
Abstract

Background
Haemodynamic support using vasopressors is a common intervention provided to patients in the intensive care unit (ICU). Traditionally, they have been administered by way of a central venous line (CVC) to ensure prompt delivery and avoid potential complications that may occur with extravasation from a peripheral site. 1 However, despite the routine use of ultrasound for safety, complications still occur with the insertion and use of these lines. Given these factors, peripheral administration of vasopressors may be a useful alternative.
In Australia and New Zealand, metaraminol is frequently used as a peripheral vasopressor, but noradrenaline can also be administered in a dilute solution peripherally.2,3 We conducted a prospective observational study aiming to compare the safety and cost of peripheral noradrenaline infusion compared with metaraminol infusion for patients requiring low dose vasopressor support in our tertiary 30 bed intensive care department.
Methods
Patients who were admitted without a central venous line who were requiring low dose (less than 5 mg/hour metaraminol) vasopressor support between October 2017 and October 2018 were eligible to participate.
Vasopressor infusions were administered by way of a dedicated peripheral intravenous cannula (ideally 18 G or larger). Patients had continuous monitoring with electrocardiography, oxygen saturation and in most situations arterial blood pressure (or hourly non-invasive measures). Patients were observed for potential complications, including extravasation, loss of cannula, arrhythmias and hypertension.
Metaraminol infusions were administered according to the departmental protocol, using a titrated infusion of 0.5 mg/ml (50 mg in 100 ml). Following the inclusion of 50 patients having received metaraminol, the subsequent 50 consecutive patients received dilute noradrenaline (8 μg/ml (4 mg in 500 ml of 5% dextrose or 0.9% saline)). Baseline demographics, illness severity and indication for vasopressor were collected, in addition to the amount (and calculated cost) of vasopressor vials, intravenous lines and fluid bags used. It takes five vials to make a 100 ml bag of metaraminol at a cost of A$71.09 compared to A$14.02 for a 500 ml bag of dilute noradrenaline. Statistical analysis was conducted using Stata 15.0 (StataCorp LLC, College Station, TX, USA). As both interventions are already accepted forms of treatment for blood pressure support, the study was approved as a quality improvement study (approval number 14208), with a waiver from the ethics committee.
Results
Table 1 outlines the demographics, safety characteristics and cost comparison of the two groups, with no significant differences in age, indication and duration of vasopressors, or fluid administration prior to admission to the ICU. More patients in the noradrenaline group received a CVC and became bradycardic (heart rate <60/minute) during the course of vasopressor treatment; however, this did not reach statistical significance. There were two patients in the noradrenaline group with suspected extravasation, and both were monitored but did not require further management.
Safety and cost summary data for both groups.
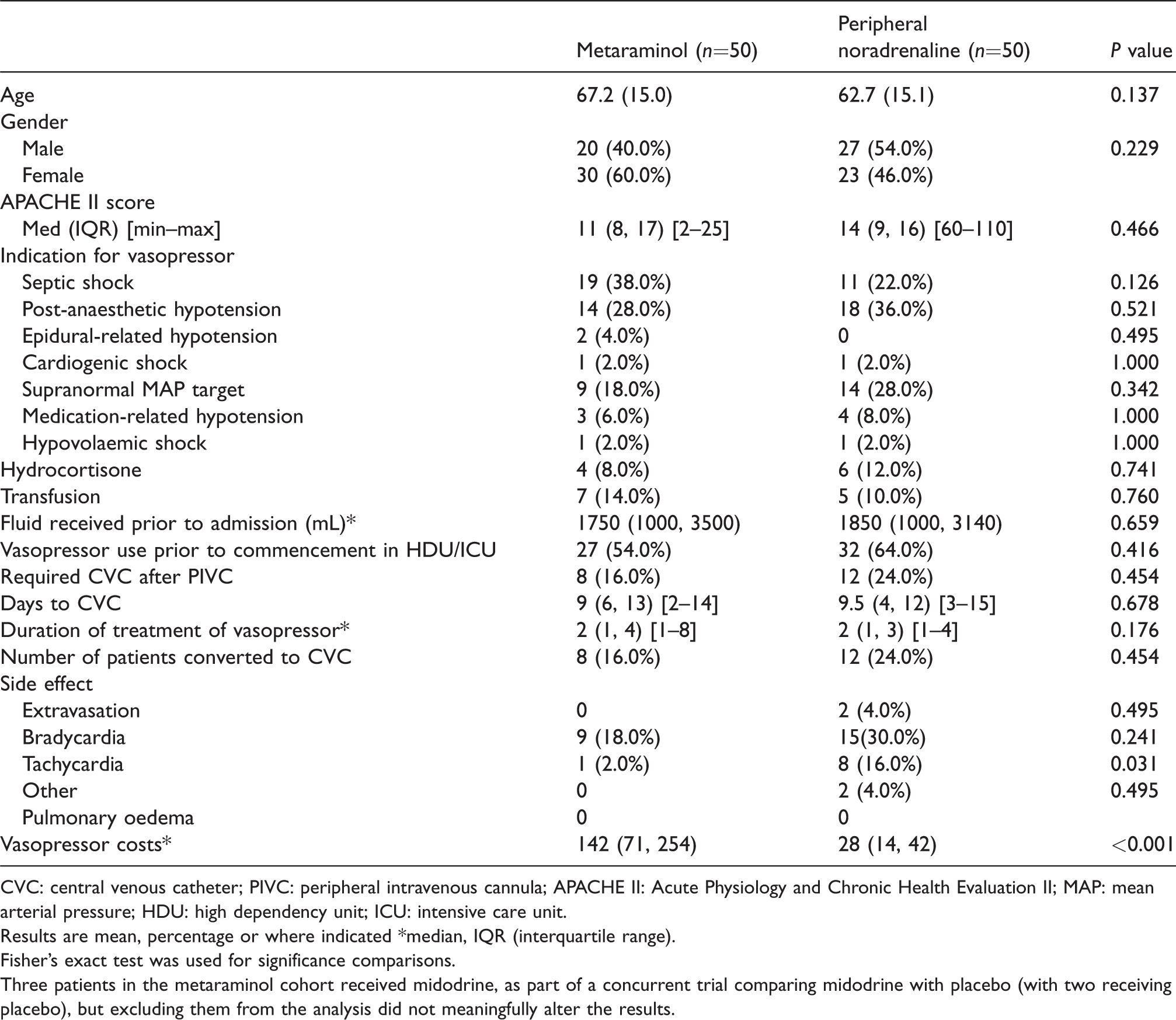
CVC: central venous catheter; PIVC: peripheral intravenous cannula; APACHE II: Acute Physiology and Chronic Health Evaluation II; MAP: mean arterial pressure; HDU: high dependency unit; ICU: intensive care unit.
Results are mean, percentage or where indicated *median, IQR (interquartile range).
Fisher’s exact test was used for significance comparisons.
Three patients in the metaraminol cohort received midodrine, as part of a concurrent trial comparing midodrine with placebo (with two receiving placebo), but excluding them from the analysis did not meaningfully alter the results.
The metaraminol group median cost of treatment per day (cost/days on vasopressor infusion) was A$114 higher than the noradrenaline group. The total cost for the metaraminol group was A$8815.69, while the noradrenaline group total cost was A$1514.48.
Discussion
In this prospective observational study, dilute noradrenaline administered by a peripheral intravenous cannula in an ICU appeared safe, while also being significantly cheaper than metaraminol.
In line with other authors, our study demonstrates that the peripheral intravenous administration of vasopressors carries a low rate of complications and offers a substitute to administration through a central venous line.2,4–6 To support the safe administration we instituted the following measures: development of a guideline in conjunction with pharmacy, education of staff, nursing staff ratios allowing careful titration of doses and observation for complications, and strict use of an appropriately running peripheral cannula. We also had a limit at which clinicians were encouraged to switch to the central administration of vasopressors, (metaraminol rate >5 mg/hour, or 600 μg/hour of noradrenaline).
These findings have two potential benefits for critically ill patients. In limited resource settings, or when the duration of vasopressor requirement may be short, peripheral noradrenaline appears to be a useful option, and is also a cost-saving alternative to metaraminol.
The observational nature of this study introduces several limitations, and we did not account for fluid administration control after arrival in the ICU.
Conclusion
Given the choice between metaraminol and dilute noradrenaline, dilute noradrenaline is cheaper and may be equally safe and efficacious.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.