
Abstract

Despite the reported benefits of multimodal surgical prehabilitation, it has not been widely implemented in many hospitals. We would like to share our experiences and challenges in successfully piloting a patient-centred prehabilitation programme at our hospital.
The Prince Charles Hospital, Brisbane, Australia is a quaternary level cardiothoracic referral centre that performs approximately 100 elective major abdominal surgical procedures per annum. This project was approved by the hospital ethics committee as a quality assurance activity (Project ID: 52719) with funding (A$30,276) obtained from Metro North Hospital and Health Service, Queensland, Australia to implement the programme in up to 20 patients with cancer.
Our small multidisciplinary prehabilitation team comprised physiotherapists, dietitians, social workers, pre-anaesthetic clinic nurses, a consultant anaesthetist and surgeons. Patients scheduled to undergo major abdominal surgery with a proposed surgical date after a minimum of two weeks, were referred by the surgeons and seen by the allied health team during their pre-anaesthetic appointment. Details of the allied health initial assessment items, findings and management are listed in Table 1. The physiotherapist prescribed preoperative exercise to all participants with a choice of three options: individualised Home Exercise Programme only (with phone follow-up and support available) ± attendance at once weekly, or twice weekly individualised face-to-face, hour-long exercise sessions, involving a combination of aerobic and resistance exercises.
Details of prehabilitation: initial assessment results and allied health management
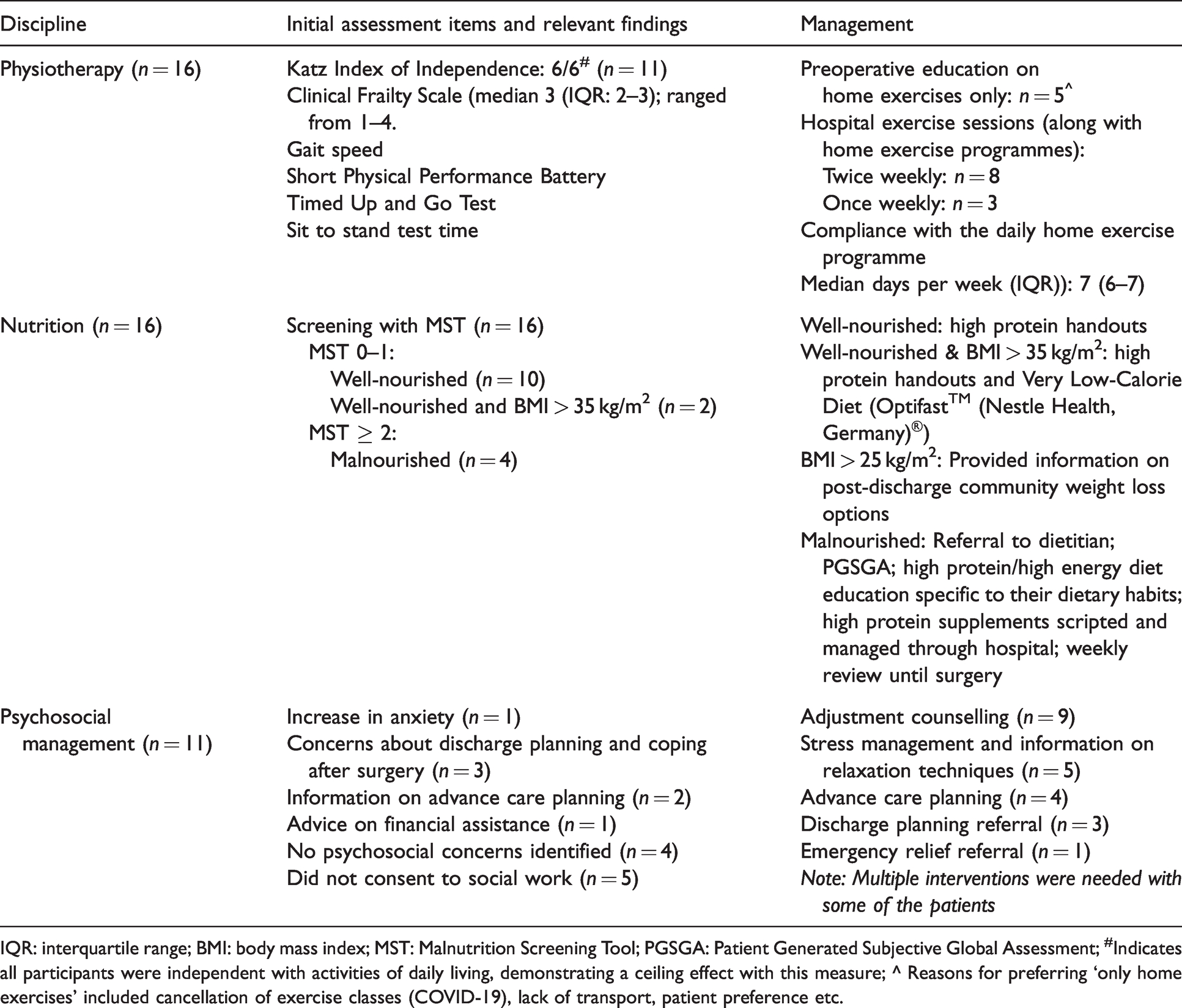
IQR: interquartile range; BMI: body mass index; MST: Malnutrition Screening Tool; PGSGA: Patient Generated Subjective Global Assessment; #Indicates all participants were independent with activities of daily living, demonstrating a ceiling effect with this measure; ^ Reasons for preferring ‘only home exercises’ included cancellation of exercise classes (COVID-19), lack of transport, patient preference etc.
With nutritional assessment, if the Malnutrition Screening Tool (MST) 1 on arrival was either 0 or 1 (‘not at risk’), patients were provided education resources on basic healthy eating with a focus on high protein leading up to surgery. 2 If the MST scores were 2 or more (‘at risk’), the prehabilitation dietitian completed a Patient Generated Subjective Global Assessment and provided individualised recommendations based on European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines. 3
Participants completed a locally designed psychosocial screening tool to assess their level of psychological distress in response to their diagnosis and to determine any other psychosocial stressors that impacted their ability to cope. Following the assessment, the social worker provided personalised psychosocial interventions (Table 1), followed by postoperative telephone interviews to receive participants’ feedback. As well as collecting information on clinical outcomes, participants’ overall satisfaction with the programme and their willingness to be involved in designing a future prehabilitation programme were assessed at the final session.
Sixteen patients, ten males and six females (median age: 70 years, range 35–91) undergoing major gastrointestinal surgery were enrolled in our pilot prehabilitation programme between August 2019 and July 2020. The prehabilitation programme did not result in any surgical delay and was efficiently delivered during their waiting period. Despite the limited time available, we observed a significant improvement in the median (interquartile range (IQR)) scores of gait speed (m/s) (from 1 (0.9–1) to 1.35 (1–1.5); P = 0.004), Short Physical Performance Battery (SPPB) 4 (from 11 (9.5–12) to 12 (12–12), P = 0.047), sit-stand test time (s) (from 11 (9.1–11.9) to 8.4 (7–10.2); P = 0.006) and Timed Up and Go (TUGT) 5 (s) (from 6.71 (5.65–8.4) to 6.33 (5.33–7.72); P = 0.02). There was one case of pleural effusion, but no other major postoperative adverse events, deaths or intensive care unit admissions. Median length of hospital stay was 8.5 days (range: 2–50; n = 16). Within these 16 patients there were two outliers: one patient had a complex surgical procedure with postoperative Takotsubo cardiomyopathy and stayed for 50 days; the other had a very large incisional hernia repair but was discharged in two days.
Feedback from the participants informed us that the participants valued the holistic approach of the prehabilitation programme and credited the availability of support from healthcare professionals; this reduced their apprehensions around surgery and built their confidence while anticipating their surgery. They felt that being physically and emotionally prepared made a big difference, with many identifying that the exercise programme not only helped them with their physical recovery but also assisted them from a mental health perspective. All our participants were fully engaged, attended all gym sessions, and rated the programme highly (Table 2). Overall project costs inclusive of staff costs, promotional materials, parking tickets and fitness trackers (Fitbit Inspire®, Fitbit Inc., San Francisco, CA, USA) came to approximately A$13,966. This pilot project was aimed to test the feasibility of running such a programme in our hospital; with only a small number of patients, it was not powered to evaluate any impact in terms of financial outcomes, length of stay or quality of life measures.
Survey on patient experience and satisfaction with the prehabilitation programme
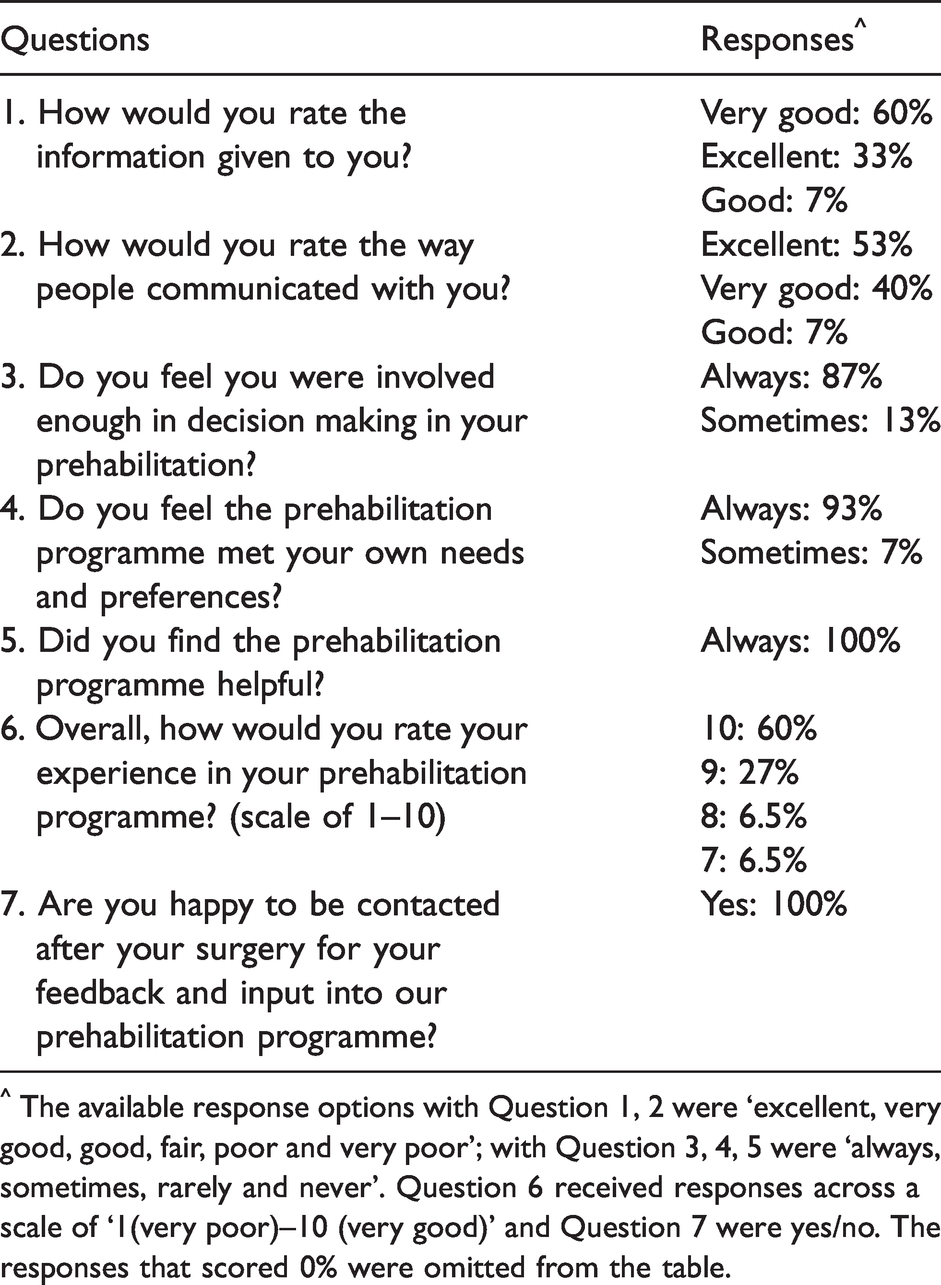
^ The available response options with Question 1, 2 were ‘excellent, very good, good, fair, poor and very poor’; with Question 3, 4, 5 were ‘always, sometimes, rarely and never’. Question 6 received responses across a scale of ‘1(very poor)–10 (very good)’ and Question 7 were yes/no. The responses that scored 0% were omitted from the table.
We relate the success of our programme to the measures we adopted to ensure patient compliance including (a) creating an individualised programme tailored to participants’ needs and preferences, (b) measures to check compliance such as attendance at exercise classes, number of steps recorded, exercise diaries and phone follow-ups, (c) integrating prehabilitation sessions with planned hospital visits as cost- and time-effective measures, (d) providing free parking tickets for patient hospital visits, and (e) uninterrupted service during COVID-19 hospital lockdown with tele-health consultations. We organised the first session at the earliest time slot after the day of cancer diagnosis to maximise the prehabilitation time and encouraged the presence of a support person for better understanding. We had involved social workers rather than psychologists in our programme. We also actively promoted our programme through videos, hospital news bulletins, presentations in hospital grand rounds, surgical and executive meetings, and engaging surgeons in the programme, to ensure we got rapid buy-in from all relevant stakeholders.
With limited funding and time availability for prehabilitation, our programme managed to achieve meaningful improvements in patients’ functional status, and had high patient compliance and satisfaction with the programme. We hope others interested in commencing a surgical prehabilitation service at their facility can benefit from our published experience.
Footnotes
Author contributions
Acknowledgements
We would like to thank Lisa Woolcock and Suzanne Main from Department of Social Work, Nicole Conway and Elizabeth Aitken from Surgical OPD and PREAC The Prince Charles Hospital, Brisbane, Australia for their kind support. We acknowledge the statistical assistance provided by Dr. Stephanie Yerkovich from The Prince Charles Hospital Foundation, Brisbane.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Funding for this programme was provided by the Metro North Hospital and Health Service, Queensland, Australia as a seed grant.