
Abstract

Insertion of central venous catheters (CVCs) via the Seldinger technique is a routine procedure that is frequently performed in the intensive care unit (ICU) with few complications. Guidewire ensnarement is a serious complication, however, that can occur during ‘blind’ insertion in patients with inferior vena cava (IVC) filters. 1 In this letter, we report a case of guidewire ensnarement during placement of a peripherally inserted central catheter (PICC) in order to raise awareness of this rare but avoidable complication and to discuss strategies for prevention. Written consent was obtained from the patient for publication of this report.
A 48-year-old man was admitted to the ICU with subdural haemorrhage after receiving subcutaneous enoxaparin for lower limb deep vein thrombosis. Anticoagulation was stopped, and a retrievable Celect™ Platinum IVC filter (Cook Medical, Bloomington, IN, USA) was deployed infrarenally by an interventional radiologist. Eight days later, bedside PICC insertion with the Xcela® 5Fr 55 cm PICC kit (Navilyst Medical, Marlborough, MA, USA) was performed in the ICU.
An 0.018-inch 145 cm hydrophilic floppy straight-tip guidewire was introduced into the right basilic vein under real-time ultrasound. The first attempt at guidewire cannulation was unsuccessful and resulted in mild curved deformation (<30°) of the guidewire tip. The same guidewire was successfully introduced on the second attempt with no resistance followed by catheterisation with an over-the-wire technique. Attempts at guidewire withdrawal, however, were met with stiff resistance midway, and the procedure was aborted. The operator was still able to retrieve the guidewire in its entirety by withdrawing the PICC and guidewire en bloc, although the guidewire tip became unravelled in the process. A chest radiograph subsequently showed that the IVC filter had migrated into the right brachiocephalic vein and that one of the struts had become deformed (Figure 1). Interventional radiologists and vascular surgeons were consulted, and the IVC filter was successfully retrieved via an endovascular approach.
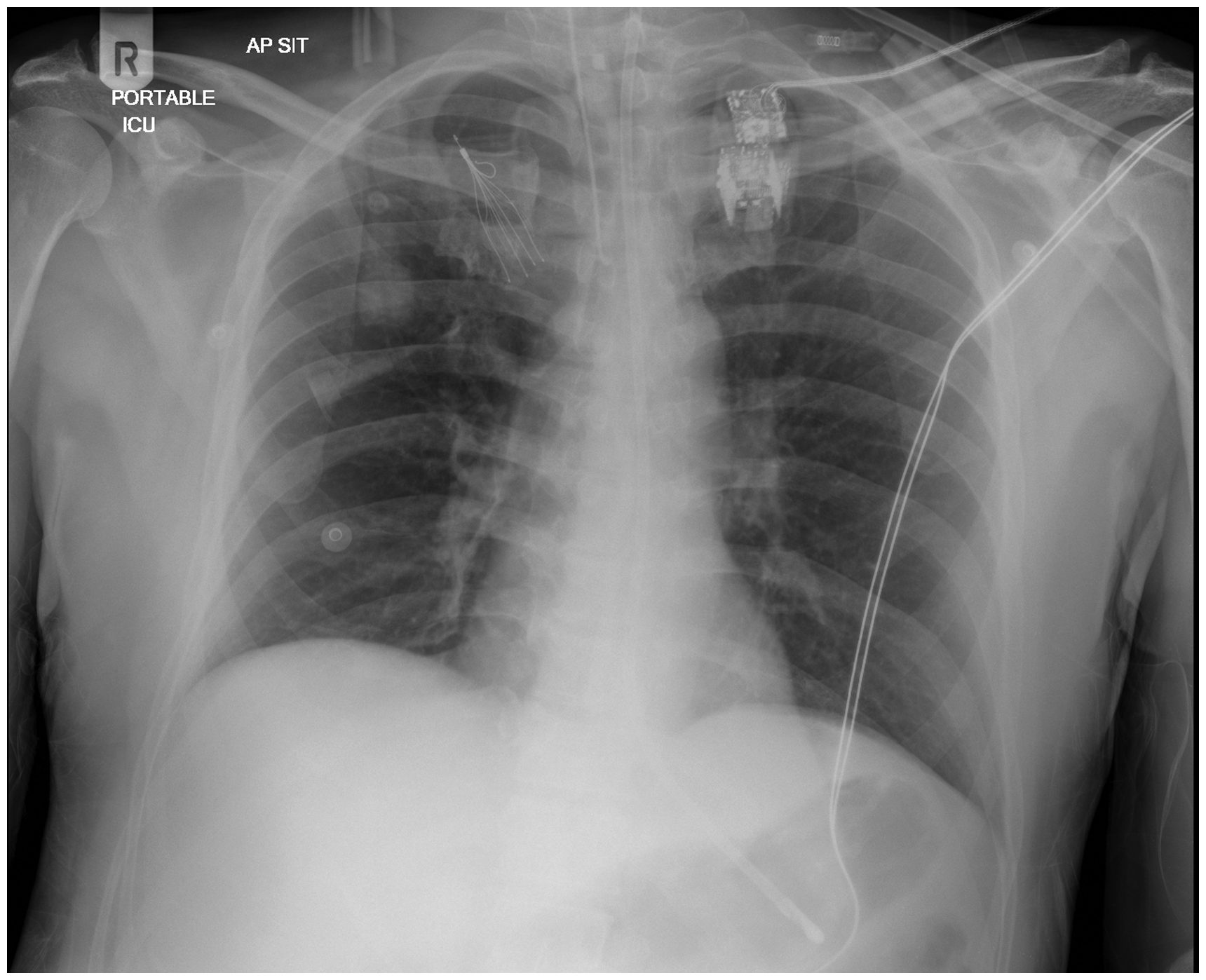
Chest radiograph demonstrating migration of the inferior vena cava filter over the right upper zone of the chest, likely within the brachiocephalic vein. One of the filter struts is deformed and bent backwards. Endotracheal and nasogastric tubes are also present.
Use of IVC filters is increasing. So, proceduralists should routinely review their patients’ medical history for the presence of intravascular devices prior to CVC insertion.
Although bedside placement of a PICC without fluoroscopy can be routinely performed with success rates exceeding 90%, 2 it is advisable that the procedure be performed under fluoroscopy in patients with an IVC filter. Should fluoroscopy be unavailable, operators are advised to utilise only the minimum length of guidewire necessary. Most guidewires are often longer than needed for optimal placement, and operators should pay close attention to the length markings on the guidewire. In general, the guidewire should not be advanced beyond 25 cm using the right jugular or femoral approach. Additionally, pre-procedure plain radiography can be performed to estimate the distance from needle entry site to the IVC filter. 3 All reported cases of guidewire ensnarement thus far have been associated with a J-tipped guidewire, and the use of a straight-tipped guidewire may further reduce the risk of filter entanglement. 4 Should there be guidewire deformation during cannulation, as in our case, a new guidewire should be obtained. Finally, operators should refrain from manipulating guidewires or catheters against resistance. Instead, it should be left in place until urgent imaging is obtained. Forceful attempts to withdraw a trapped guidewire without imaging or careful planning can result in filter dislodgement, migration, caval injury, strut fracture or fragment embolisation which may render filter retrieval more difficult. 1 Although guidewire disengagement via an endovascular approach is generally successful (>95%), 4 specialist vascular surgery assessment is recommended when planning a retrieval procedure particularly if the filter is deformed or fractured.
In summary, iatrogenic IVC filter migration associated with guidewire ensnarement is a rare but serious complication that can be avoided at multiple levels. Routine review of patients’ medical history, use of fluoroscopy or bedside plain radiography, careful guidewire usage and prompt identification of guidewire ensnarement can greatly reduce the risk of filter migration and deformation.
Footnotes
Declaration of conflicting interests
The author(s) have no potential conflicts of interest to declare with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.