
Abstract
This case report describes a patient who developed allergic contact dermatitis to a chlorhexidine skin preparation applied for a transversus abdominis plane block, but not to a different chlorhexidine solution applied to the surgical field. The patient had presented for an elective inguinal hernia repair. He had a known history of anaphylaxis to non-steroidal anti-inflammatory medication but was otherwise well. The surgery was completed uneventfully. Three or four days postoperatively, the patient developed a rash at the site where chlorhexidine skin preparation had been used to prepare the skin for the transversus abdominis plane block. The rash had well-demarcated edges and exactly matched the distribution of the previously applied skin preparation. No rash was present at the surgical site, which had been prepared with a different chlorhexidine-containing solution. The rash gradually resolved over several weeks with the application of topical corticosteroids. The patient was otherwise completely well with no evidence of infection or any other systemic illness. The skin preparations differed in the dyes and alcohols that they contained. The dyes or alcohol in the preparation for the transversus abdominis plane block were therefore considered the likely cause of this patient’s allergic reaction. Dyes and alcohols should be considered as a cause of skin allergy in the perioperative setting.
Introduction
Dyes and alcohols are often added to chlorhexidine skin preparations. Alcohols may contribute to the antiseptic qualities of the solution, while dyes help ensure that the skin is adequately covered. 1 The same dyes are commonly used in other products including medications, foods and cosmetics to improve their appearance or to produce their desired effect. 2 , 3
Many dyes are recognised as allergens. However, allergies to the dyes used in surgical skin preparations are rare. To the authors’ knowledge, there is only one published case report describing allergic contact dermatitis to a tinted chlorhexidine skin preparation. In this case, a patient demonstrated allergic contact dermatitis to a chlorhexidine skin preparation containing FD&C yellow no. 6 dye, but not to the same product without the dye. 4
Case reports of allergic contact dermatitis to isopropyl alcohol, an alcohol often found in chlorhexidine skin preparations, are similarly uncommon with only six identified during a literature search. However, in a European study of 1450 patients with a history of cutaneous allergy to products containing isopropyl alcohol, 44 (3%) had positive patch tests to isopropyl alcohol. 5 This suggests that exposure and sensitisation to isopropyl alcohol, while rare, may be more common than previously suspected.
Allergies to chlorhexidine itself occur in approximately 0.5% of the population and can be life-threatening. 6 It is a well-recognised allergen, due in part to the findings of the sixth National Audit Project. Chlorhexidine is included in many medical products, including medications, skin preparations and some indwelling urinary catheters. Therefore, a history of chlorhexidine allergy will often result in changes to a patient’s clinical management.
This report describes a patient who developed contact dermatitis following exposure to a chlorhexidine-based skin preparation. The patient would have likely been labelled as allergic to chlorhexidine had a second chlorhexidine solution containing different dyes and alcohols not been used during the same surgery.
This case, therefore, demonstrates the importance of considering all potential causes of periprocedural allergy in order to identify the causative agent correctly.
The patient gave verbal consent for this report, including the figure, to be published.
Case history
A 41-year-old man presented for an elective left inguinal hernia repair. He was in good health and took no regular medications, although he reported a history of anaphylaxis to the non-steroidal anti-inflammatory medication rofecoxib.
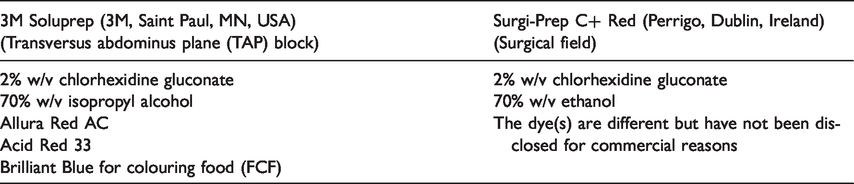
After induction of general anaesthesia and insertion of a laryngeal mask airway, the left middle abdomen and flank were prepped for a transversus abdominis plane (TAP) block with a Soluprep antiseptic swab, tinted (3M, Saint Paul, MN, USA). Following the TAP block, the surgeon prepped the left lower quadrant with Surgi-Prep C+ red solution (Perrigo, Dublin, Ireland) prior to draping and skin incision. Both solutions contain 2% chlorhexidine but different dyes and alcohols, as described in Table 1.
Constituents of the two chlorhexidine solutions.
Surgery and anaesthesia were uneventful, and the patient was discharged home the next day. Three or four days postoperatively, he developed a red, raised rash where the TAP block solution had been applied but not where the surgical field solution had been applied. The rash was most severe five or six days postoperatively but was still quite marked when photographed at a follow-up clinic visit 12 days postoperatively (Figure 1). At the time of this follow-up review, the patient had been applying a topical corticosteroid for several days. The patient reported that the rash had begun to settle with this treatment. A referral to a dermatologist or immunologist was considered at this clinic visit. However, as the rash was improving, was only mildly itchy and the patient was well and comfortable, a referral was not made. A follow-up telephone call was made on postoperative day 18. The patient reported that the rash was continuing to improve. It was during this telephone call that the patient provided consent for the publication of this case report.

The rash 12 days post--transversus abdominis plane (TAP) block. Please see attached JPEG image.
Discussion
The patient’s skin reaction is consistent with allergic contact dermatitis. This is the most likely diagnosis because the rash, including its clearly demarcated edges, exactly corresponds to the area in which the skin preparation for the TAP block had been applied. The time course of the rash and the absence of signs or symptoms of infection or systemic disease are also consistent with contact dermatitis. Differential diagnoses including trauma, localised skin infection and shingles were considered. The patient’s history did not reveal any traumatic injury. The distribution of the rash and the absence of oedema was not typical of erysipelas or cellulitis. The absence of systemic symptoms also made cellulitis unlikely. Shingles was similarly considered unlikely given the site of the rash had never been painful. The rash was also never vesicular nor pustular and did not follow a typical dermatomal distribution.
Contact dermatitis is a type IV delayed hypersensitivity reaction, which requires prior exposure to the allergen. The reaction typically manifests as erythema, vesiculation and pruritus, primarily confined to the site of contact with the allergen. 7 There are three distinct phases: In the first phase, with an initial exposure (unknown in this case), the allergen (hapten) binds to skin proteins. In the second phase, known as sensitisation, the hapten–protein complexes are engulfed by Langerhans cells and are taken to regional lymph nodes for priming of naive T cells. This results in clonal expansion of hapten-specific memory T cells. The final phase, elicitation, requires re-exposure to the hapten. Hapten–protein complexes are again formed, which are now presented to the antigen-primed T cells. This interaction initiates an inflammatory cascade which, over 24–48 hours, produces the clinical signs and symptoms of allergic contact dermatitis. 8
It appears that this patient has reacted to one of the three dyes (Allura Red AC, Acid Red 33, or Brilliant Blue for colouring food (FCF)), or to the isopropyl alcohol in the Soluprep solution used for the TAP block.
Allura Red is used in multiple foods, pharmaceutics and cosmetics. The European Chemicals Agency classifies Allura Red as non-irritating to eyes or skin based on animal studies. 9 A review by the World Health Organization similarly did not find evidence of skin irritation in humans. 10
Acid Red is used in multiple pharmaceutics and cosmetics. It has been shown to cause serious eye irritation, although data for skin reactions are lacking. 11 Animal studies have not demonstrated skin irritation on exposure to Acid Red; however, contact dermatitis from exposure to the dye in perfume has been reported. 12
Brilliant Blue has similar widespread uses to Acid and Allura Red dyes. While the European Chemicals Agency classifies Brilliant Blue as both a skin and eye irritant, a search of the literature could not identify a single case or study with such a reaction. 13
The mainstay of management of allergic contact dermatitis is avoidance of the allergen. 14 Skin patch testing may be useful to identify the offending allergen. Although symptoms may spontaneously resolve, treatment is often required to control symptoms. Topical corticosteroids are appropriate first-line therapy. 14 Referral to a dermatologist or immunologist may be considered to confirm the diagnosis and to identify the offending allergen and provide ongoing management.
In conclusion, this report describes a case of contact dermatitis after exposure to a surgical skin preparation. The likely precipitant was either isopropyl alcohol or a dye used to colour the solution rather than chlorhexidine itself, which is more commonly recognised as an allergen. This case therefore demonstrates the importance of considering all potential causes of periprocedural allergy in order to identify the causative agent correctly. Clinicians should be aware of the potential for these commonly encountered substances to cause allergy in their patients and that symptoms may present days after exposure, including after hospital discharge.
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.