
Abstract

The coronavirus (COVID-19) pandemic presents unique challenges to airway management. Numerous procedures carried out by anaesthetists, such as fibreoptic bronchoscopy (FOB), are aerosol-generating procedures and as such carry a high risk of viral transmission from infected patients to staff members. 1 However, such procedures may be unavoidable, with procedures such as video-assisted thoracoscopic surgery potentially requiring FOB at various times. To minimise the risk of viral transmission and the need for FOB, several studies support the use of an endotracheal tube with an embedded camera, although many are in agreement that bronchoscopy may still be necessary. 2 , 3 Other authors have proposed that procedures that involve a break in airway continuity (i.e. traditional FOB) should be done during apnoea with no continuous positive airway pressure (CPAP) or positive end-expiratory pressure (PEEP), and that FOB removal and reinsertion be kept to a minimum. 4 In this letter we describe a simple technique using readily available equipment for both right- and left-sided thoracic surgery that allows FOB to be carried out without a break in airway continuity during periods of ventilation or CPAP/PEEP.
For right-sided thoracic surgery, in addition to a left-sided double-lumen tube (DLT), an extra heat and moisture exchange (HME) filter, ultrasound probe sterile sheath (e.g. Protek Medical Products, Coralville, IA, USA) and a double swivel airway connector (DSAC) (e.g. Lovell Surgical Supplies, Seaford, Victoria) are needed (Figure 1). Pre-induction, the FOB is covered with an ultrasound probe sheath and the proximal end of the probe sheath (closest to the operator) is taped to the body of the FOB. A small hole is cut at the distal (patient) end of the ultrasound sheath, which then allows it to be taped to the DSAC. The DSAC is then connected to the tracheal lumen of the DLT and the additional HME filter is connected to the proximal (free end) of the DSAC. Once muscle relaxation is achieved, intubation with the DLT is performed in a standard manner.
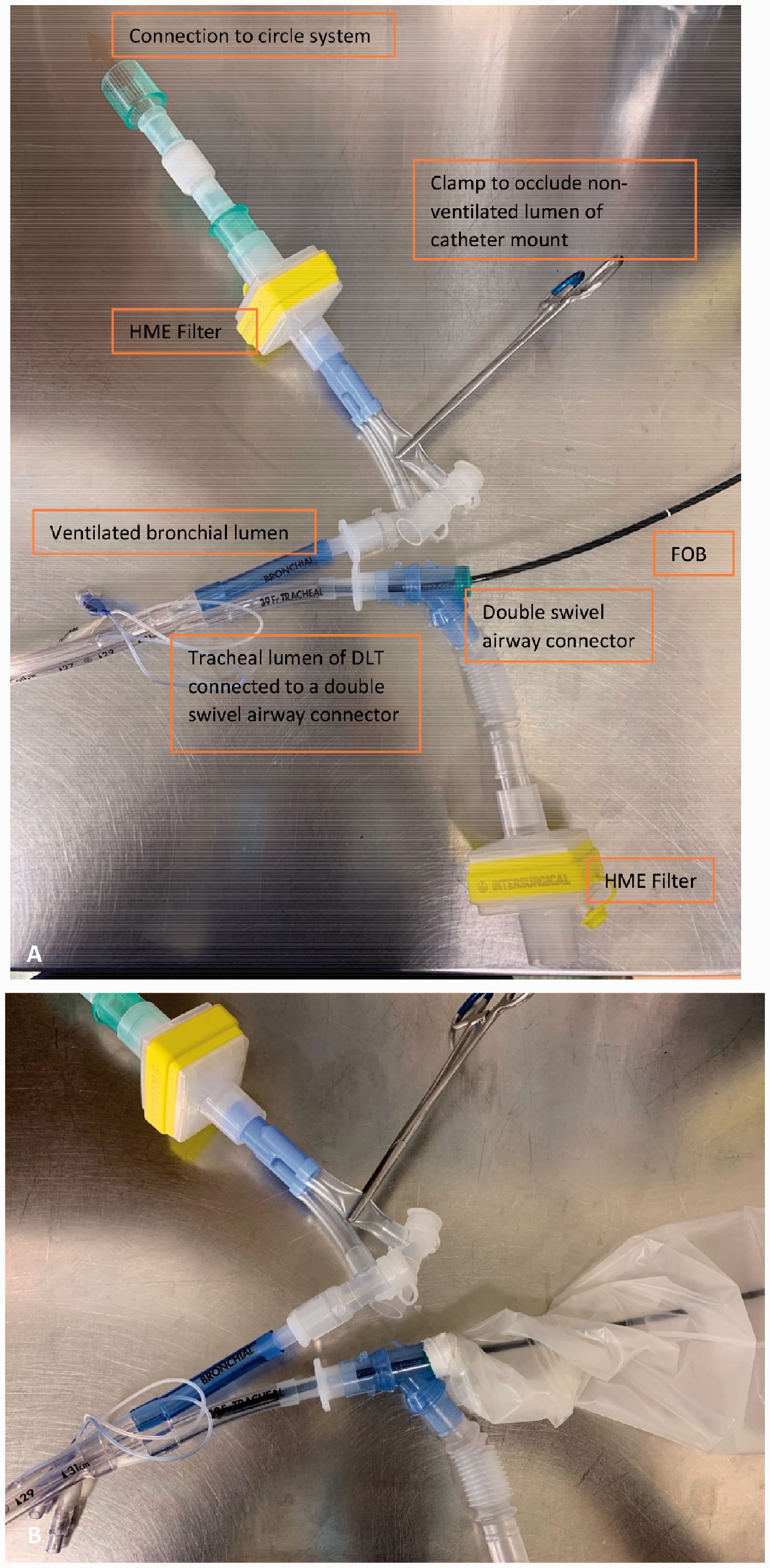
(a) Equipment setup for right-sided thoracic surgery using a left-sided double-lumen tube (DLT). Fibreoptic bronchoscopy (FOB) is carried out via the tracheal lumen and the bronchial lumen is ventilated. Ultrasound probe sterile sheath not shown for clarity. (b) Complete setup shown with the taped ultrasound probe sterile sheath over the FOB. Equipment shown: left-sided DLT (Covidien, Tullamore, Ireland), heat and moisture exchange (HME) filter (Intersurgical, Pabrade, Lithuania), double swivel airway connector (Lovell Surgical Supplies, Seaford, Victoria), ultrasound probe sterile sheath (Protek Medical Products, Coralville, IA, USA).
Next, the sheathed FOB is advanced into the tracheal lumen of the DLT through the DSAC and used to confirm the position of the bronchial cuff. Once cuff position is deemed satisfactory and the bronchial cuff is inflated, the bronchoscope is pulled back proximally into the tracheal lumen of the DLT and the DLT position is secured. Finally, suction tubing is connected to the capnograph port of the extra HME filter (where the capnograph tubing is usually connected). This will facilitate lung deflation on the operative side. In our limited experience, there has been no resistance to lung deflation with this technique. Using this technique, repeat bronchoscopy can be carried out as desired without necessitating apnoea or removal of PEEP/CPAP, as there is no break in airway continuity. At the conclusion of surgery, the equipment used is disassembled during a period of apnoea and both lungs are ventilated through the two lumens of the DLT. Following extubation the equipment used is either disposed of or sterilised in accordance with recommended infection control practices.
For left-sided thoracic surgery, the equipment required is a left-sided DLT with an embedded camera (e.g. Vivasight; ETView Ltd., Misgav, Israel), a DSAC and an extra HME filter (Figure 2). We believe that having an embedded camera negates the need for FOB unless complications occur during surgery. Similar to the setup detailed above, the DSAC is attached to the operative (bronchial) side of the DLT with the extra HME filter at the proximal end (Figure 2). Induction and intubation is performed and ventilation achieved through the tracheal lumen. This initial setup allows for continuous visualisation of the bronchial cuff position without further airway manipulation, while allowing the flexibility to insert an FOB down the bronchial lumen using the sheath setup detailed above if required.
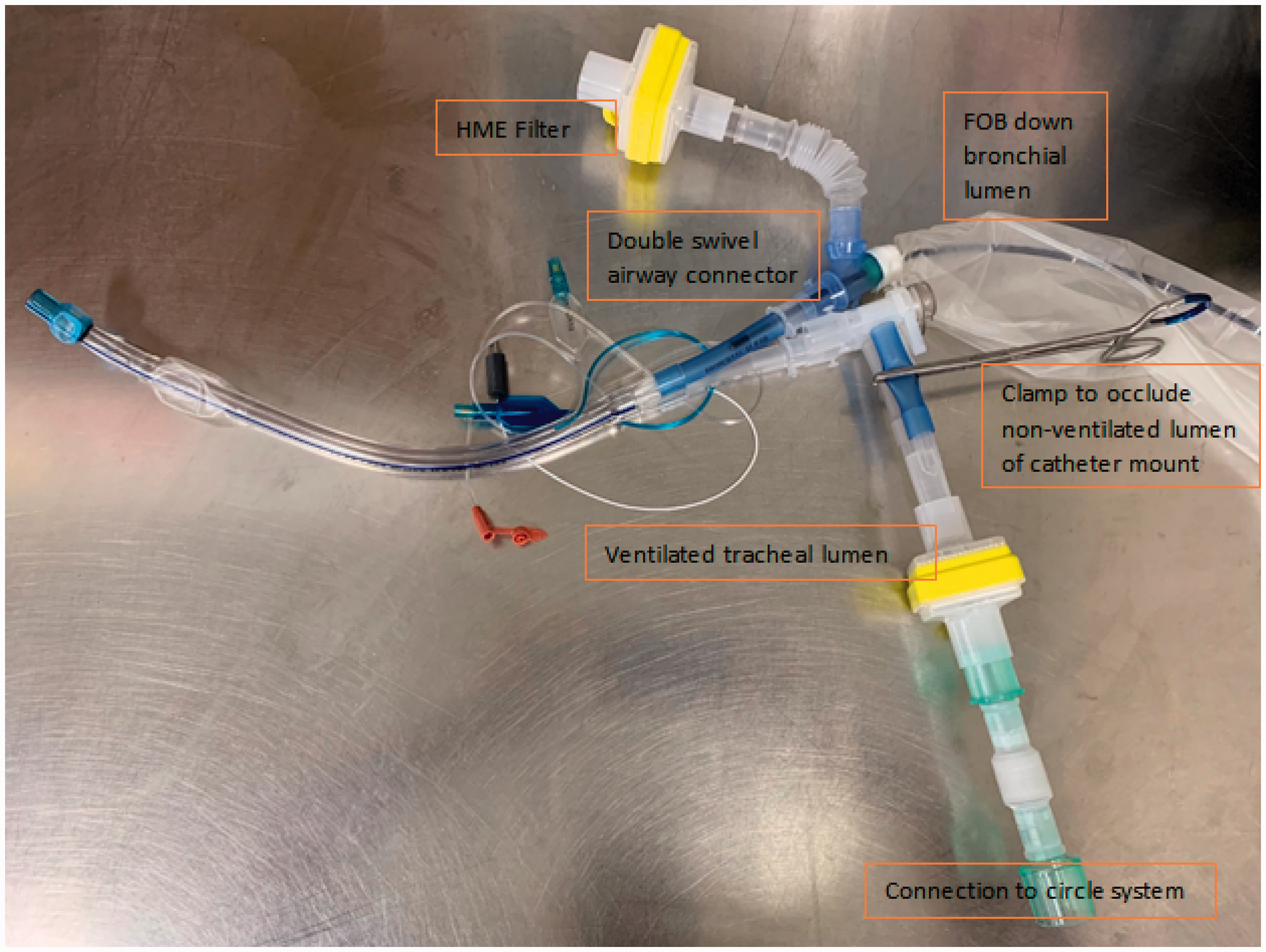
Equipment setup for left-sided thoracic surgery using a left-sided double-lumen tube (DLT) with an embedded camera. If required, fibreoptic bronchoscopy (FOB) can be carried out via the bronchial lumen. Equipment shown: left-sided DLT with an embedded camera (Vivasight; ETView Ltd., Misgav, Israel), heat and moisture exchange (HME) filter (Intersurgical, Pabrade, Lithuania), double swivel airway connector (Lovell Surgical Supplies, Seaford, VIC, Australia, Victoria), ultrasound probe sterile sheath (Protek Medical Products, Carolville, IA, USA).
An analogous setup to that described above for left-sided thoracic surgery may also be used for right-sided thoracic surgery (i.e. using a left-sided DLT with embedded camera). However, we have described the use of a left-sided DLT without an embedded camera for two reasons; firstly, to illustrate the setup, and secondly if FOB is likely to be required there are cost savings associated with the use of a DLT without an embedded camera. Furthermore, the sheath and FOB setup may be inserted down either limb of the DLT so long as there is a period of apnoea and clamping of the open limb of the DLT.
In the equipment setup detailed above, the taped seal minimises the escape of aerosol around the DSAC valve during FOB. It also allows for repeated bronchoscopy and the use of simultaneous ventilation/CPAP/PEEP without the increased risk of pathogen transmission due to a break in airway continuity. We believe this easily assembled, cost-effective setup allows for safer FOB during thoracic surgery. However, even with this knowledge, a discussion should still be carried out pre-induction with the surgical team regarding the use and risks of FOB, and that its use should be limited to patients who have complex anatomy or complicated surgery.
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.