
Abstract
There are no published data on the age of retirement of anaesthetists in Australia and New Zealand. We surveyed 622 retired Fellows of the Australian and New Zealand College of Anaesthetists to determine their ages of complete retirement from clinical practice, demographics, and whether they had retired at the age they had intended to retire. We also aimed to explore factors affecting the decision to retire, the practice of ‘winding down’, common post-retirement activities, and the arrangement of personal and professional affairs. Responses were received from 371 specialists (response rate 60%). The mean (standard deviation) age of retirement was 65.2 (6.9) years. The mean (standard deviation) retirement ages ranged from 62.0 (7.1) years (those who retired earlier than planned) to 68.2 (4.3) years (those who retired later than they had intended). The mean (standard deviation) age of retirement of the male respondents was 66.0 (6.5) years, and for female respondents was 62.7 (7.7) years. Two hundred and thirty-three respondents (63%) reported winding down their practice prior to retirement, and 360 (97%) had made a will. Poor health and loss of confidence were the two most common factors in the retirement decisions of those who retired earlier than they had planned. Our results may assist current practitioners plan for retirement, and suggest strategies to help health services, departments and private groups accommodate individuals in winding down their practice.
Introduction
Retirement is one of the important transitions we make in our lives. For some doctors, the decision to retire is difficult; for others, retirement is welcomed. Each doctor makes an individual decision, based on his or her own situation and experience. Predicting the timing of retirement, and the factors which influence that decision, are important for both individuals, health services, public hospital departments, and private groups when planning for the future.
The formal definition of a retired person used by the Australian Bureau of Statistics is someone who had ‘previously worked and had retired from work or looking for work, and did not intend to look for, or take up, work in the future’. 1 The Australian and New Zealand College of Anaesthetists (ANZCA) defines a Fellow as ‘fully retired’ when they have ‘ceased practising all forms of clinical medicine, medicolegal work and clinical support activities (such as administration, teaching and research)’. 2 Current workforce surveys collect information on the intended age of retirement; however, actual retirement may subsequently occur at an earlier or later date than the stated intended age. There is currently inadequate information related to ‘winding down’, which refers to the deliberate reduction in hours, or change in nature of work in anticipation of retirement. 3 , 4 Previous papers have published retirement ages of medical practitioners (including anaesthetists) working in the United Kingdom 5 and the United States. 6 However, there exist no published data specifically regarding the retirement ages of ANZCA Fellows who were working in Australia and New Zealand.
The aim of this survey was to determine the actual retirement ages of anaesthetists and pain medicine specialists registered as ‘retired’ by ANZCA and its Faculty of Pain Medicine. We collected data on their age of complete retirement from clinical practice. In addition, we aimed to report on the demographics of the population, factors involved in the decision to retire, the practice of ‘winding down’ prior to retirement, common post-retirement activities, the arrangement of personal and professional affairs and recommendations to colleagues contemplating retirement.
Materials and methods
Ethics approval was provided by the human research ethics committee of the Royal Brisbane and Women’s Hospital (LNR/2019/QRBW/54312). The target population was those ANZCA Fellows registered as retired. The survey was developed by the authors based on literature review and expert opinion. An earlier version of the survey was piloted in 2016 by the first author and the responses of 204 retired Australian Society of Anaesthetists members (unpublished data) were used to refine the questions of the current survey. The survey link was distributed by the Clinical Trials Network of ANZCA, and consent was implied by the voluntary completion of the survey. Respondents were reassured their responses would be de-identified. A single reminder email was sent six weeks later if an initial response had not been received. Demographic information was collected, including age, sex, country of residence, the country in which their anaesthesia training was undertaken, the country or countries in which they had worked in the past ten years, and details of their anaesthesia qualifications. Respondents were asked to state their age at complete retirement from clinical practice and whether they had retired at the time at which they had intended to retire, or whether they had retired earlier or later than they had planned. They were asked to rank the three most important reasons for their retirement, and whether or not they had actively wound down their practice. Winding down was defined in the survey as ‘a reduction in hours of clinical work, or a change in work pattern’ prior to complete retirement (see Supplementary Appendix). Further questions were on activities after retirement, and arrangements they had made for their personal and professional affairs. The full survey questions can be viewed in the Supplementary Appendix.
The sample was one of convenience, based on the response rate of the predefined target population. Demographics of the respondents were summarised using descriptive statistics. Results of interest were analysed using the χ2 or Fisher’s exact test when appropriate, and significance was set at P<0.05. Responses to survey questions were presented as numbers (percentages).
Results
The survey was distributed to the target population of 622 retired anaesthetists/pain medicine specialists in November 2019. A total of 371 surveys were returned by 29 March 2020 (response rate 60%). Of the 371 respondents, 370 were retired anaesthetists and one was a retired pain medicine specialist. The mean (standard deviation, SD) age of respondents was 72.3 (7.4) years, range 37.0–93.0 years. Two hundred and eighty-seven (77%) respondents were men and 84 (23%) were women. The mean (SD) age of the male respondents was 73.0 (6.5) years, range 37.0–89.0 years, and of the female respondents it was 68.5 years (9.2) years, range 46.0–93.0 years. Tables 1 and 2 show the current country of residence, the country (or countries) in which the respondents had worked in the past ten years of practice, the country in which their primary anaesthesia qualification(s) were obtained, and their qualifications. In the past ten years of their practice, 309 respondents had been working in Australia (83%) and 44 had been working in New Zealand (12%).
Residence, work and qualification details of 371 retired specialists, Australia and New Zealand.
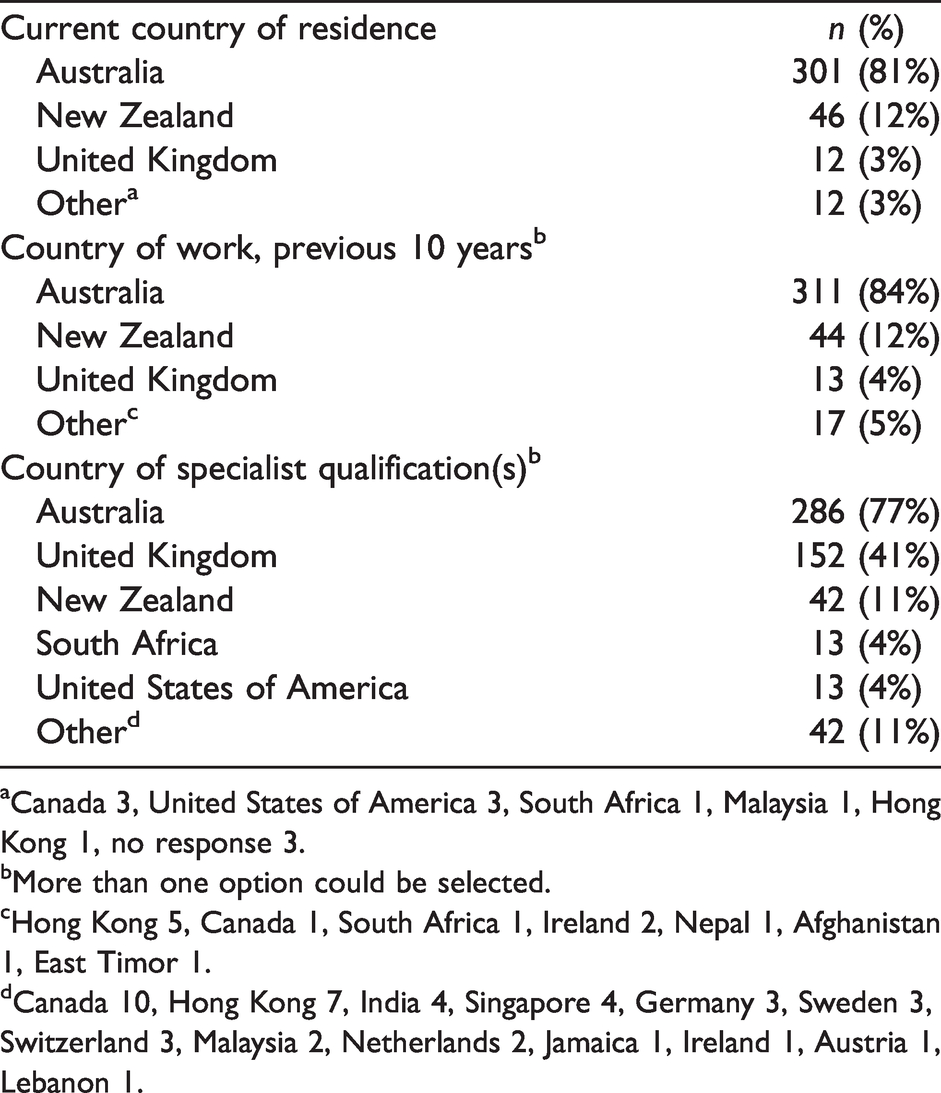
aCanada 3, United States of America 3, South Africa 1, Malaysia 1, Hong Kong 1, no response 3.
bMore than one option could be selected.
cHong Kong 5, Canada 1, South Africa 1, Ireland 2, Nepal 1, Afghanistan 1, East Timor 1.
dCanada 10, Hong Kong 7, India 4, Singapore 4, Germany 3, Sweden 3, Switzerland 3, Malaysia 2, Netherlands 2, Jamaica 1, Ireland 1, Austria 1, Lebanon 1.
Qualifications of 371 retired specialists, Australia and New Zealand.
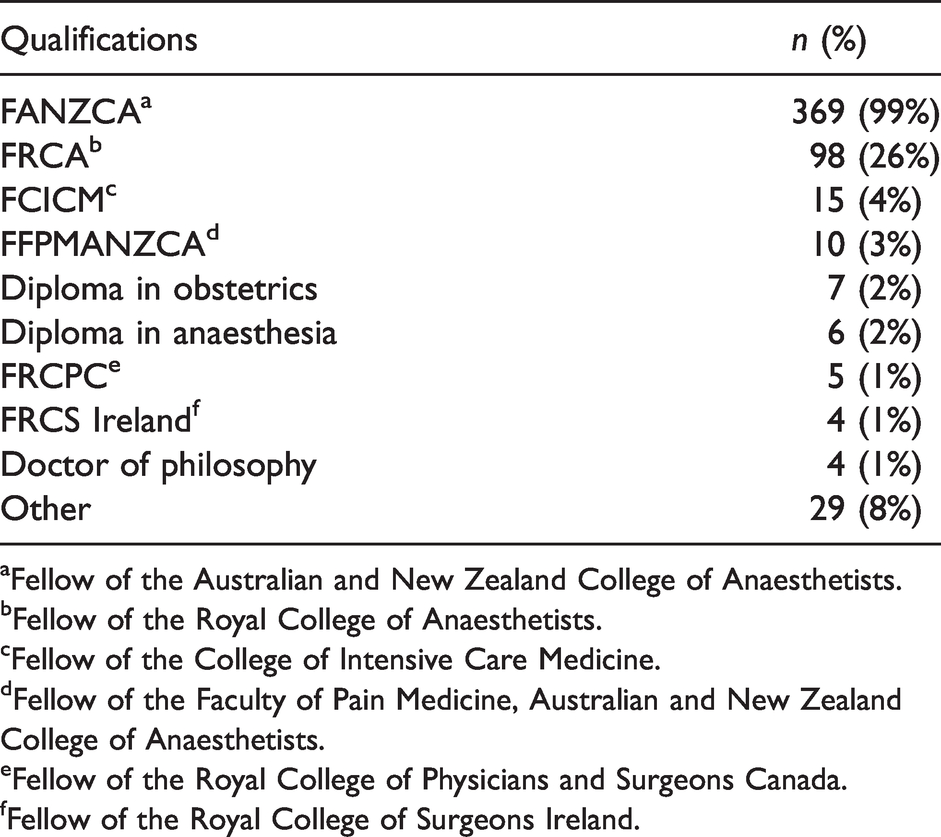
aFellow of the Australian and New Zealand College of Anaesthetists.
bFellow of the Royal College of Anaesthetists.
cFellow of the College of Intensive Care Medicine.
dFellow of the Faculty of Pain Medicine, Australian and New Zealand College of Anaesthetists.
eFellow of the Royal College of Physicians and Surgeons Canada.
fFellow of the Royal College of Surgeons Ireland.
Age of retirement from clinical practice
The mean (SD) age of retirement (AOR) of all respondents was 65.2 (6.9) years. Excluding the 12 anaesthetists who retired under 50 years of age, the mean (SD) AOR was 66.0 (5.5) years. The mean (SD) AOR of all the male respondents was 66.0 (6.5) years (range 37.0–78.0); 32 (11%) retired under the age of 60 years. The mean (SD) AOR for all female respondents was 62.7 (7.7) years (range 44.0–80.0). Seventeen respondents (5%) retired under the age of 55 years.
Two hundred and forty-nine (67%) of all respondents retired at the age they intended to retire. The mean (SD) AOR of those respondents was 66.0 (6.8) years (range 32.0–80.0). The mean (SD) AOR of those 86 (23%) respondents who retired earlier than they intended to was 62.0 (7.1) years (range 44.0–78.0). The mean (SD) AOR of the 48 (13%) respondents who retired later than they intended to was 68.2 (4.3) years (range 59.0–77.0). Figure 1 shows the age distribution of those who retired when intended, later than intended and earlier than intended. The mean (SD) AOR of the 309 respondents working in Australia in their past ten years of practice was 65.2 (7.0) years and of the 44 respondents working in New Zealand was 67 (7.6) years.
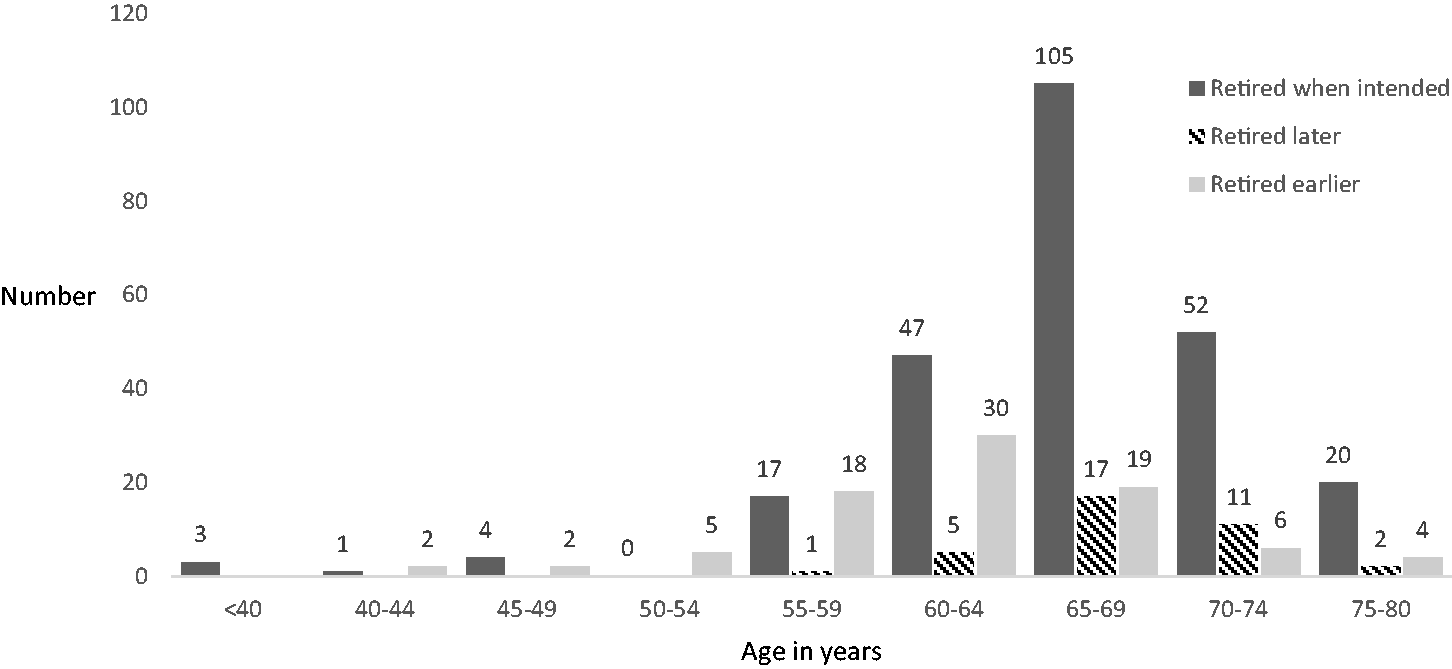
Frequency histogram showing the age in years of 371 retired specialists who retired when intended (solid dark), later than intended (striped) and earlier than intended (solid light).
Of the 53 (14%) respondents who retired before the age of 60 years, ten (19%) had lost confidence, and 13 (25%) retired under 60 years of age because of poor health. Thirty-two (11%) male respondents had retired under the age of 60 years: one, aged 32 years, because of stress; two, aged 35 and 36 years, had gone on to other careers, and five had retired in their 50s to go onto other careers. Two men in their 50s had retired later than they had planned. Two wanted to ‘quit while they were ahead’. Twenty-three female specialists had retired under the age of 60 years: five for family reasons, and one aged 46 years, who had retrained in another specialty. One aged 59 years felt ‘burnt out’. Six respondents were ‘tapped on the shoulder’, one after clinical airway incidents. One had to retire at 70 years because of a private hospital policy. Two respondents aged 65 and 78 years had found it difficult to maintain continuing professional development (CPD) requirements. Barriers to retiring at the respondents’ planned age included financial reasons: ‘insufficient financial resources’ (ten, 5%); ‘loss of income’ (three, 1.5%); loss of prescribing rights (six, 3%); ‘no other activities’ to occupy his or her time (four, 2%); and loss of status: ‘who will I be if not a doctor?’ (three, 1.5%). A few respondents reported the negative aspects of retirement: there was ‘nothing else to do’, ‘no other activities to occupy me’. Table 3 shows the most important reasons for retirement in those who retired at their intended age, those who retired later than intended, and those who retired earlier than intended. Of those who retired earlier than intended, the most common reason for retirement was ‘poor health’ (34, 40%). Loss of confidence was a factor in 25 (29%) respondents who retired earlier than planned, in 14 (6%) of those retiring when intended, and eight (22%) of those retiring later than intended: this difference was statistically significant (χ2 35.05, P<0.001).
Reasons for retiring, 371 retired anaesthetists and pain medicine specialists (the three most important reasons were requested).
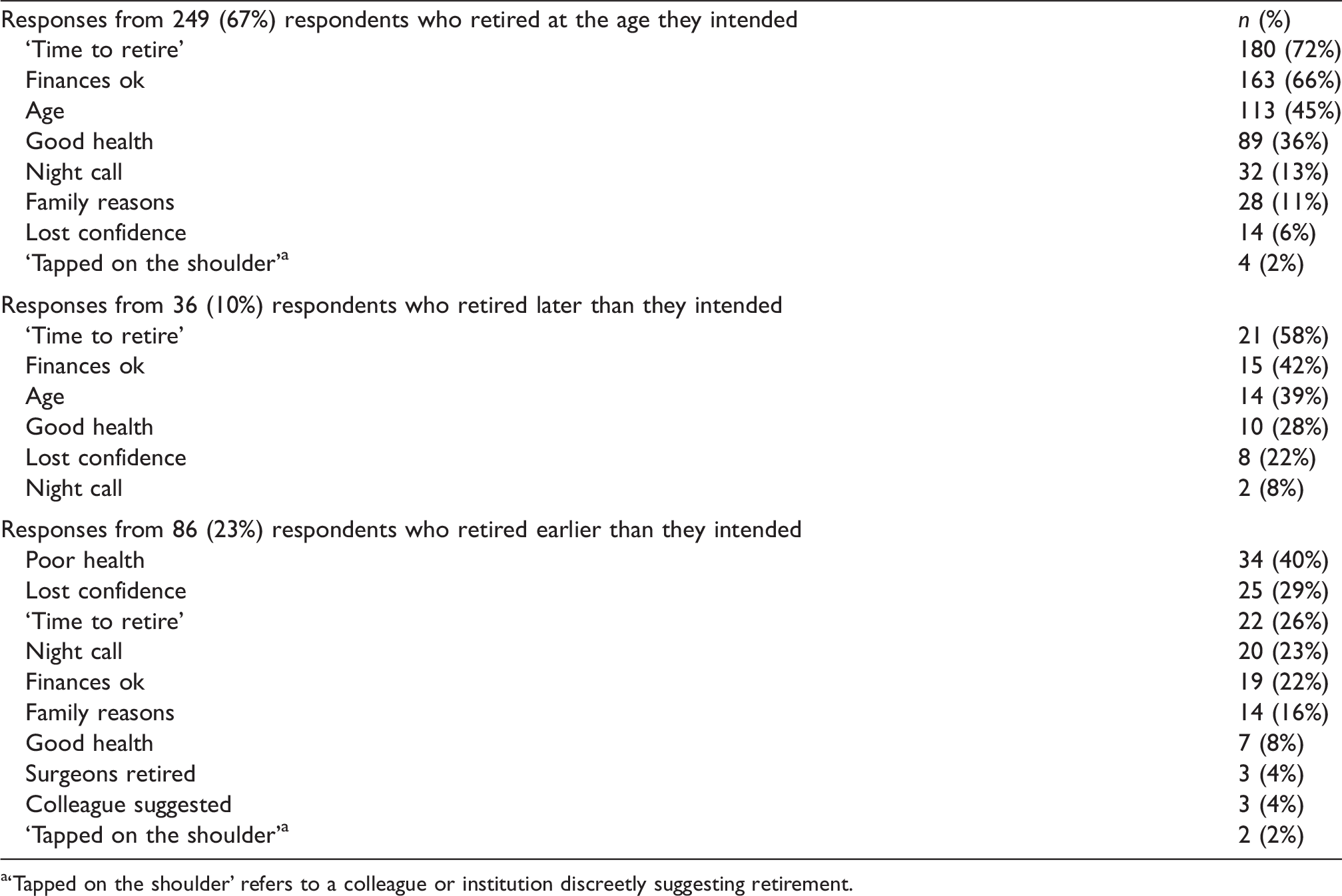
a‘Tapped on the shoulder’ refers to a colleague or institution discreetly suggesting retirement.
Type of practice
Respondents were asked the nature of their practice in the past ten years of their working life: 130 (35%) were in private practice, 127 (34%) were in public practice, and 113 (30%) practised in a combination of both public and private practice. The mean (SD) AOR of those respondents in solely private practice was 66.8 (6.5) years. For those in solely public practice, the mean (SD) AOR was 63.7 (7.2) years. For those who worked in both public and private practice, the mean (SD) age at retirement was 65.3 (6.7) years. Two hundred and thirty-three (63%) respondents had worked less than full time (‘winding down’) before fully retiring and the age of these respondents ranged from 45 to 80 years. The length of time respondents had wound down is shown in Figure 2.
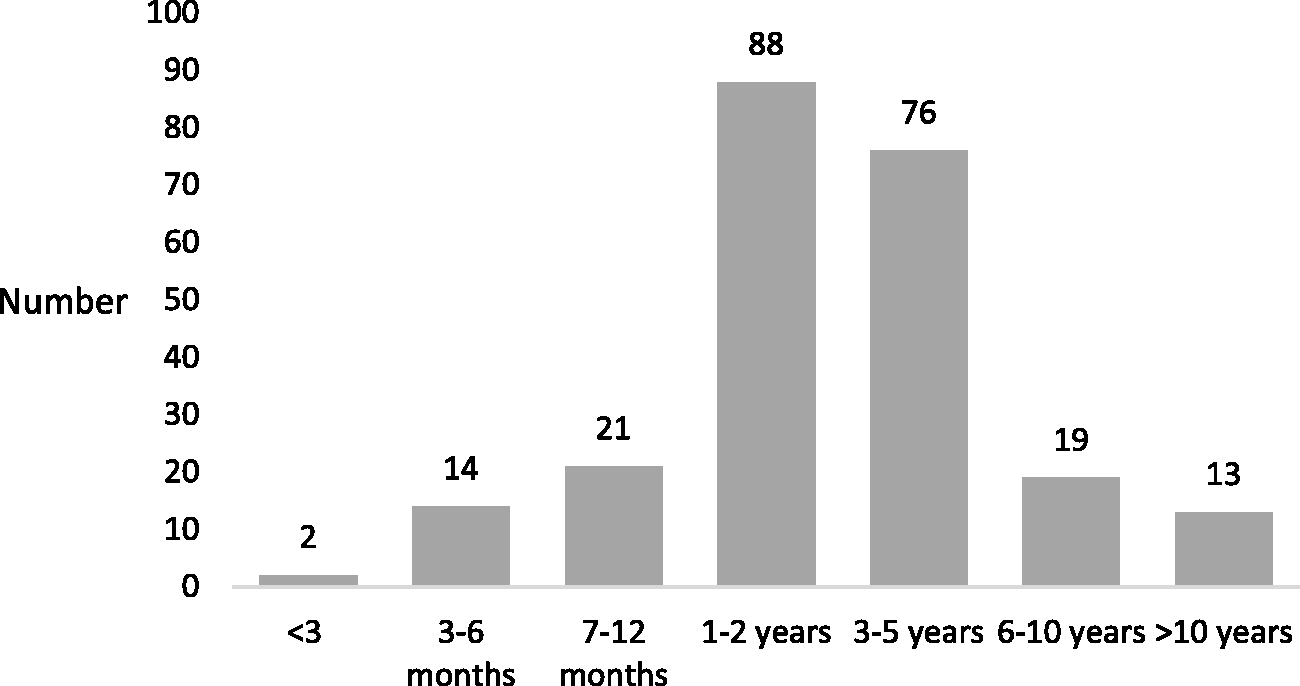
The period of time spent ‘winding down’ from full-time practice of 233 retired specialists. Winding down refers to a reduction in hours of clinical work, or a change in work pattern.
Personal and professional affairs
One hundred and sixty-one (43%) respondents reported retaining their membership of a medical defence organisation (MDO). One hundred and forty-four (89%) provided reasons for this, which included for the protection of run-off cover (44, 27%), for Good Samaritan cover (26, 16%) and for the benefit of the travel insurance provided by their MDO (24, 15%). Several respondents reported that they were still working in medicine in various positions, including non--anaesthesia-related clinical work, as well as research, assessments and education; other work included advisory, medicolegal, committee and board work.
One hundred and twenty-one (32.6%) respondents remained on the medical register of either the Australian or New Zealand regulatory body. Reasons for this were provided by 111 (92% of 121). Reasons included still working in medicine, unwilling to lose their status as a doctor (18, 15%) and wishing to continue to write prescriptions and make referrals to specialists (23, 19%). Table 4 shows the numbers of respondents who had completed various tasks related to arranging their personal affairs, respondents’ activities in retirement and advice from respondents for those considering retirement.
Numbers and percentages of respondents who had undertaken tasks related to their personal affairs (n=371); respondents’ activities in retirement and their advice to those planning retirement (n=369).
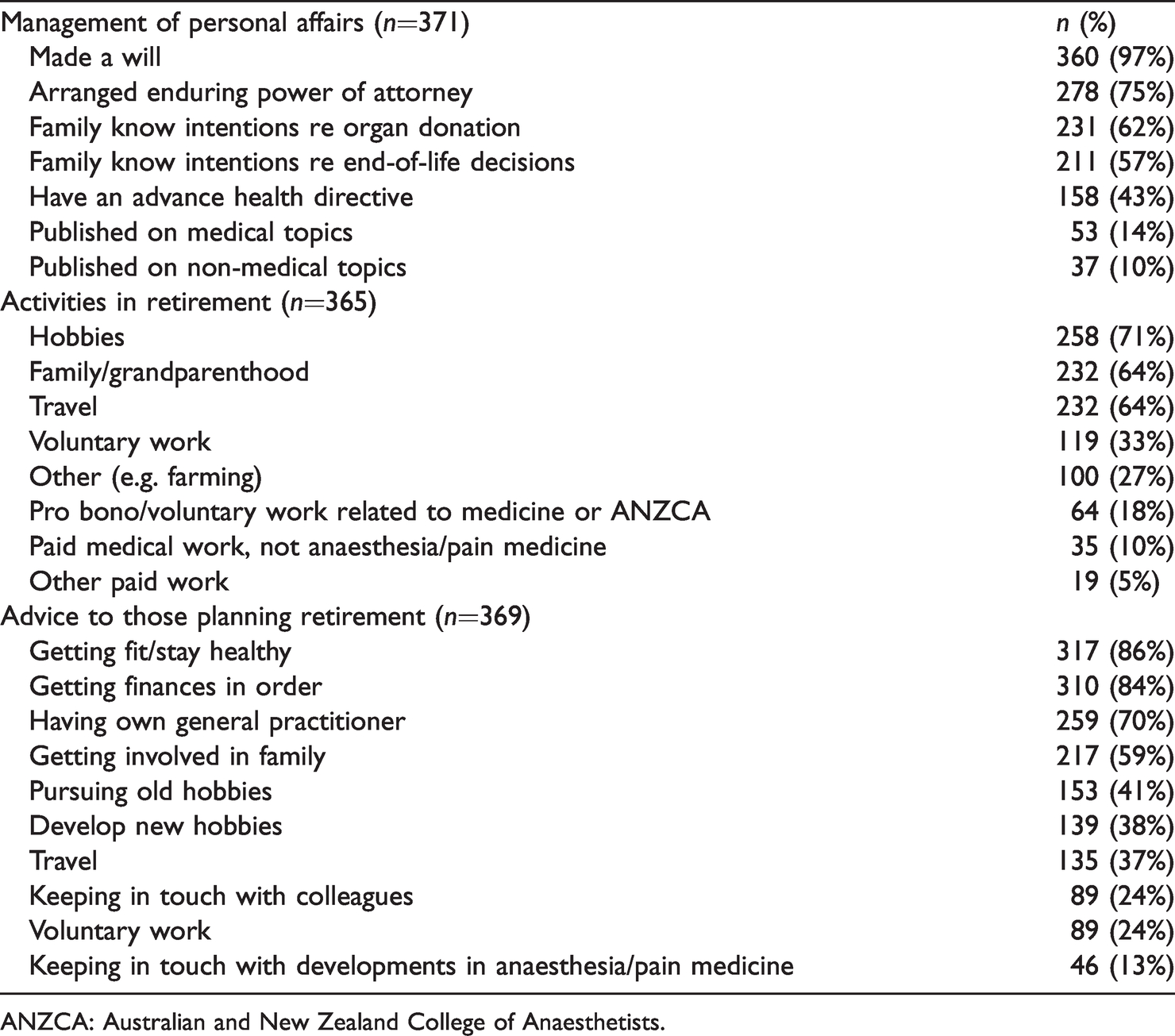
ANZCA: Australian and New Zealand College of Anaesthetists.
Discussion
The majority of respondents had retired at their intended age. The average AOR ranged from 63 years (female respondents) and 67 years (those in solely private practice). Four respondents who retired under the age of 50 years had gone on to practice in other fields. Reasons for retirement of those who retired when they intended, and those who retired later than planned, were similar. Poor health was a major factor in early retirement, while loss of confidence was also significantly more important for those retiring earlier than planned.
Our results show that night call was a reason for retirement in all three categories (intended age, earlier than intended and later than intended). This suggests that night call and its fatigue-generating tendency is variably tolerated, with some individuals more affected than others by disruptions to their diurnal cycle. 7 Night call may also require anaesthetists to supervise or provide direct care for a wide variety of cases, which they may not feel comfortable managing. Many chose to retire later than age 65 years because they had good health and were enjoying their work. Others decided to retire before they made a serious clinical error that could be attributed to age: ‘better a year too early than a day too late’. These doctors displayed the insight we hope all our treating physicians possess! Voluntary free-text responses revealed some respondents wanted to avoid a tap on the shoulder, suggesting that they were aware of, and had insight into, the effects of ageing.8–10
The majority of our respondents had reduced their workload for a range of periods before retiring, from less than three months to over ten years. Several respondents retired much earlier than the average AOR in our survey, at less than 50 years of age. Some had changed careers and one had retired due to stress. While the details relating to these respondents are limited, there are multiple plausible reasons for such early retirement, including changes in mental health and wellbeing, relationship or family responsibilities, and perhaps seeking a better life balance. We have demonstrated that a significant fraction of anaesthetists elected less than full-time employment and this information may help departments plan for members’ changing participation in the workforce in their later years. Winding down, or a structured transition to retirement, may consist of a reduction in total work hours, reduction or cessation of night call responsibilities, reduction in clinical case acuity or a cessation of work in the operating theatre environment. 3 Absorbing such changes in public departments or private groups of various sizes is likely to be easier if anticipated ahead of time.
Over a third of respondents had retained their medical indemnity cover—mostly for reasons of run-off cover, Good Samaritan cover, medicolegal work, and to retain their travel insurance. MDOs in Australia are required by federal law to provide run-off cover for their retired practitioners, irrespective of the age of the retiree, and these retired practitioners are therefore not required to pay further MDO fees. 11 Good Samaritan cover, cover for medicolegal work, and retention of prescribing and referral rights, require ongoing payment of annual MDO fees. A third of respondents had retained their medical registration with the relevant regulatory authority; some retained this registration for status reasons (‘who am I if not a doctor?’), while others retained it for the ability to write prescriptions and referrals. Current regulatory bodies encourage all doctors to have their own general practitioner, and writing prescriptions and referrals for oneself or for family members is not a recommended practice. 12 , 13 Such activities in retirement would only be covered if MDO membership is retained. 11
The majority of respondents were residing in Australia and New Zealand at the time of survey completion. However, our results regarding retirement age are similar to those in the literature relating to medical practitioners in other countries. The Royal College of Physicians in the UK reported in 2015 that 40% of their specialists and trainees intended to retire at 60 years of age, and a further 32% at 65 years of age. 14 Wijeratne et al. conducted a survey of doctors in Australia aged 55 years or greater, and found that the intended AOR was lower in surgeons and anaesthetists compared with other specialties, with the highest intended retirement age identified in general practitioners and psychiatrists. 15 This may indicate that proceduralists acknowledge the effect of age-related changes on their practice, more so than non-proceduralists. However, it may also reflect the potential financial security differences between the two groups. In the same paper, respondents who had greater work centrality and greater emotional resources were less likely to intend to retire. Those with financial security and who had anxiety about ageing were more likely to intend to retire, while Peisah et al. speculated that attaining higher levels of psychological comfort with their work may be a reason for doctors to delay retirement. 16
In the current survey, the average retirement age of the group of specialists was 65.3 years. This is higher than the Australian Bureau of Statistics’ reported average ages at retirement of Australian professionals (60.1 years), Australian healthcare workers (58.6 years), and those in professional, scientific and technical services (61.0 years). 17 A survey of 3695 medical graduates in the UK reported an average AOR of 60 years, with hospital doctors, including anaesthetists, tending to retire earlier than general practitioners or psychiatrists. Female doctors tended to retire earlier than male doctors; however, the survey was limited by the respondents being aged in their early sixties, with many yet to retire. 5 Orkin et al. reported an average AOR of 62.7 years in 3222 anaesthesiologists surveyed in 2006 in the US. 6 In this population, aged 50–79 years, poor health was cited as a reason for retirement in 60% of respondents who retired aged earlier rather than later. It is important to note that retirement planning among specialist doctors in different countries will be influenced by their unique social, cultural and economic structures. 18 For example, in the UK the personal taxation and pension systems tend to discourage specialist doctors from working past the state pension age of 66 years. 18 , 19 Conversely, the New Zealand pension ‘New Zealand Super’ is not means tested and is available for all those over 65 years of age. 20
The mean AOR of our respondents shows that most retired in their 60s and in good health, which bodes well for them in terms of their healthy life expectancy (HLE). HLE is the expected number of remaining years of life spent in good health from a particular age—in the context of retirement, typically the age of 65 years. 21 Data from the Office for National Statistics (UK) in 2012 indicated that retirees from more affluent areas could expect an average of 12 years of disability-free life after retiring at the age of 65 years. 22 However, for the UK population overall, the HLE from birth was less than 65 years, and in some underprivileged areas the HLE from birth was under 60 years. 22
The majority of our respondents retired when intended, and many were aware of age-related changes. There is no dispute that anaesthetists’ faculties, along with those of other human beings, are affected by age. 9 , 10 , 23 However, the effects of the ageing process on one’s faculties and performance as an anaesthetist is, of course, variable, 24 and many may be practising safely at the age of 65 years or over. It has been suggested that some older doctors possess ‘crystallised intelligence’, and therefore may cope better than younger anaesthetists in maintaining a work–life balance. 25,26 Older doctors have also been shown to exhibit lower levels of psychological distress and burnout, which one paper attributed to ‘the development of protective defences in their relationship with patients, and the liberation afforded by accumulation of experience and changed work conditions’. 16 Peisah et al. studied older doctors ‘identified as ageing well by their peers’. Their findings suggested that those clinicians had insight into the issues of ageing, 27 and had adopted changes in their practice to compensate. Such changes included taking longer speaking with patients, avoiding isolation, avoiding areas of unfamiliar practice, not undertaking new procedural work, and using memory aids. 27 Seeking a second opinion is also a strategy that may be of use to the older practitioner. 28
Increasing age carries an increased risk of being involved in litigation; 4 some respondents showed by their comments that they were well aware of the increased risk of error and potential litigation as they aged. Anaesthesiologists older than 65 years in Ontario, Quebec and British Columbia had 50% more cases involving litigation, and almost twice the number of cases involving severe patient injury, compared with anaesthesiologists younger than 51 years of age. 4 , 29 Similar findings were observed in the UK. 30 Of the 41 doctors aged over 60 years who were referred to the New South Wales Medical Board Impaired Registrants Program between 2000 and 2006, 22% had depression, 29% suffered from substance use, 54% had cognitive impairment and 12% had dementia. 23 Notifications to the Australian Health Practitioner Regulation Agency between 2011 and 2014 showed that older doctors had higher notification rates compared with younger doctors. 31
Until recently, doctors with impairment in Australia tended to be identified reactively, after complaints were made. The professional performance framework, proposed by the Medical Board of Australia in 2018, aims to identify at-risk practitioners proactively, in part by three-yearly health checks and peer review from the age of 70 years. 32 In New Zealand, all medical practitioners are required to undertake recertification, which may consist of CPD programmes facilitated by medical colleges, and includes regular practice review. 33 The Royal Australasian College of Surgeons’ Senior Surgeons Group, recognising the potential effects of ageing, instituted CPD changes for older surgeons, including requirements for health checks and performance review, as well as a modification of CPD requirements for those teaching or doing locum work. 34
There is currently no mandatory retirement age for doctors in Australia. Professor AB Baker’s recommendations for anaesthetists (including reducing night call duties at 55 years of age, ceasing night calls and reducing overall hours at 60 years of age, and retirement at 65 years of age) remain recommendations only. 35 There is ongoing debate as to whether mandatory ages for ceasing call or retiring from active practice can be supported. 4 Peisah et al. suggested that those older doctors with insight, who self-monitor, and who take heed of their colleagues’ experiences and advice, will retire at an appropriate time. 27 They also concluded that doctors without insight into their diminishing capabilities are the most resistant to admitting failings, or to changing behaviour, including the need to retire. 27 Should there be a mandatory retirement age for doctors, such as is considered necessary for airline pilots? The authors suggest that such a ruling would disadvantage many, but catch only a few in the ‘deteriorating competence’ net. But waiting until your surgeons retire, or until someone taps you on the shoulder, may not be the best determinant of when to stop work! 36
The need for resources with information and advice around retirement was recognised over two decades ago by the ANZCA Welfare of Anaesthetists’ Special Interest Group (SIG)—now the Wellbeing SIG. At this time, the SIG generated and published the resource document ‘Retirement and late career options for the older professional’. 37 Information and educational resources surrounding the important individual decision of when to retire, including career advice, need further development. 23 , 28 , 30 The authors suggest that education on all the transitions of a doctor’s life, including qualifying as a doctor, starting specialist practice, as well as strategies for approaching retirement, should be included in all medical school, prevocational and specialist colleges’ curricula. The findings of this survey will help to inform further development of the relevant educational resources, and may encourage other researchers to examine in greater detail some questions raised in this article.
What exactly comprises a successful transition to retirement is likely to vary between individuals and will be influenced strongly by personal decisions. Elements of a successful transition to retirement will require insight and planning. The great majority of respondents in this survey appear to have managed the transition successfully. They reported enjoyment from spending time with their families, having hobbies, as well as keeping in touch with friends and colleagues. Many enjoyed travelling, and a wide variety of other activities. While most had prepared a will, many were yet to arrange enduring powers of attorney and communicate their end-of-life options and organ donation wishes to their families. Our respondents offered many excellent pieces of advice to those of their colleagues contemplating retirement—especially to get one’s finances in order, keep healthy, quit while you are ahead, and smell the roses.
There are limitations to our survey. Our target population was ‘specialists registered with ANZCA as retired’. However, we asked respondents for their age at ‘complete retirement from clinical practice’ which differs from both the Australian Bureau of Statistics 1 and the ANZCA 2 definitions of retirement. This limits accurate comparisons between our data and national data from Australia and other countries. Although our response rate of 60% is considered successful in terms of survey data, 40% of retired anaesthetists are not represented by this survey. We have not compared the demographics of our group with the demographics of the remaining 40% due to the de-identified nature of the survey. Our sample may therefore be biased in terms of age, sex, country of residence and ability to recall events accurately. As our survey relied on email distribution via ANZCA, our results will exclude any anaesthetists not using email, not currently registered with ANZCA as retired or those too unwell to respond.
While it was reassuring to find that most respondents retired when intended and while in their mid-sixties, we recommend improved education and resources be made available to anaesthetists approaching retirement age. The decision to retire will always be heavily influenced by individual circumstances, some of which are beyond our personal control. However, the authors suggest that support for winding down should be facilitated by both public departments and private practice groups. A planned transition to retirement may minimise the likelihood of being ‘tapped on the shoulder’ and maximise the chances of many years of healthy post-retirement life.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X211005783 - Supplemental material for ‘Quit while you are ahead – and smell the roses!’ A survey of retired Fellows of the Australian and New Zealand College of Anaesthetists
Supplemental material, sj-pdf-1-aic-10.1177_0310057X211005783 for ‘Quit while you are ahead – and smell the roses!’ A survey of retired Fellows of the Australian and New Zealand College of Anaesthetists by Diana Strange Khursandi in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
The authors would like to thank the ANZCA Clinical Trials Network for their assistance in distribution of the survey. They would also like to thank Mr Matthew Griffin (ANZCA Professional Affairs) for his assistance in collating the data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by private and departmental resources only.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.