
Abstract
Although a wide range of medical applications for three-dimensional printing technology have been recognised, little has been described about its utility in critical care medicine. The aim of this review was to identify three-dimensional printing applications related to critical care practice. A scoping review of the literature was conducted via a systematic search of three databases. A priori specified themes included airway management, procedural support, and simulation and medical education. The search identified 1544 articles, of which 65 were included. Ranging across many applications, most were published since 2016 in non – critical care discipline-specific journals. Most studies related to the application of three-dimensional printed models of simulation and reported good fidelity; however, several studies reported that the models poorly represented human tissue characteristics. Randomised controlled trials found some models were equivalent to commercial airway-related skills trainers. Several studies relating to the use of three-dimensional printing model simulations for spinal and neuraxial procedures reported a high degree of realism, including ultrasonography applications three-dimensional printing technologies. This scoping review identified several novel applications for three-dimensional printing in critical care medicine. Three-dimensional printing technologies have been under-utilised in critical care and provide opportunities for future research.
Introduction
Three-dimensional (3D) printing is a technology that builds complex structures through the application of layers of substrate in an additive fashion.1–3 Used in commercial and industrial applications for decades, this technology has become widely available in recent years. An increasing number of medical applications have been recognised, including the production of custom prostheses, devices, and models for teaching and simulation practice.1–3 There is a growing body of literature regarding the use of 3D printing technologies for personalised implants and devices, bioactive scaffolds to promote tissue growth, and the direct printing of tissues and organs. 4
Despite its use in other areas of medicine, the use of 3D printing in critical care has remained limited and poorly explored in the literature. We recently used 3D printing to develop a high-fidelity low-cost manikin for a comprehensive simulation of extracorporeal cardiopulmonary resuscitation. 5 This experience prompted us to search for other applications for 3D printing within the discipline of critical care medicine. The objective of this study was to conduct a scoping review of the literature in order to identify applications of 3D printing relevant to critical care medicine and to identify potential future research opportunities and priorities.
Methods
Study protocol
The study protocol was established a priori and was developed as outlined by the members of the Joanna Briggs Institute and Joanna Briggs Collaborating Centres.
6
The specific research question was, ‘What are the applications of 3D printing in critical care medicine with respect to:
Airway management, procedural support including vascular access, spinal procedures, and tube thoracostomy, simulation and medical education, and other applications relevant to critical care?’
Eligibility criteria
Studies of any methodology that related to one or more of the study research questions were considered. Studies were included if they had clinical applications to critical care. Studies were excluded if they were written in languages other than English, conducted in non-human subjects, or were reviews or editorials that did not contain novel information.
Search methodology
An initial search was performed of three databases, PubMed, EMBASE and Web of Science from inception through to 28 February 2020. The search strategy used a variety of terms to capture articles relating to 3D printing used in critical care settings including intensive care, emergency medicine, anaesthesiology and trauma medicine. Details of the search strategy can be found in Table 1.
Detailed search strategy for scoping review.
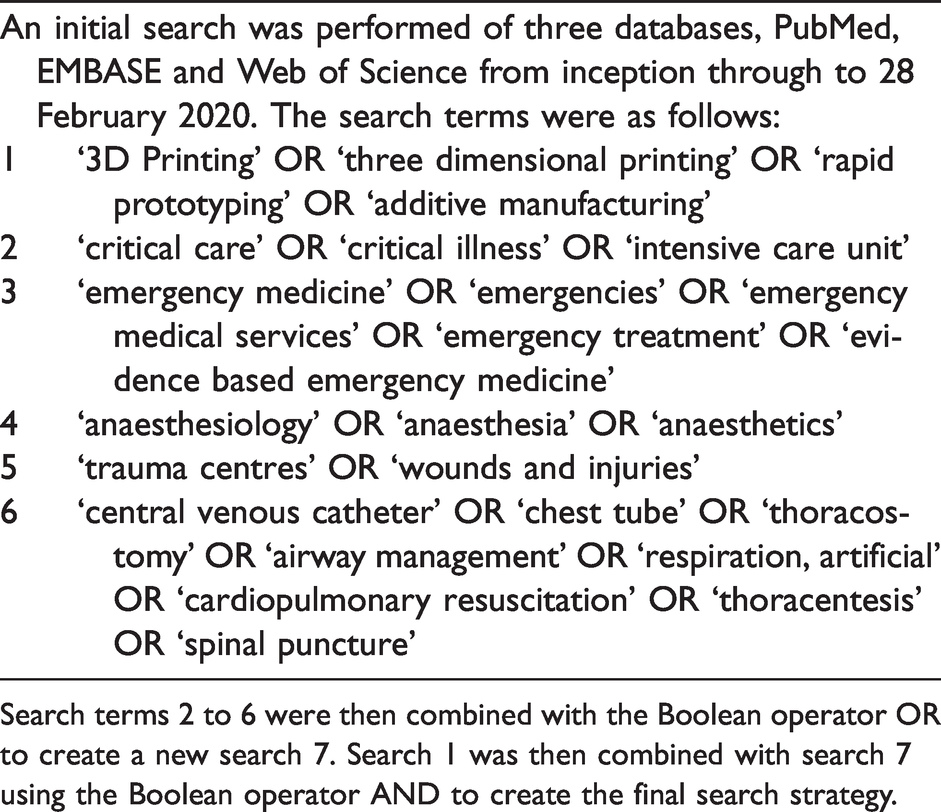
Search terms 2 to 6 were then combined with the Boolean operator OR to create a new search 7. Search 1 was then combined with search 7 using the Boolean operator AND to create the final search strategy.
Titles and abstracts were screened independently by two authors (NA and KBL) for potential inclusion. Full text articles were retrieved and reviewed independently by two authors (NA and KAW) for eligibility criteria. At each stage, discrepancies between the two reviews were resolved by a third author. Reference lists of included articles were reviewed for additional articles. Following the compilation of a list of articles for inclusion, data were extracted by two authors (NA and KAW) with results mapped according to the prespecified themes. Analysis was descriptive.
Results
The search strategy identified 1544 citations, of which 65 were included for inclusion in the final review as detailed in Figure 1. The years of publication ranged from 2010 to 2020, with most papers being published from 2016 onwards. Studies were conducted in 16 countries, most commonly the United States of America (n = 26) and Canada (n = 11), with the remainder from countries in Europe (n = 15), Asia (n = 11), Australia (n=1) and South America (n = 1). Although originally mapped according to the a priori research questions, based on results these were revised to the themes of simulation, procedural support and other applications.
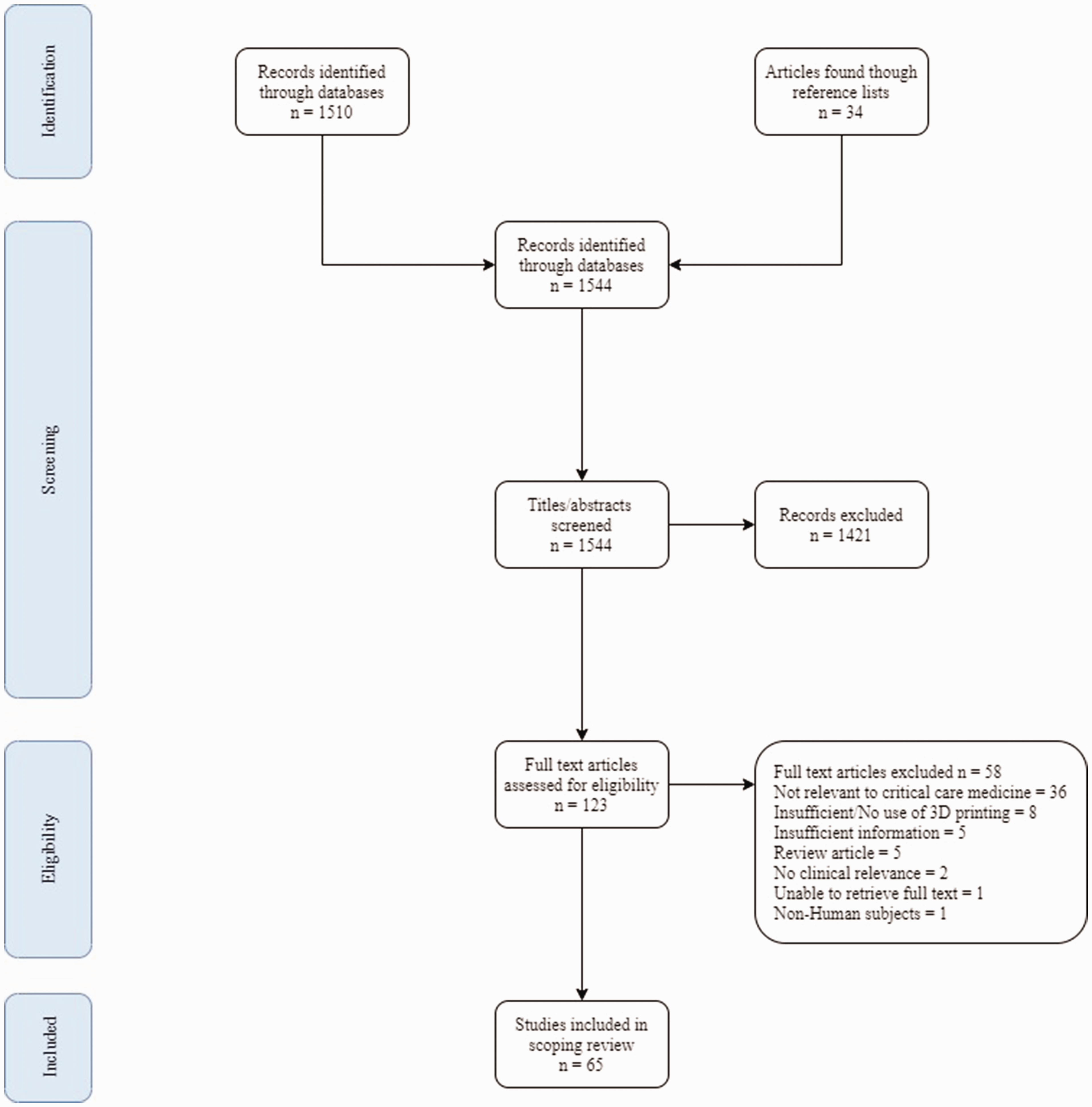
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for study identification and inclusion.
Simulation
Forty-five articles relating to simulation were classified into the sub-themes of front-of-neck access (n=10), preoperative planning for airway management (n = 8), bronchoscopy (n = 7), spinal/neuraxial procedures (n = 8), vascular access (n = 6), thoracostomy (n = 3) and miscellaneous (n = 3).
Ten studies investigated different uses of 3D printing for the simulation of front-of-neck access for airway management.7–16 One randomised controlled trial compared a 3D-printed model to a conventional high-fidelity simulator and found that after training on either device there was no significant difference in success rate or procedure time than when cricothyroidotomy was performed by 52 unskilled residents on a porcine larynx. 7 Gauger and colleagues found that a 3D-printed laryngotracheal model improved anaesthetic residents’ knowledge and performance in cricothyroidotomy in a low-resource setting; however, no comparator was used. 14 Kovatch and colleagues developed a paediatric airway model constructed from silicone using a 3D-printed cast and validated it as an effective training tool for cricothyroidotomy by six anaesthesiologists and otolaryngologists, who noted a high degree of realism. 11 Shen and colleagues created a printed airway intervention simulation model that incorporated electromagnetic sensors and a motion tracking system to allow augmentation with virtual reality to improve fidelity. 16 Six further studies related to this topic, including two abstracts that created high-fidelity low-cost cricothyroidotomy simulation models, 8 , 15 two that simulated obese patients’ airways, 9 , 10 and two that used porcine skin with artificial blood to simulate bleeding in a 3D-printed model. 12 , 13
Eight studies used 3D-printed models for preoperative planning and simulation of airway management in complex cases, five of which were in children.17–24 Kavanagh and colleagues developed four models using 3D printing, including three direct-printed models made with different materials, including polylactic acid (PLA), acrylonitrile butadiene styrene and high-impact polystyrene, and a silicone model made from a 3D-printed cast. 18 These were tested by four otolaryngologists who concluded that the cast model was significantly better in terms of tissue characteristics, ease of tissue manipulation and overall accuracy. 18 Similar findings were also observed in two other studies reporting on the development of paediatric intubation simulation models involving the 3D printing of airways using black resin and red Ninjaflex (NinjaTek, Manheim, PA, USA). 17 , 19 Challenges included that the black colour used in the resin obscured the intubating view and while Ninjaflex was most comparable to soft tissue, it did not demonstrate the same yield as human tissue. 17 , 19 Single patient case studies were reported including complex cases of intubations involving children with Jarcho–Levin syndrome 20 and another with pulmonary alveolar proteinosis requiring single-lung ventilation. 21 Three other studies included printed models to plan and rehearse intubation preoperatively in complex cases related to a laryngectomy, tracheal stenosis and a head and neck cancer.22–24
Seven studies investigated 3D printing of airway models for bronchoscopy.25–31 A single-blinded, randomised, controlled study involving 30 anaesthetists and physicians compared a low-cost, 3D-printed bronchial model of a healthy patient against two commercial training devices. 29 The overall realism of anatomy was significantly higher in the 3D-printed model and was sufficiently similar for the performance of skills, including localising an obstruction, placing a bronchial blocker and the aspiration of fluid. 29 Another study compared two healthy patient 3D-printed models for rigid bronchoscopy which reported a high degree of realism and instrument manoeuvrability, with no significant difference in overall satisfaction when compared to a porcine model. 25 Similarly, Ho and colleagues developed three different patient-specific, multi-material, 3D-printed bronchoscopy models, that respiratory physicians reported as having a high degree of anatomical realism, endoscopic manoeuvrability, representation of pathologies and value for learning. 27
Eight studies involved the use of 3D printing in simulations for spinal and neuraxial procedures.32–39 Jeganathan and colleagues produced a 3D-printed thoracic spine model for the simulation of epidural insertion, which 14 physicians reported as good on a Likert scale for the realism of palpation, needle entry and pop sensation through the ligament, and excellent for ultrasound anatomy and guidance. 32 Another novel lumbar spinal model tested by 22 anaesthetists was found to be comparable to the Simulab procedural trainer in relation to soft tissue resistance to the needle, but the model lacked realistic palpation, was fragile and had needle track marks. 35 These characteristics may have in part been due to model construction using PLA filament with gelatin with psyllium fibre filler. Odom et al. used a nylon-based lumbar model tested by nine healthcare workers who found it both easy to use and realistic during palpation. 36 Five studies specifically considered the role of ultrasonography in spinal procedures, finding that PLA filament has a similar echogenicity and appearance to bone, and that the use of graphite powder in the printing material can improve image fidelity. 32 ,35–38
Six articles related to the use of 3D printing for vascular access simulation including femoral arteries and central and peripheral veins. 5 ,40–44 One study reported on the development of a partially 3D-printed intraosseous needle placement guide. 43 Sheu and colleagues developed a 3D-printed ultrasound-compatible femoral artery model that was compared to a commercial model in a randomised trial, which found there was no significant difference in training outcomes or confidence levels. 40 Another study demonstrated the validity of a pulsatile 3D-printed femoral arterial access simulator. 41 Pang and colleagues demonstrated the use of 3D printing to create a pelvic model with a veno-arterial vascular access system that was integrated with a standard cardiopulmonary resuscitation manikin for high-fidelity multidisciplinary simulations of extracorporeal cardiopulmonary resuscitation. 5
Three articles involved 3D printing of simulators for thoracostomy.45–47 Bettega and colleagues compared a 3D-printed thorax and an animal model for the simulation of chest drain insertion by 49 medical students and found that there was no significant difference in confidence or skill level between the two groups. 45 Others focused on the fabrication process of a model and use in remote telesimulation. 46 , 47
Three studies developed models for critical care simulation experiences, including incision and drainage of an abscess, 48 use of a 3D-printed cerebellum in a neurosurgical intraoperative cardiac arrest simulation, 49 and a 3D-printed shoulder model to create a simulation experience for ultrasound-guided intra-articular injections. 50
Procedural support
Sixteen articles related to 3D printing for support in procedures, including videolaryngoscopy (VL) blades (n = 5), intubation (n = 5), ventilation (n = 4) and tracheostomies (n = 2).
Five abstracts related to the design, production and testing of 3D-printed VL blades.51–55 A randomised controlled trial comparing the 3D-printed blade for VL and a Macintosh blade, involving 64 physicians, found that the VL group had significantly higher rates of first pass intubation success, shorter time to intubation, and better Cormack–Lehane grade views. 52 Another randomised controlled cross-over trial, that compared a standard C-MAC VL with a 3D-printed VL blade that utilised a disposable camera to transmit to a smartphone, found that time to intubation was equivalent but provided limited statistical analysis. 53 One study reported on the development of a steel 3D-printed laryngoscope designed for intubation with double-lumen tubes and reported successful testing in manikins. 55
Five studies related to the design of prototypes relating to the skill of intubation.56–60 A randomised controlled trial evaluated the performance of laryngoscopy using a 3D-printed ergonomic grip during simulation with medical students, and found it enabled a significantly shorter time to intubation and improved success rates in difficult intubation scenarios. 57 One study reported on the use of 3D-printed smartphone adaptors that allowed connection to an existing VL blade to improve visualisation. While the rate of successful intubation was high in both manikins and patients, participants reported difficulty with using the device and found there was an increase in time to intubation in the manikin group. 58 The three remaining studies involved 3D printing a laryngoscope handle that contained a thermoelectric generator to power a light source from the heat from the user’s hand, 59 a modified Magill’s forceps for tongue retraction during paediatric intubation 60 and a high-fidelity training device for cricoid pressure. 56
Four studies related to the development of customised devices to facilitate ventilation.61–64 These included a facial prosthetic to optimise mask fit in a patient with facial abnormalities and a silicone mask for a child with Trisomy 21, both constructed from 3D-printed negative moulds. 61 , 62 One study compared the use of an i-gel® (Intersurgical Ltd, Wokingham, Berkshire, UK) supraglottic airway with a 3D-printed modified version in 48 cadavers and found that there was a significant reduction in the force exerted on the airway mucosa and a significant increase in tidal volume during positive pressure ventilation with the printed device. 64
Two studies related to the creation of devices for tracheostomies. 65 , 66 A case study reported the use of a 3D-printed patient-specific tracheostomy tube in a patient who was unable to tolerate commercially available tubes. 65 A comparative trial of a novel 3D-printed translaryngeal tracheostomy needle introducer on 13 cadavers found that there were fewer puncture attempts, increased precision on first puncture and reduced time required for insertion when using the device in comparison to the standard needle insertion approach. 66
Other
There were four studies that did not involve any of the themes but met the inclusion criteria.67–70 Three studies used 3D printing to create anatomical models for the purpose of testing devices or to complete physiological studies, without the need to involve live patients.67–69 Zaylaa and colleagues created an incubator for preterm infants by printing parts of the incubator then incorporating circuity and a heating unit. 70 The 3D-printed incubator achieved higher scores in all measures compared with other incubation methods, including commercial incubators. 70
Discussion
In this scoping review we systematically identify applications relevant to critical care medicine that utilise 3D printing. These applications are largely related to simulation models for procedures of the airway, but include vascular access, spinal procedures, tube thoracostomy and bronchoscopy. Importantly, and although relevant to critical care medicine, nearly all of the articles were published in journals from other disciplines. Indeed, we conducted an ad hoc literature search using the term ‘3D printing’ in PubMed on 31 March 2020 and found a total of 9981 citations. However, none of these were in the leading discipline-specific critical care medical journals. This review highlights the unrecognised potential for 3D-printed applications in critical care medicine.
The recent coronavirus disease (COVID-19) health crisis, which has evolved since we embarked on this project, has brought the potential for 3D printing in critical care medicine to the forefront. There are now preliminary reports of a range of items being manufactured with 3D printing, including nasopharyngeal swabs, personal protective equipment, positive pressure valves and ventilator tubing. 71 , 72 3D-printed low-cost ventilators have been developed in several countries, including the USA, Spain and Lebanon.73–75 There has been significant support from professional bodies, private manufacturers, government organisations and individuals to address shortages of essential supplies, particularly through diversification of manufacturing capabilities, open source design instructions and crowdsourcing. 76
We found that a significant proportion of the literature pertained to simulation training. Simulation-based learning is widely used in critical care, in part due to the high risk and invasive nature of many procedures in this area of medicine. 77 There has been growing recognition that the traditional ‘see one, do one, teach one’ model of training is insufficient, with a move towards a ‘see one, do many with simulation, do one’ sequence. 41 , 78 , 79
Many of the studies included in our review detailed the manufacturing process for the use of 3D-printed devices and models. While beyond the scope of this report to detail these within the text, data are listed in the electronic Supplemental material and a detailed summary regarding the selection of printing materials has been published by Garcia and colleagues. 80
3D printing has the potential to increase the access to low-cost, low and high-fidelity simulations. Studies frequently noted that commercial devices, particularly simulation models, are expensive, and that 3D-printed devices can be produced at a much lower cost. These included studies involving simulation models for laryngoscopy, 18 , 19 front-of-neck access, 8 ,10–15 spinal and neuraxial procedures32–39 and thoracostomy,45–47 as well as laryngoscope blades. The ability to transfer electronic files and printing instructions further allows the dissemination of printed models and simulators to remote areas. Although in previous decades 3D printers were expensive and largely limited to commercial operations, they are now increasingly affordable and available for use by non-experts. We are currently developing a protocol to enable clinicians without 3D printing expertise to build a resuscitation manikin, including airway and cardiopulmonary resuscitation components, based on internet order and instructions for a total cost of approximately A$1000 inclusive of printer purchase. 5
Our review has a number of strengths and limitations that merit noting. Our review benefits from a structured, systematic and predefined search criteria and strategy. As our aim was to gain an understanding of the existing literature and gaps within it, we elected to utilise a range of broad search terms in multiple databases and we considered grey literature and unpublished data. While this strategy potentially increases the odds of including relevant articles, by limiting to three databases and to studies written in English some relevant articles may be missed. Indeed, one missed article on a bronchoscopy application was identified during peer review. We made no attempt to grade the quality of the literature included in this review as is standard for scoping reviews. 6
Conclusion
This scoping review identified that 3D printing is an under-researched and under-utilised technology in the critical care setting. The increasing ease of access and low cost of 3D printing will inevitably lead to innovations in critical care applications, and this will be propelled forward by the COVID-19 pandemic.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X20976655 - Supplemental material for Applications of 3D printing in critical care medicine: A scoping review
Supplemental material, sj-pdf-1-aic-10.1177_0310057X20976655 for Applications of 3D printing in critical care medicine: A scoping review by Natasha Abeysekera Kirsty A Whitmore Ashvini Abeysekera George Pang Kevin BLaupl and in Anaesthesia and Intensive Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.