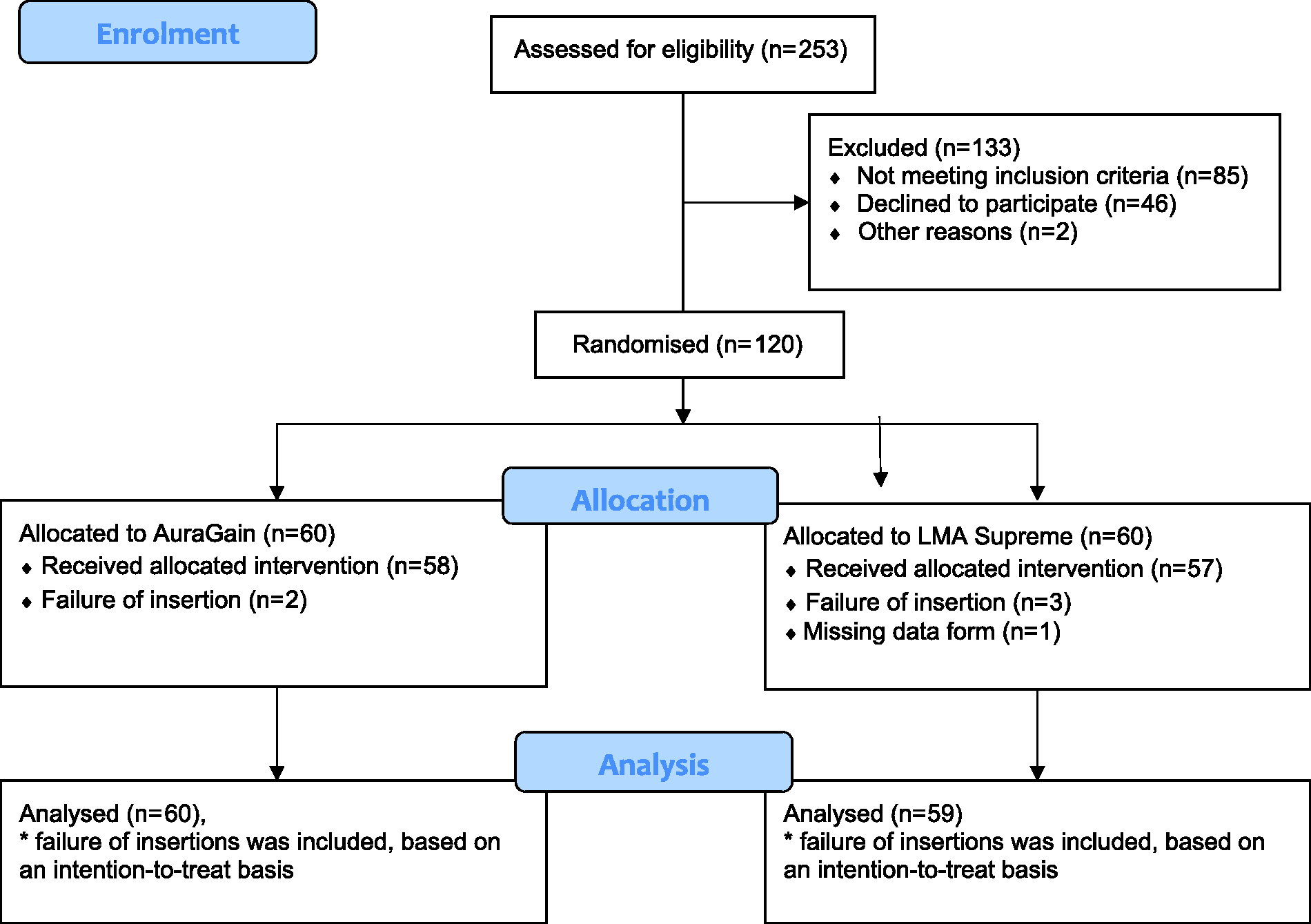
Consolidated standards of reporting trials (CONSORT) flow diagram (www.consort-statement.org) for patient participation. AuraGain™ (Ambu® A/S, Ballerup, Denmark) (AG); LMA® Supreme™ (Teleflex Medical, Athlone, Co. Westmeath, Ireland) (LS).
Patient and surgical variables.
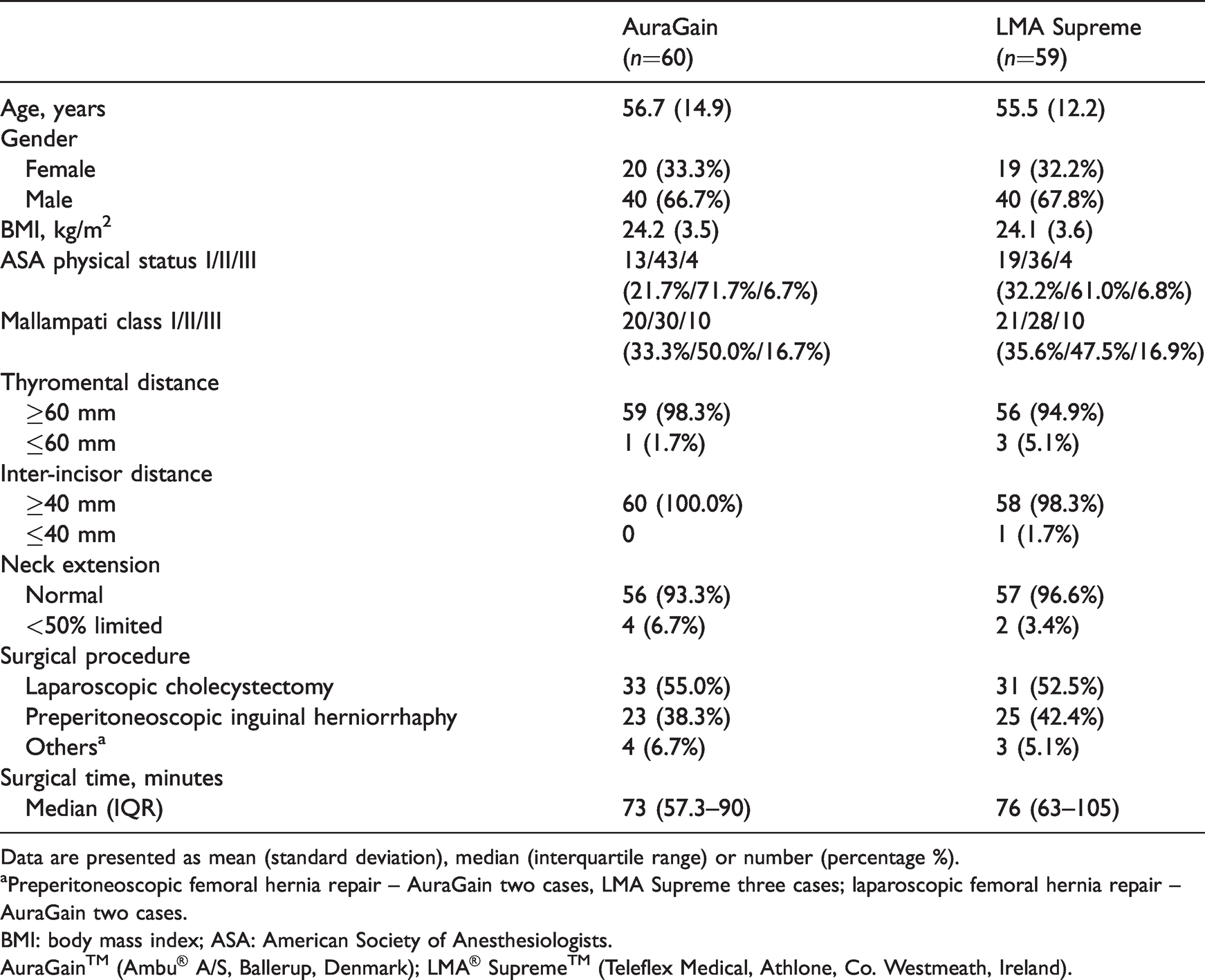
Data are presented as mean (standard deviation), median (interquartile range) or number (percentage %).
aPreperitoneoscopic femoral hernia repair – AuraGain two cases, LMA Supreme three cases; laparoscopic femoral hernia repair – AuraGain two cases.
BMI: body mass index; ASA: American Society of Anesthesiologists.
AuraGain™ (Ambu® A/S, Ballerup, Denmark); LMA® Supreme™ (Teleflex Medical, Athlone, Co. Westmeath, Ireland).
Data concerning device insertion are presented in Table 2. With regard to the primary outcome measure, the AG had a higher mean (SD) OLP of 26.1 (6.9) cmH2O than the LS 21.4 (4.7) cmH2O, P < 0.01. Fifty-seven of 60 (95%) AGs and 54/59 (91.5%) LSs were successfully inserted at the first attempt (P = 0.691). Overall success at AG insertion was 96.7% and 94.9% for LS (P = 0.679). The AG was deemed subjectively more difficult to insert, with only 26/60 (43.3%) of AG insertions graded easy versus 48/59 (81.4%) of LS insertions, P < 0.001. The mean (SD) time to insertion was also longer for the AG, 32.2 (10.5) s, versus the LS, 28.3 (12.0) s, P = 0.001. At OLP, audible gastric insufflation occurred in five of 60 (8.3%) patients in the AG group and six of 59 (10.2%) patients in the LS group (P = 0.729).
Airway device insertion characteristics.
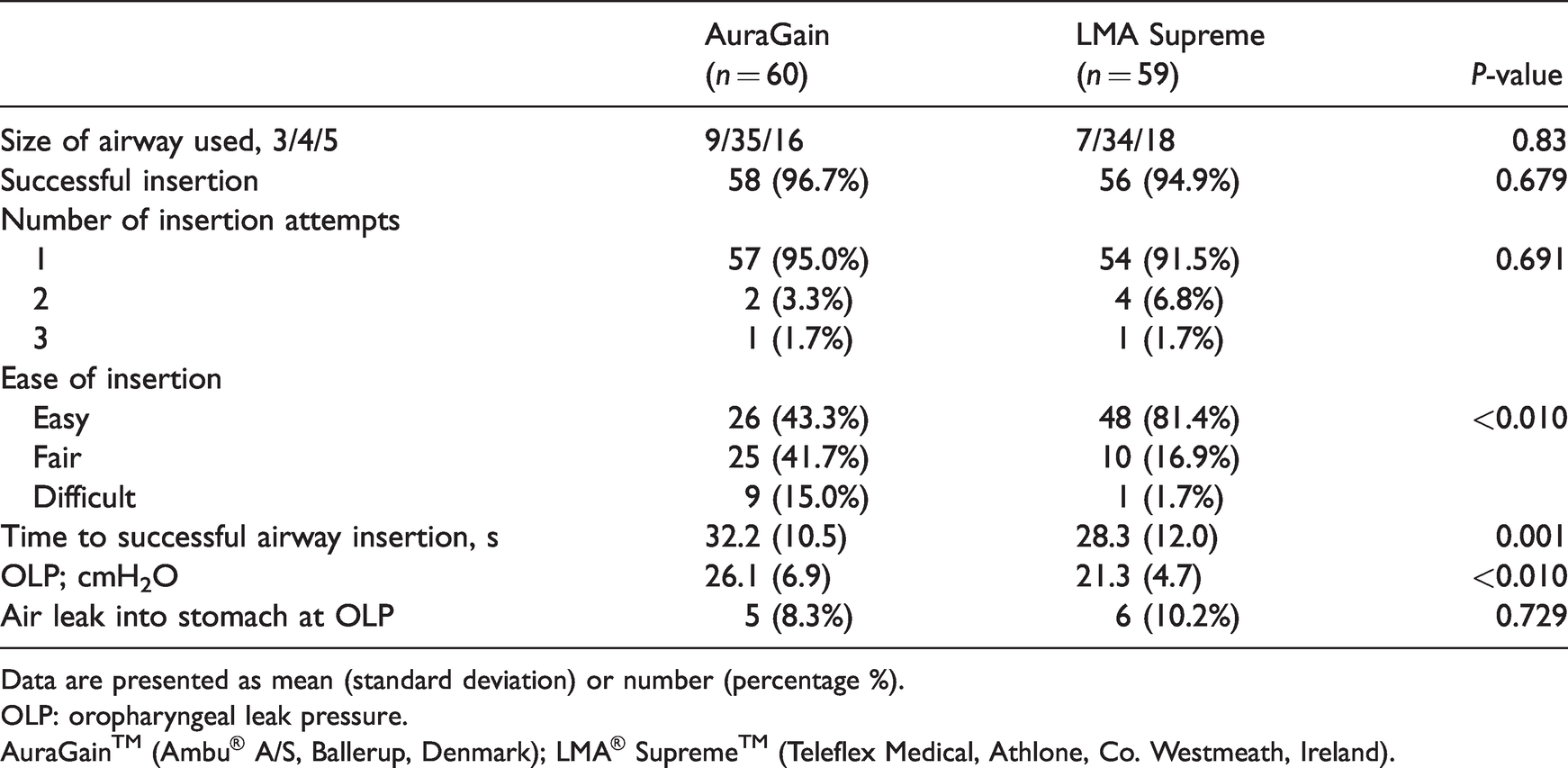
Data are presented as mean (standard deviation) or number (percentage %).
OLP: oropharyngeal leak pressure.
AuraGain™ (Ambu® A/S, Ballerup, Denmark); LMA® Supreme™ (Teleflex Medical, Athlone, Co. Westmeath, Ireland).
Table 3 highlights the intraoperative airway maintenance and ventilatory performance of the SGDs. Intraoperative device failure occurred in one patient in the AG group and three patients in the LS group, where an audible leak was heard and the PIP exceeded OLP following CO2 insufflation. Airway manipulation (e.g. jaw thrust, neck adjustment, pulling and pushing of the SGD, changing SGD size), and/or additional muscle paralysis and/or requesting the surgeons to reduce the CO2 insufflation pressures were performed to improve ventilation. However, the PIP and air leak remained refractory to adjustments and tracheal intubation was performed. Of note, the recorded baseline OLP was less than 20 cmH2O in the patient in the AG group and one patient in the LS group. We did not remove the devices initially, in spite of a low OLP after insertion as we assessed that adequate positive pressure ventilation with minimal leak volume was achieved. Taking into account intraoperative device failure, the perioperative success rates for the AG and LS were 57/60 (95%) and 53/59 (89.8%), respectively, P = 0.322. There was no significant difference in leak volume and cuff pressure intraoperatively between the two groups. In addition, there was no significant difference in PIPs between patients who were placed in reverse Trendelenburg position for cholecystectomy (intraperitoneal surgery) and Trendelenburg position for preperitoneoscopic inguinal herniorrhaphy (extraperitoneal surgery) at the various timepoints shown in the table.
Intraoperative device performance and ventilation of the supraglottic devices that were successfully inserted.
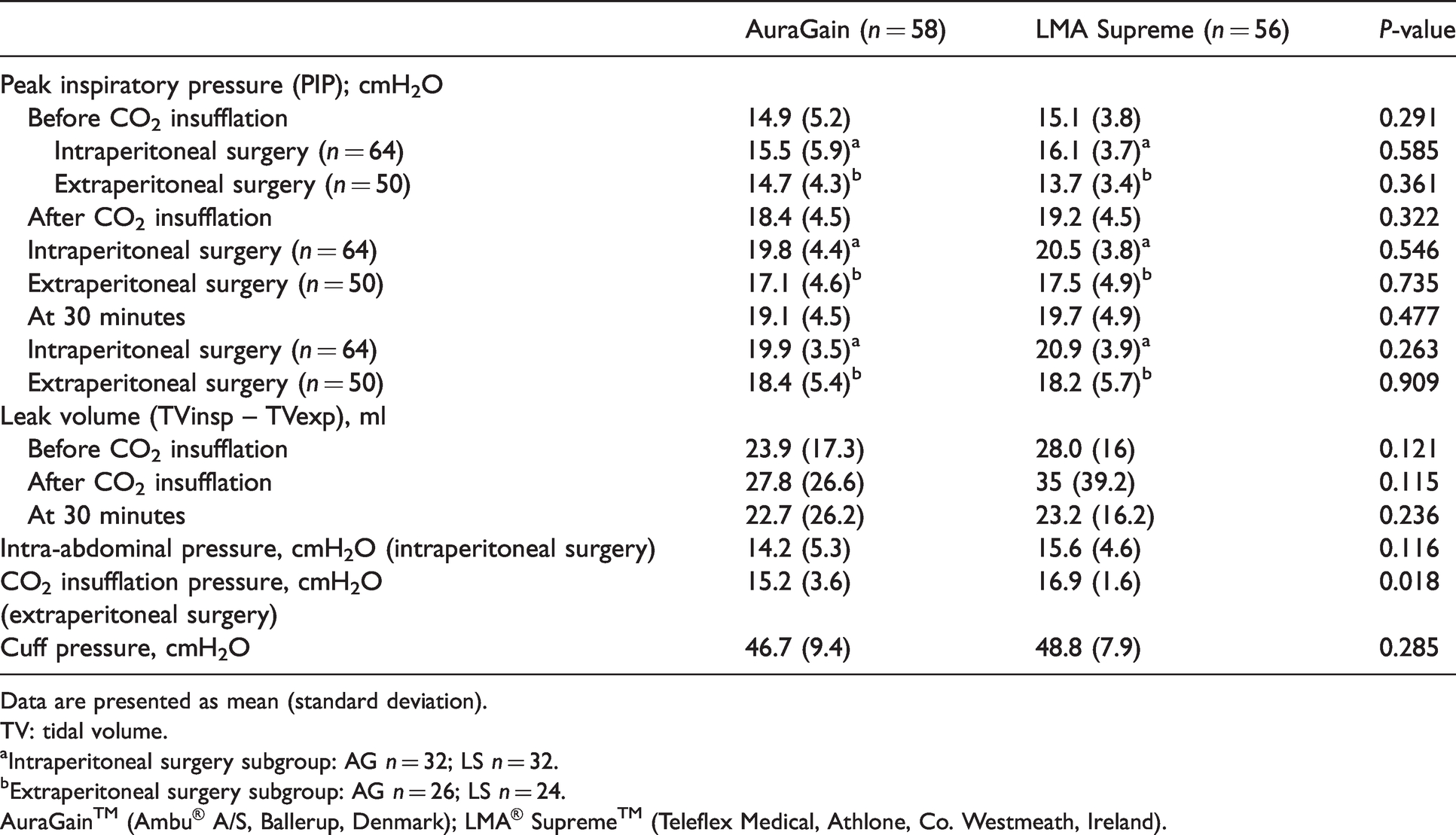
Data are presented as mean (standard deviation).
TV: tidal volume.
aIntraperitoneal surgery subgroup: AG n = 32; LS n = 32.
bExtraperitoneal surgery subgroup: AG n = 26; LS n = 24.
AuraGain™ (Ambu® A/S, Ballerup, Denmark); LMA® Supreme™ (Teleflex Medical, Athlone, Co. Westmeath, Ireland).
Table 4 shows intraoperative and postoperative complications. Although visible gastric distension was observed in seven patients in the AG group and five patients in the LS group within the intraperitoneal surgery subgroup, no cases of regurgitation or aspiration occurred.
Intraoperative and postoperative complications.
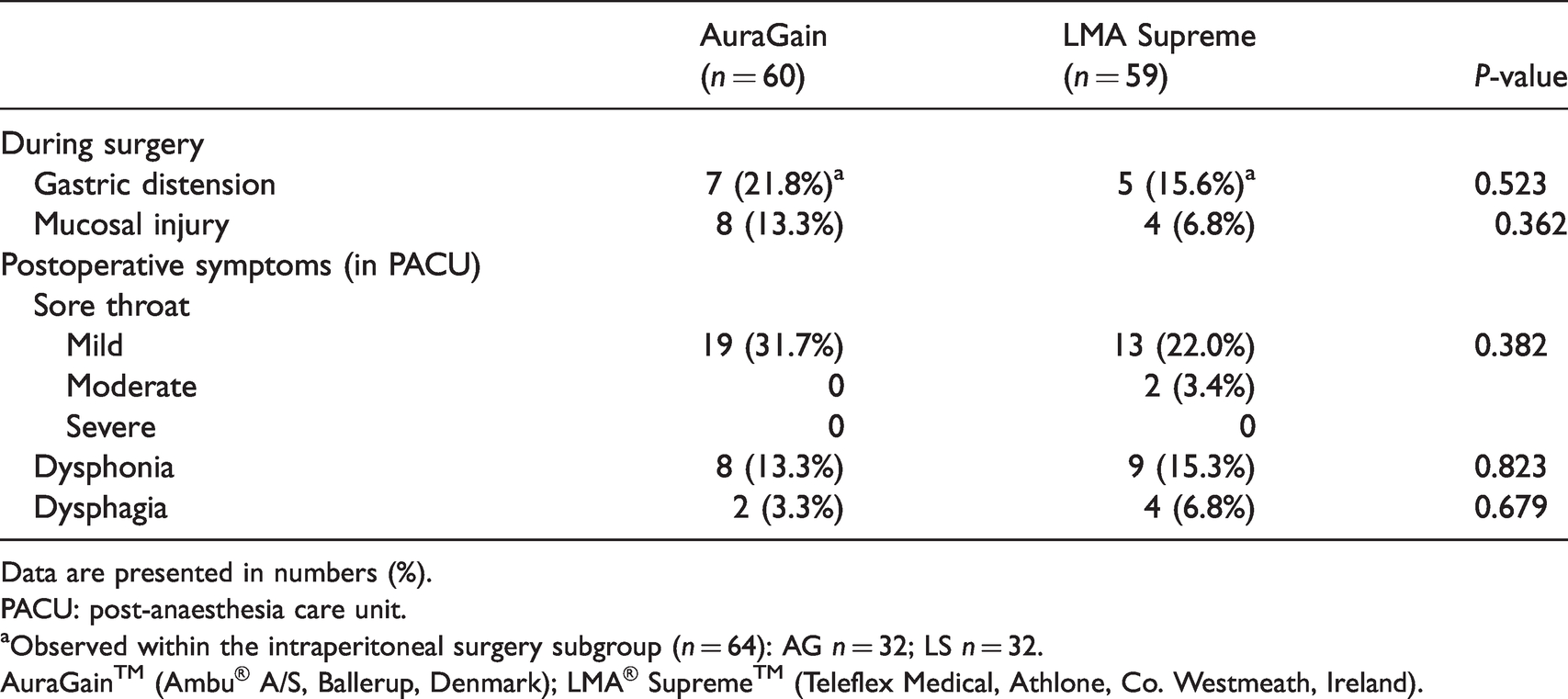
Data are presented in numbers (%).
PACU: post-anaesthesia care unit.
aObserved within the intraperitoneal surgery subgroup (n = 64): AG n = 32; LS n = 32.
AuraGain™ (Ambu® A/S, Ballerup, Denmark); LMA® Supreme™ (Teleflex Medical, Athlone, Co. Westmeath, Ireland).
Discussion
In our study, the AG achieved slightly higher OLPs than the LS. The ability to maintain adequate ventilation through the SGD following CO2 insufflation is an important consideration as the OLP should be high in order to withstand the assault of increased airway pressures during pneumoperitoneum or pneumo-extraperitoneum in herniorrhaphy. When the airway pressure exceeds the OLP, peri-cuff leak might result in inadequate ventilation. This may also result in potential gastric distension, increasing the risk of regurgitation and aspiration. The slightly higher OLPs conferred by the AG may provide a slightly greater margin of safety during laparoscopic surgery. Although CO2 insufflation during preperitoneoscopic inguinal herniorrhaphy is more localised and confined to the extraperitoneal space, the resultant respiratory effects are similar to those from pneumoperitoneum. Cephalad displacement of the diaphragm and reduced diaphragmatic excursion in the Trendelenburg position causes decreased lung compliance with a resultant increase in PIP, 13 in addition to the need to increase minute ventilation due to systemic CO2 absorption. In our study, the recorded PIP changes were similar in the subgroups at each of the timepoints measured. As such, the airway pressure stressors imposed on the SGDs by pneumoperitoneum during intraperitoneal surgery in reverse Trendelenburg position and pneumo-extraperitoneum during extraperitoneal surgery in the Trendelenburg position are likely to be comparable and may be considered to have similar implications on the primary outcome.
Our results are similar to the study by Lopez et al., who compared the AG and LS in 60 patients undergoing laparoscopic gynaecological surgery. 14 The mean (SD) OLP of the AG was higher than the LS (34 (5) cmH2O versus 29 (5) cmH2O; P = 0.0002). Wong et al. also demonstrated better OLP with the AG than the LS (mean (SD) 26.4 (3) cmH2O 21.6 (3) cmH2O, difference in means 4.8 cmH2O, P < 0.001) in 165 adult patients presenting for ambulatory surgery. 15 A recent meta-analysis of the use of SGDs in laparoscopy reported the highest OLP with the AG before pneumoperitoneum. 16 However, no significant difference between the AG and LS was demonstrated in another study performed in 100 patients in a South-East Asian population. 17
Fewer intraoperative device failures were observed with the AG than the LS. One patient in the AG group and three patients in the LS group required eventual tracheal intubation as the large peri-cuff leak could not be resolved despite adjustments, bringing the overall perioperative success of the AG and the LS to 95% and 89.8%, respectively. While no statistical significance was detected, our study was not adequately powered to detect or exclude differences in our secondary outcomes. Previous studies reported the need for device adjustment post-pneumoperitoneum with the LS, but not with the AG.4,14 However, there was no documented device failure requiring tracheal intubation. Possible reasons for intraoperative device failure in our study include older patient age 18 (the four patients were aged between 59 and 73 years), male gender, 18 a lack of dentition with a change in jaw tone which in turn affects device stability, and proceeding with surgery with an OLP of less than 20 cmH2O. Although OLP of less than 20 cmH2O was reported to be generally safe and able to provide effective positive pressure ventilation,12,19 achieving an OLP of more than 20 cmH2O remains recommended for laparoscopic surgery due to the raised airway pressures secondary to CO2 insufflation. Despite both SGDs being able to provide comparable ventilation and safety, performance factors such as OLP, the need for frequent adjustments and risk of intraoperative device failure should be taken into consideration during device selection.
Effective ventilation could be achieved via both the AG and the LS. Notwithstanding this, audible gastric insufflation was noted in 8%–10% of patients at the OLP. The laparoscopic surgeons reported visible gastric distension in 15%–21% of patients undergoing intraperitoneal surgery intraoperatively, despite the nasogastric tube being placed on passive drainage. However, this assessment was subjective and we can draw no conclusions about relative gastric insufflation incidence between the two devices from this study. Although no cases of regurgitation or aspiration occurred in our study, aspiration risks could increase with prolonged surgery. Anaesthetists should be mindful of gastric insufflation when performing positive pressure ventilation through SGDs. Routine nasogastric tube insertion via the SGD for gastric decompression should be considered. In our opinion, placing the nasogastric tube on active intermittent suction intraoperatively is useful for continuous gastric decompression, hence reducing the risk of regurgitation.
Similar to other studies,15,17 we found that the AG was a little more difficult to insert with a longer time for insertion than the LS. The wide-bore airway tube of the AG allows direct bronchoscopy-guided intubation when necessary, resulting in a more prominent shape of the back of the cuff, which probably confers better perilaryngeal seal. 14 However, the increased bulk and stiffness contributes to the difficulty in negotiating the device past the posterior pharyngeal wall. However, the clinical relevance of a 4-s difference remains questionable.
While there was no statistically significant difference in leak volume (in ml) between inspired and expired tidal volumes between the two devices, we observed a difference of the same magnitude as the difference in OLPs (>10%). This was most apparent immediately after CO2 insufflation, with the difference becoming smaller at 30 minutes into surgery. Given the lack of power, a true difference in leak volume cannot be confirmed or excluded.
Our study found no significant difference in the postoperative pharyngolaryngeal complications between the two SGDs. While the incidence of sore throat with the LS was within the published range of 2%–56.7%,20,21 we found a high incidence of sore throat of 31.7% with the AG. However, only two patients complained of moderate sore throat, whereas the remaining 29 patients only had mild sore throat. Earlier studies reported the incidence of sore throat with the AG to be 6.5%–10%.14,17,22 Our finding was more consistent with a recent study, which demonstrated the composite pharyngolaryngeal complications to be 32% 15 with the AG. Possible explanations for the high incidence include increased difficulty in insertion and increased perilaryngeal as well as pharyngeal pressures exerted by the bulky cuff. The cuff sizes for the LS are the same for sizes 4 and 5, while a size 5 AG has a larger cuff than that of a size 4. A cadaver study studying the in vivo fit of SGDs using a lateral neck X-ray suggested that the size of the AG cuff was not appropriate for the estimated height and weight of the cadavers. 23 For our study, sizing of the SGD was based on the patient’s body weight, as per the manufacturer’s recommendation. As the Asian population has a smaller build, a smaller mouth opening and possible smaller hypopharyngeal volume, it is possible that our size selection was not best suited for some patients, causing them to experience sore throat postoperatively.
There were several limitations to our study. Firstly, our study was performed in non-obese patients (mean BMI was 24 kg/m2). The results obtained may not reflect the performance of these SGDs in more obese patients during similar surgeries. Secondly, as with all airway studies, the investigators were not blinded to the device allocation, and this might result in potential reporting bias, based on their previous experience with the devices. Finally, in retrospect the SGDs that exhibited an OLP of less than 20 cmH2O should have been removed and repositioned, regardless of the adequacy of ventilation, to enable a better seal to be obtained for safer positive pressure ventilation. Repositioning these SGDs might also impact the mean OLP obtained for each device. Despite this, our study demonstrated a satisfactory safety profile with both devices for all patients studied.
In conclusion, we found a small difference in OLP between the AG and the LS during laparoscopic surgery and preperitoneoscopic inguinal herniorraphy with CO2 insufflation. However, the AG was slightly more difficult to insert and required a longer time for insertion. The higher OLPs suggest that the AG may facilitate the use of higher PIP during such surgery.
Footnotes
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author Contribution(s)
Declaration of conflicting interest
The author(s) have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.