
Abstract
Self-harm is one of the most common reasons for admission to an intensive care unit (ICU). While most patients with self-harm survive the ICU admission, little is known about their outcomes after hospital discharge. We conducted a retrospective cohort study of patients in the Barwon region in Victoria admitted to the ICU with self-harm (between 1998 and 2018) who survived to hospital discharge. The primary objective was to determine mortality after hospital discharge, and secondarily estimate relative survival, years of potential life lost, cause of death and factors associated with death. Over the 20-year study period, there were 710 patients in the cohort. The median patient age was 37 years (interquartile range (IQR) 26–48 years). A total of 406 (57%) were female, and 527 (74%) had a prior psychiatric diagnosis. The incidence of ICU admission increased over time (incidence rate ratio 1.05; 95% confidence interval (CI) 1.03–1.06 per annum). There were 105 (15%) patients who died after hospital discharge. Relative survival decreased each year after discharge, with the greatest decrement during the first 12 months. At ten years, relative survival was 0.85 (95% CI 0.81–0.88). The median years of potential life lost was 35 (IQR 22–45). Cause of death was self-harm in 27%, possible self-harm in 32% and medical disease in 41%. The only factors associated with mortality were male sex, older age and re-admission to ICU with self-harm. Further population studies are required to confirm these findings, and to understand what interventions may improve long-term survival in this relatively young group of critically ill patients.
Introduction
Intentional self-harm accounts for more than 20,000 hospital admissions in Australia each year. 1 It is the leading cause of death in people aged 15–44 years, and is responsible for the greatest years of life lost. 2 Self-harm is one of the most common reasons for admission to an intensive care unit (ICU)3–5 yet receives substantially less research attention than other critical illnesses. 6
While in-hospital mortality rates of ICU patients with self-harm are lower than those with other critical illnesses, relatively little is known about their outcomes after hospital discharge.6–9 An episode of self-harm is a strong predictor of subsequent suicide,10–13 and the need for an ICU admission may identify a group of patients with higher intent of dying.14–16 Hence, those who survive an ICU admission with self-harm may be at particularly high risk of dying after they leave hospital.
For these reasons, we undertook a study to investigate long-term outcomes of patients admitted to the ICU with intentional self-harm who survived to hospital discharge. The primary objective was to determine the mortality of this patient cohort relative to the background population. Additionally, we sought to quantify the incidence of ICU admission with self-harm, describe the principal causes of death after hospital discharge, estimate the years of potential life lost, and determine factors associated with mortality.
Methods
Study design
This was a retrospective observational cohort study of patients with intentional self-harm admitted to the ICU at Barwon Health between 1 July 1998 and 30 June 2018 (20 years). The research and ethics committee of Barwon Health approved this study (project no.: 18/173).
Study setting
Barwon Health is based in Victoria, Australia, and serves a regional population of approximately 400,000 people. It comprises a general hospital of 370 inpatient beds, with a 17-bed ICU. The Mental Health, Drugs and Alcohol Service (MHDAS) provides multidisciplinary community and inpatient services, comprising an inpatient psychiatric unit, consultation/liaison (CL) service, child and adolescent mental-health service, drug and alcohol service, acute intervention service, community rehabilitation programmes, and a community mental health team (CMHT).
Cohort definitions
Hospital admission with intentional self-harm was identified using codes from the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM). Case inclusion criteria included admission to the ICU with intentional self-harm by poisoning (ICD-10-AM Codes X60–X69) or trauma (ICD-10-AM Codes X70–X84), with survival to hospital discharge.
Data sources
ICU data were obtained from an in-house database, and hospital data from medical records. Linkage of the ICU database with the Australian National Death Index captured date of death after hospital discharge, along with principal cause of death coded to ICD-10-AM. 17 MHDAS data were sourced from the client management interface/operational data store (Department of Health and Human Services, Victoria), community care documentation system (The Care Manager) and hospital medical records. Linkage between datasets used patient surname, given names, sex, date of birth and hospital record number. An anonymous record identification number was created, and patient identifiers were removed from the analysis dataset.
Data collected
Descriptors of the cohort included patient demographics (age, sex, residential area), socioeconomic indices (the Index of Relative Socio-economic Disadvantage and the Index of Relative Socio-economic Advantage and Disadvantage), 18 year of admission, ICD-10-AM code, any previous episode with the MHDAS and any prior psychiatric diagnoses identified from the MHDAS datasets.
Descriptors of the ICU admission included source of admission (emergency department, ward, operating theatre, other hospital), cardiac arrest in the 24 hours prior to admission, Glasgow Coma Scale (GCS) score, severity of illness scores (Acute Physiology And Chronic Health Evaluation (APACHE)), mechanical ventilation, cardiovascular support, renal replacement therapy, extracorporeal life support and length of stay (ICU, hospital).
MHDAS management was described by the duration between ICU admission and CL psychiatry review, compulsory admission status at any time in ICU (Victorian Mental Health Acts 1986 and 2014), hospital discharge destination (home, inpatient psychiatric unit) and follow-up with a CMHT.
Outcomes
The primary outcome was mortality rate after hospital discharge relative to the age- and sex-matched population of Victoria. Secondary outcomes included principal causes of death, years of potential life lost and patient characteristics associated with mortality after hospital discharge.
Statistical methods
Data are presented as absolute numbers (%), and summarised as mean (standard deviation (SD)) or median (interquartile range (IQR)) where appropriate. The number of ICU admissions with self-harm codes and their proportion of all ICU admissions (with 95% confidence intervals (CI)) were determined, and temporal trends were derived by Poisson regression with robust standard errors.
Relative survival was referenced to age- and sex-specific life tables for the state of Victoria. 19 Estimates employing the Ederer II estimator, with 95% CI, were calculated annually for ten years following the index hospital episode. Excess mortality over time, as the rate per 1000 patient years, was estimated via a Poisson generalised linear model, employing restricted cubic splines to account for temporal non-linearity. Estimates of years of potential life lost were censored at 78 years of age. 20 Factors independently associated with all-cause mortality censored at ten years after discharge were assessed by Cox proportional hazards regression. Exploratory analyses included outcomes and risk factors for ICU re-admissions with self-harm. All analyses were performed in Stata/MP v15.1 (StataCorp LP, College Station, TX, USA).
Results
Incidence of ICU admission
Over the 20-year study period, there were 24,632 ICU patient episodes, of which 880 (3.6%) had a self-harm code. The number and proportion of ICU episodes with self-harm increased from 28 (3.1%) of 907 ICU admissions in 1998–1999, to 75 (5.5%) of 1376 ICU admissions in 2017–2018, with an average incidence rate ratio of 1.05 (95% CI 1.03–1.06) per annum (Figure 1).
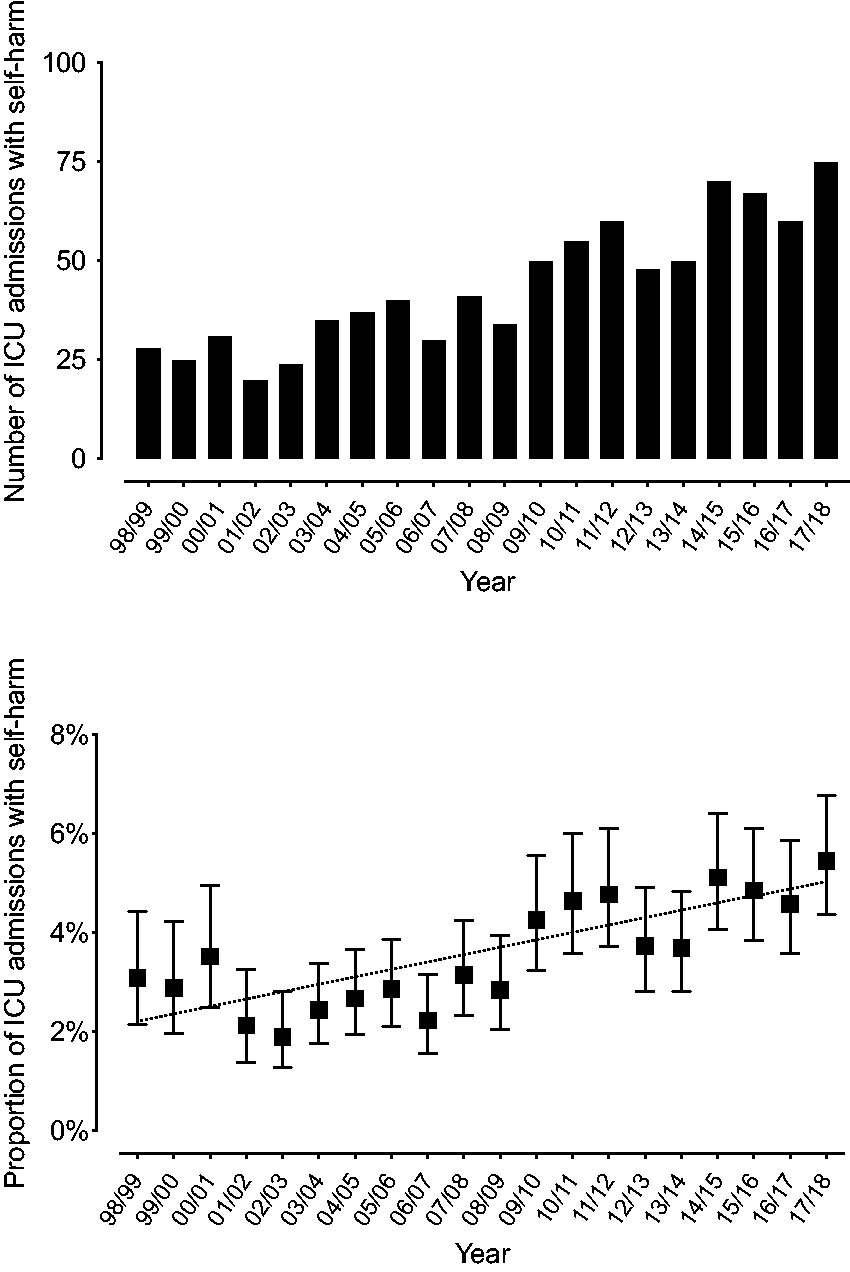
Incidence of intensive care unit (ICU) admission with self-harm at Barwon Health. (a) Number of ICU admissions with a self-harm code (ICD-10-AM X60-X84), and (b) proportion of ICU admissions (with 95% confidence intervals) that had a self-harm code. Dotted line represents regression over time.
Cohort characteristics
There were 750 patients with an index ICU admission with self-harm, of whom 40 (5.3%) died in hospital (Supplemental Tables S1 and S2). The 710 patients surviving to hospital discharge formed the study cohort (Supplemental Figure S1), whose characteristics are outlined in Table 1.
Characteristics of patients admitted to the intensive care unit with self-harm who survived to hospital discharge.
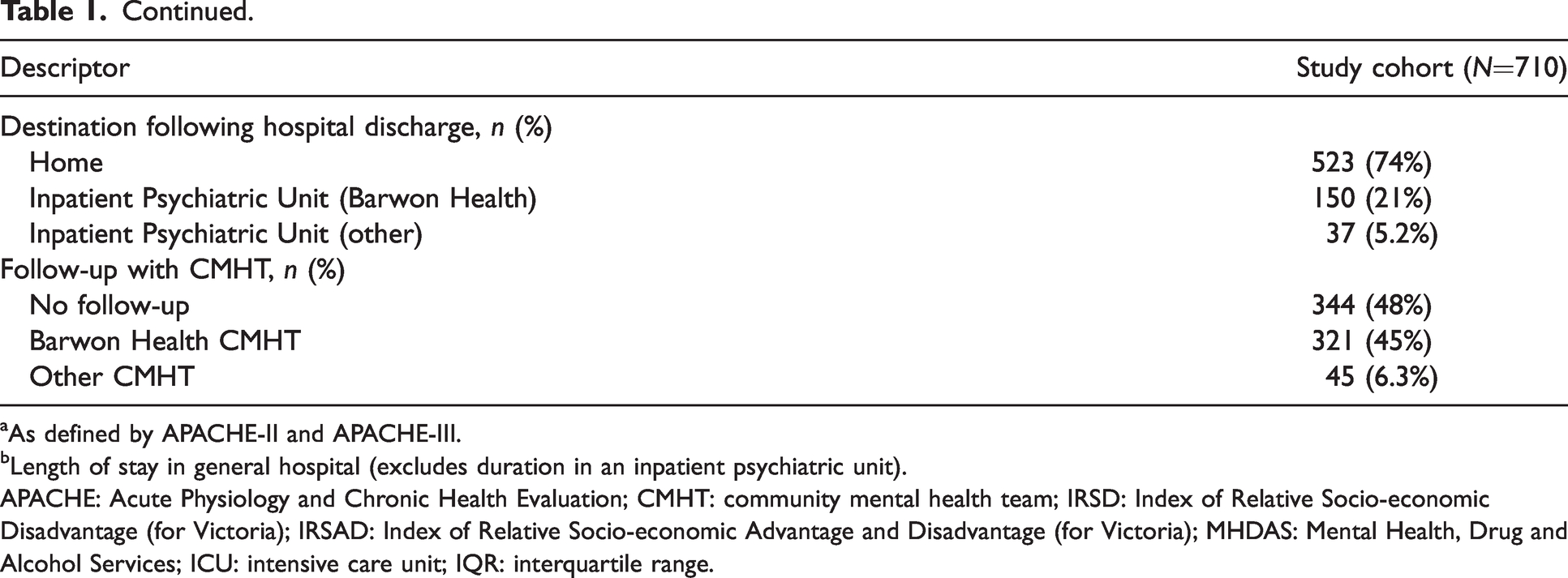
aAs defined by APACHE-II and APACHE-III.
bLength of stay in general hospital (excludes duration in an inpatient psychiatric unit).
APACHE: Acute Physiology and Chronic Health Evaluation; CMHT: community mental health team; IRSD: Index of Relative Socio-economic Disadvantage (for Victoria); IRSAD: Index of Relative Socio-economic Advantage and Disadvantage (for Victoria); MHDAS: Mental Health, Drug and Alcohol Services; ICU: intensive care unit; IQR: interquartile range.
The median patient age was 37 years (IQR 26–48 years), and 406 (57%) were female. Five hundred and twenty-seven (74%) had a prior psychiatric diagnosis, with major depressive disorder, substance-use disorder and borderline personality disorder the most common. Three hundred and sixty-six (52%) patients had previous contact with the MHDAS, with 126 (18%) having contact within the three months prior to ICU admission.
Self-harm was coded as poisoning in 648 (91%) patients, trauma in 29 (4.7%) and a combination of both in 29 (4.1%) patients. Self-poisoning with anti-epileptic, sedative/hypnotic or psychotropic drugs was coded in 549 (77%) index admissions (Supplemental Table S2).
ICU supportive treatments included mechanical ventilation for 437 (62%) patients, cardiovascular support for 111 (16%), dialysis for 19 (2.7%) and extra-corporeal life support in one patient. The median length of stay was 1.3 days (IQR 0.7–2.2 days) in the ICU and 2.6 days (IQR 1.5–4.8 days) in hospital.
Six hundred and seventy-seven (95%) patients received a mental health assessment during hospitalisation. Fifty (7.0%) patients were subject to a compulsory treatment order under the relevant Mental Health Act, and 187 (26%) patients were admitted to an inpatient psychiatric unit. Three hundred and sixty-six (52%) patients received CMHT follow-up after hospital discharge.
Mortality
A total of 105 (15%) patients died after hospital discharge, within a median follow-up time of 6.6 years (IQR 3–10 years). Relative survival decreased incrementally each year after hospital discharge (Figure 2). After ten years, relative survival was 0.85 (95% CI 0.81–0.88; females 0.86 (95% CI 0.81–0.90), males 0.83 (95% CI 0.77–0.88)). Excess mortality was greatest in the first 12 months after hospital discharge, with 24 patients dying during this time (Figure 2). The median years of potential life lost was 35 (IQR 22–45; Figure 3).
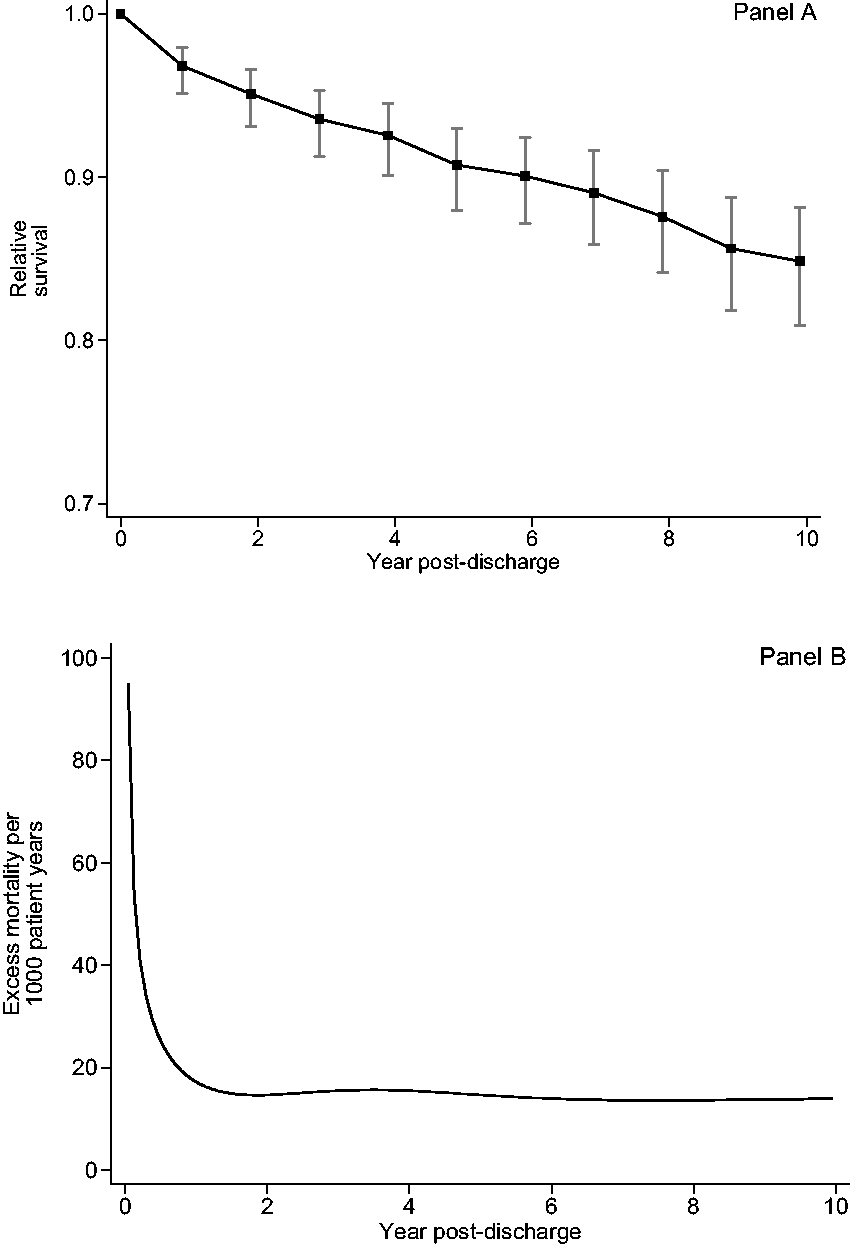
Relative survival of patients admitted to the intensive care unit with self-harm and discharged from hospital. (a) Annual point estimates per year post discharge with 95% confidence intervals, and (b) excess mortality per 1000 patient years modelled over the ten years after hospital discharge using a restricted cubic spline.
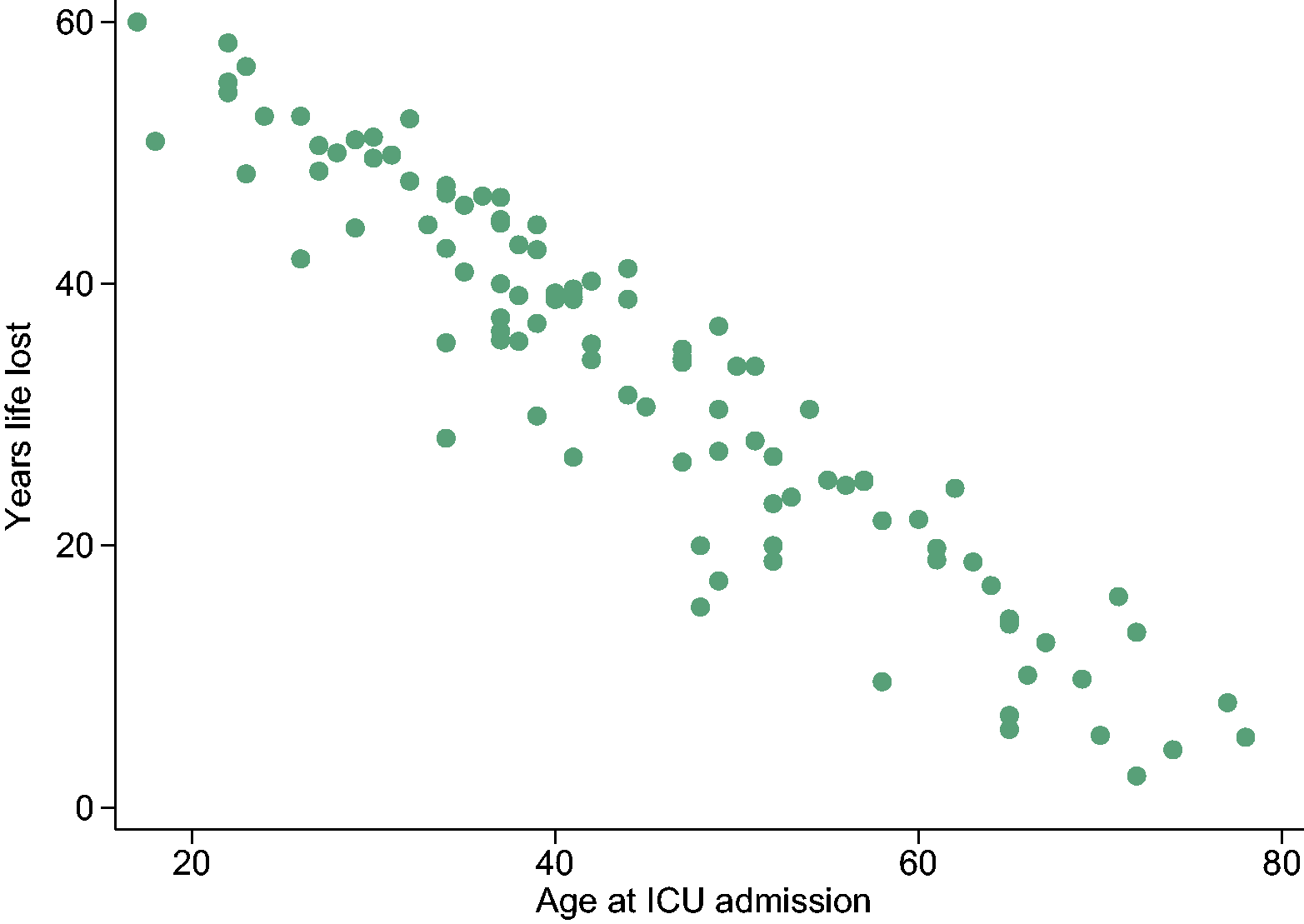
Scatter plot of the potential years of life lost in patients admitted to the intensive care unit (ICU) with self-harm who died after hospital discharge (excludes patients aged >78 years).
Cause of death
A principal cause of death code was known for 100 (95%) of the deceased. Twenty-seven had a code of intentional self-harm, 32 had a code that could possibly represent self-harm and 41 had a code representing medical conditions (Supplemental Table S3).
Of the 24 patients who died within 12 months of hospital discharge, 12 (50%) died from intentional self-harm, five (21%) from possible self-harm and seven (29%) from other medical conditions (Supplemental Table S4).
Factors associated with mortality
Factors of the index ICU admission associated with mortality after hospital discharge were male sex and older age group (Table 2). No other factors associated with mortality were identified.
Features of the index intensive care unit admission associated with mortality after hospital discharge (censored at ten years).
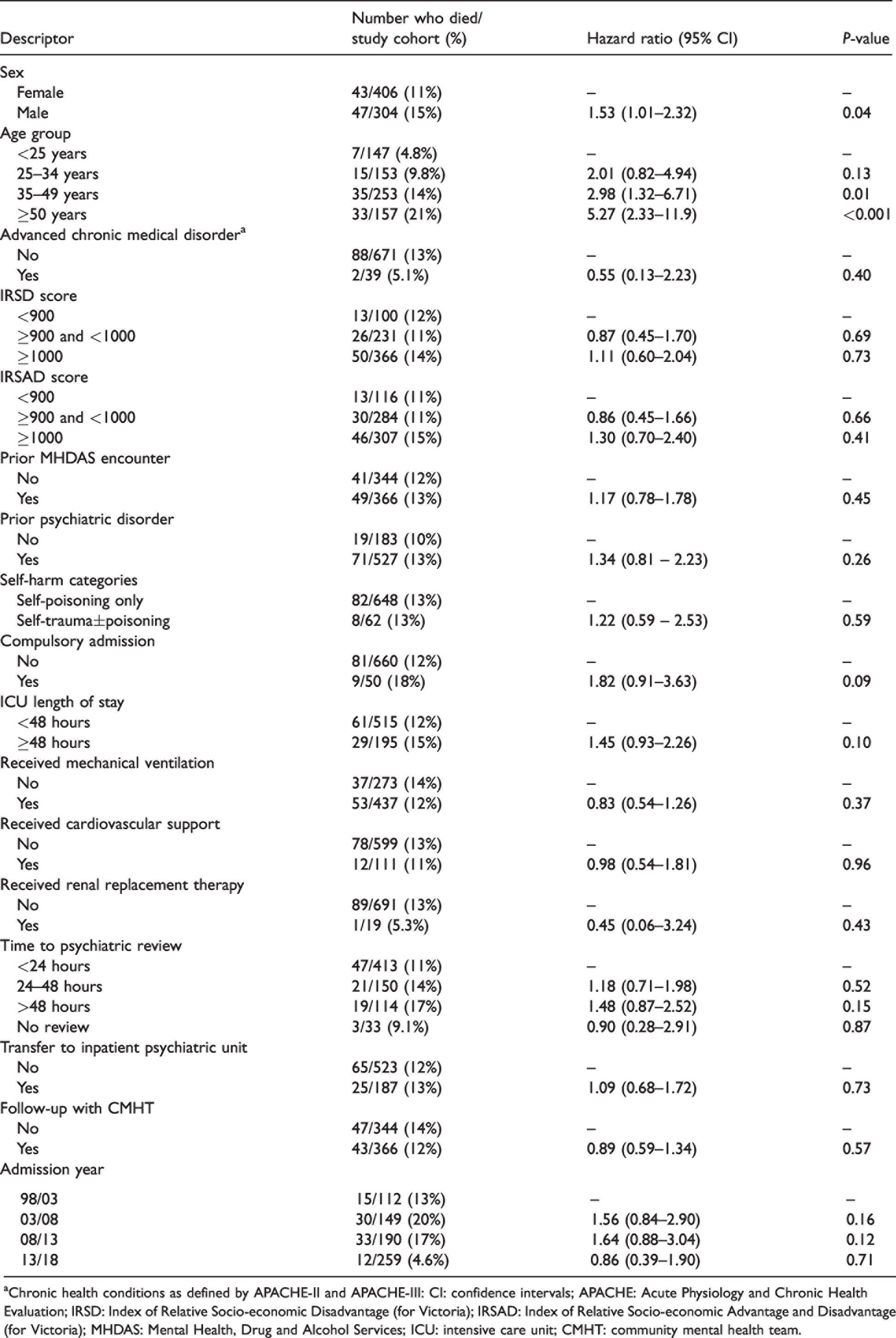
aChronic health conditions as defined by APACHE-II and APACHE-III: CI: confidence intervals; APACHE: Acute Physiology and Chronic Health Evaluation; IRSD: Index of Relative Socio-economic Disadvantage (for Victoria); IRSAD: Index of Relative Socio-economic Advantage and Disadvantage (for Victoria); MHDAS: Mental Health, Drug and Alcohol Services; ICU: intensive care unit; CMHT: community mental health team.
Re-admissions to intensive care with self-harm
Eighty-three (12%) patients had at least one re-admission to the ICU with self-harm (Supplemental Table S5). Mortality was higher in those who had more than one ICU admission with self-harm (14% versus 23%, P=0.027). Characteristics of the index admission associated with a re-admission to ICU included female sex and a prior psychiatric diagnosis (particularly borderline personality disorder, depressive disorders and substance-use disorder; Supplemental Table S6).
Discussion
Our key finding is that patients admitted to the ICU with self-harm have a long-term survival rate that is 15% lower than age and sex population norms. We also observed that excess mortality is greatest in the first 12 months after ICU discharge, and that self-harm was the dominant cause of death during the follow-up period. The importance of these findings is amplified by the large number of years of potential life lost (reflecting lethality in a young patient demographic) and the increasing prevalence of patients admitted to ICU with self-harm over the 20-year study period.
Typical features of this cohort were that they were relatively young, just over half were female, were admitted voluntarily from the emergency department with self-poisoning, have little requirement for ICU support other than mechanical ventilation and have short lengths of stay in ICU and hospital. While one in four patients were admitted for ongoing inpatient psychiatric care, approximately half (48%) did not receive follow-up from the local tertiary mental health service.
Excess mortality was found to be greatest in the first year after discharge from hospital. These ‘early’ deaths from suicide represent almost half (44%) of all patients who subsequently died from self-harm. There was no predominant feature of those who died from suicide within 12 months, and the majority received community mental health team follow-up post hospital discharge. It is also important to recognise that excess mortality in this cohort was not all from suicide, with 40% of deaths from medical disease. Patients with mental illness are known to be at increased risk of comorbid medical conditions, especially within the first 12 months of a psychiatric diagnosis. 21
Older age and male sex were the only factors associated with mortality after hospital discharge. This is consistent with findings of previous studies. 2 , 12 Acknowledging the limitations of our study size, we found no association between mortality and socioeconomic indices, year of admission, severity of critical illness, previous psychiatric illness or encounters with the MHDAS. Repeated self-harm is a well-described risk factor for suicide, 12 , 22 and our supplemental analysis found that mortality was significantly higher in those with a re-admission to the ICU.
Our findings are consistent with, and add to, the limited literature reporting long-term outcomes in patients who survive an ICU admission after self-harm. A Swedish study of 6730 patients with poisoning or substance abuse found that 4.5% had died within a year of hospital discharge, and this mortality rate was nearly 50 times greater than the age-matched population. 23 A Dutch study of 7331 patients admitted with ‘intoxication’ (of unknown intent) reported an ICU mortality of 1%, but after two years, nearly 9% of patients had died. 7 Similarly, a single-centre study from Christchurch, New Zealand, of 302 patients with ‘serious suicide attempts’ reported 9% mortality within five years of hospital discharge, with 60% of the deaths being from suicide. 8 , 16 A single-centre study from Western Australia noted that patients admitted to the ICU with ‘poisoning/drug overdose’ had a risk of death after hospital discharge that was higher than those with sepsis, trauma or cardiac arrest. 24 Subsequently, a study of 102 patients with drug overdose admitted to an ICU in metropolitan Melbourne reported that 10% had died within four years of hospital discharge. 16 Interestingly, they noted that mortality and incidence of hospital re-admission with self-harm was no different to a matched group of patients with a drug overdose managed on the general wards. Although case definitions differed between all these studies, collectively they illustrate a significant and ongoing burden of disease in patients with serious self-harm after they have left hospital.
There are several implications of our study. First, the data support the need to focus on mental health and medical follow-up of patients who have had an episode of serious self-harm, particularly within the 12 months after hospital discharge. Active contact and follow-up interventions for patients after self-harm have been shown to be effective in reducing the risk of repeat suicide attempts. 25 , 26 Our data support the importance of follow-up programmes after serious self-harm. Examples of this include the Hospital Outreach Post-Suicidal Engagement programme 27 and Way Back Program 28 that seek to engage with patients through a structured psychosocial intervention in the months after a suicide attempt. Second, the study demonstrates the need for health services to monitor outcomes of patients after ICU admission, and to ensure appropriate linkages with community and primary services so that care is provided in a holistic way for this at-risk group. Third, the study highlights an increase in the prevalence of self-harm--related presentations to the ICU over a 20-year period, and further work is required to understand why this is occurring.
Limitations of this study include it being from a single region, with uncertain generalisability to other centres. However, the Barwon region has been a reliable epidemiological base for a variety of other population cohort studies. Relative survival and years of potential life lost are useful to describe mortality, but these metrics are currently unavailable for other diseases managed in the ICU, and hence they are difficult to place in context. Details of long-term functional status of patients were not available. Only encounters with the health service MHDAS were available. Encounters with other health services, general practitioners and other medical specialists were not available. We were also unable to determine the extent of engagement with the CMHT for each patient, which may have had some impact on survival outcome. Details about previous psychiatric disorders were derived from notes in the patients’ files, and the severity of these was not quantified. The intent of self-harm (e.g. suicide, relieve anguish, ‘cry for help’) is not differentiated in ICD-10-AM codes, and was not able to be considered as a covariate for long-term outcome. The diagnosis of advanced chronic disease was extracted from APACHE categories, and may have missed other significant medical illness not classified. The cohort size was relatively small to identify characteristics associated with death from self-harm and other causes separately.
Conclusions
Patients admitted to the ICU with self-harm had a higher than expected mortality after hospital discharge, particularly within the first 12 months. The increasing incidence of ICU admission with self-harm and the large number of years of potential life lost are impetus to understand better how to care for these patients after hospital discharge. Further studies are required to understand whether these observations apply across wider health jurisdictions and what services may improve survival.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X20978987 - Supplemental material for Long-term outcomes of patients admitted to an intensive care unit with intentional self-harm
Supplemental material, sj-pdf-1-aic-10.1177_0310057X20978987 for Long-term outcomes of patients admitted to an intensive care unit with intentional self-harm by Matthew J Maiden Roth Trisno Mark E Finnis Catherine M Norrish Steven Moylan in Anaesthesia and Intensive Care
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
ORCID iDs
Supplemental material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.