
Abstract

Safe airway management of patients with suspected or confirmed severe acute respiratory distress syndrome coronavirus 2 (SARS-CoV-2) is a priority during the current pandemic. Tracheal intubation is a high-risk aerosol-generating procedure associated with healthcare worker infection (HCWI), 1 and potentially with the spread of SARS-CoV-2. Expert recommendations have provided guidance to protect healthcare workers and optimise patient outcomes. 2 Good quality audit data are essential for feedback and allow pragmatic modification of airway protocols during this highly dynamic pandemic environment. In parallel to an international registry aimed at identifying the risk of intubation and subsequent HCWI (intubateCOVID), 3 we undertook a multicentre observational audit of suspected or confirmed coronavirus disease (COVID-19) intubations in New South Wales (NSW) metropolitan hospitals. The aim of this audit was to investigate the characteristics of patients undergoing COVID-19 intubations and aspects of healthcare worker safety, and to solicit feedback for continuous quality improvement in an Australian context.
Six metropolitan public hospitals responded to an invitation to contribute to a multicentre audit via the NSW Anaesthesia Research Collaborative Network (NARCoNet). Ethics approval was granted by the human research and ethics committee of St Vincent’s Hospital (2020/ETH00999) and the audit was registered on a publicly accessible clinical trial registry (ACTRN1260000617965). A standardised data collection form was provided to all sites. De-identified patient data were electronically sent to authors GK and EBM for analysis. Patients were included if they were identified as suspected or confirmed COVID-19 and required intubation. Intubations took place between 16 March and 5 June 2020. Parametric data are reported as mean and standard deviation, and non-parametric data as median and interquartile range (IQR).
A total of 82 intubations in 77 patients were included. Patient characteristics and intubation data are presented in Table 1. Seventeen intubations (21%) were performed on 14 patients with confirmed COVID-19.
Patient characteristics and intubation data.
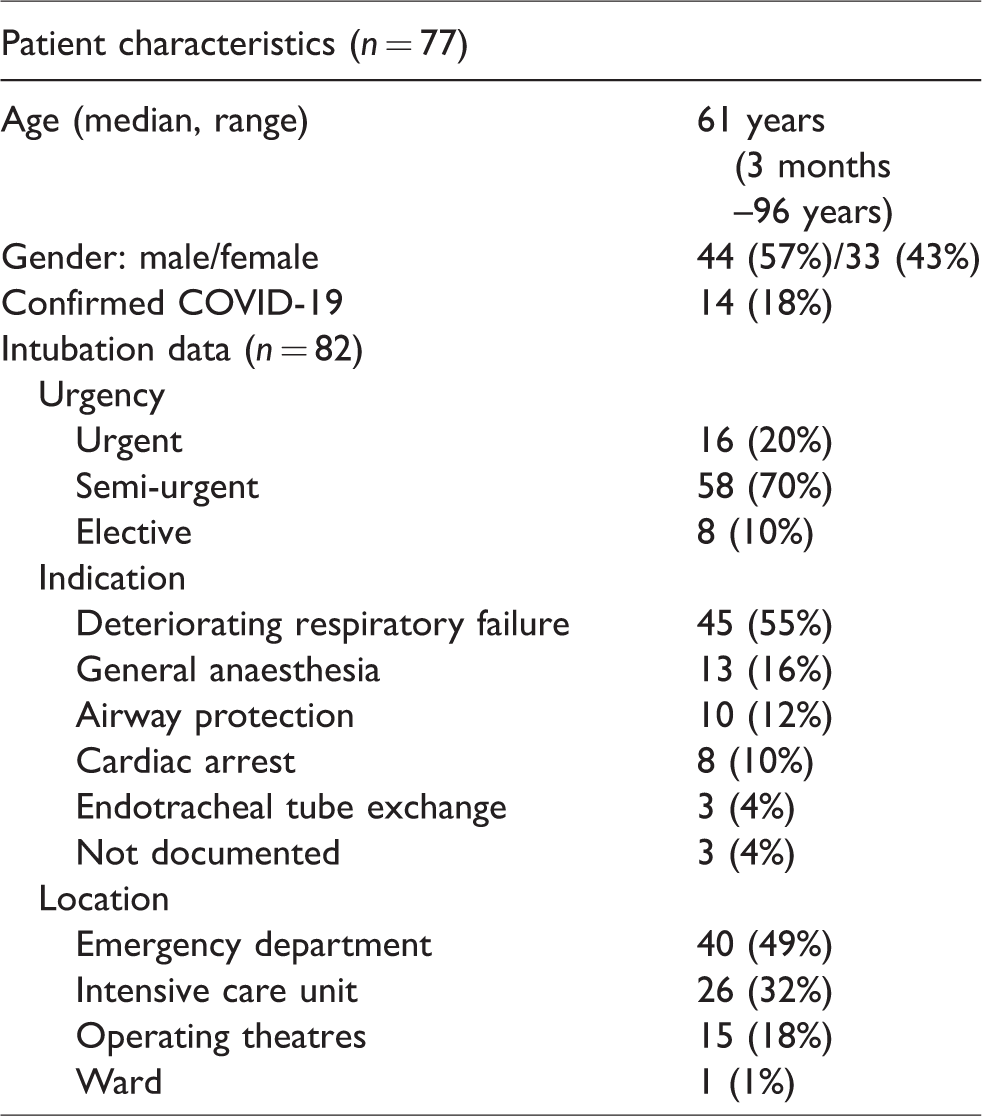
The median time between a request for intubation and performance of the procedure was 31 and 50 minutes for urgent and semi-urgent cases, respectively. The intubation was performed by a consultant anaesthetist in 94% of cases. In 46% of cases the assistant to the airway doctor was an intensive care or emergency department staff member. Two-thirds of intubations were performed in a negative pressure room. Appropriate personal protective equipment (PPE) was available and worn in 98% of cases. Gross contamination of staff was reported in two cases, and there were no reports of breaches in PPE or accidental breathing circuit disconnection.
Intubations were performed predominantly (85% of cases) with videolaryngoscopes. Only one case required a second attempt at intubation. The median oxygen saturation (SpO2) prior to pre-oxygenation was 92% (IQR 88%–97%), and after pre-oxygenation was 99% (IQR 95%–100%). The lowest median SpO2 recorded during intubation was 94% (IQR 80%–99%). Hypotension (systolic blood pressure <80 mmHg) occurred in 25 (31%) of cases, and two patients aspirated during induction. Six patients (7%) required rescue bag–mask ventilation, four patients (5%) coughed on intubation and two (2%) patients had a cardiac arrest.
In those patients subsequently confirmed to have COVID-19 the rate of SpO2 less than 85% was 53% versus 22% in those who did not have COVID-19. Hypotension occurred in 31% of COVID-19–positive cases versus 32% of negative cases. The two patients who had a cardiac arrest were both COVID-19 negative. Three (18%) COVID-19–positive patients required rescue bag–mask ventilation, as did three (5%) patients who were COVID-19 negative.
Feedback provided in free text was analysed for thematic content. Of 38 feedback items, 16 related to PPE donning and doffing, 12 related to equipment issues and six related to human factors. Examples that allowed timely corrective action included: lack of laminated donning/doffing cognitive aids leading to disposable printed cognitive aids being included in PPE packs; difficulty visualising when using videolaryngoscopes draped in plastic leading to increased use of videolaryngoscopes with handle-mounted monitors; poor team leadership and performance prompting increased simulation with closed-loop communication.
This is the first report to provide local Australian data on airway management during the current SARS-CoV-2 pandemic. Anaesthetists provided a high level of airway support to patients with suspected COVID-19 outside of the operating theatre environment and in teams with personnel from emergency departments and intensive care units.
Our data show anaesthetists to be working in non-routine locations, in a multidisciplinary team, with critically ill patients. A significant proportion of feedback related to PPE donning and doffing and may reflect clinician anxiety related to HCWI. Such high stress environments lend themselves to in situ simulation training, 4 and we would recommend that in situ multidisciplinary team training incorporating PPE donning, COVID-19–specific airway management, equipment familiarisation, crisis resource management and PPE doffing be routinely performed in hospitals expecting COVID-19 surges. 5 Simulations during this period should be in small groups and maintain social distancing when practical, due to reports of transmission of virus by infected participants. 6
The suspected COVID-19 patients undergoing airway management represented a critically ill population with minimal respiratory reserve, with severe desaturation (SpO2 <85%) occurring more frequently in COVID-19–positive patients. The prolonged duration required for donning PPE and pre-intubation setup along with high rates of significant desaturation should be taken into account. Rescue bag–mask ventilation may be required, as reported by others. 7
Reassuringly, PPE standards were met in a higher proportion of intubations than a voluntary international registry that reported appropriate PPE in 87.8% of intubations. 3 Also, despite patients’ critical illness, intubations were performed with low rates of complication, and first attempt intubation success was high. This may reflect the participation of consultant-level clinicians during intubation of these patients and the longer lead time experienced in Australia that allowed for greater preparation and training.
The limitations of this audit include potentially reduced generalisability of the findings to locations outside of metropolitan NSW. Hospital participation was voluntary and may introduce selection bias. In addition, Sydney, and Australia in general, did not have to cope with an overwhelmed medical system and remained well resourced throughout the study period, unlike other comparable international locations.
This study provides timely Australian data on patient characteristics and airway management during COVID-19 intubations. Our data support senior clinician involvement in the care of these patients, ongoing team training and continuous departmental quality improvement feedback. The situation continues to evolve rapidly and such data may inform individual hospitals as they plan to deal with continuing surges of COVID-19 patients.
Footnotes
Acknowledgements
The author(s) would like to thank the NSW Anaesthesia Research Collaborative Network (NARCoNet) for facilitating this audit.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.