
Abstract

There has been interest in simulating aerosolisation during the COVID pandemic to look for contamination and potential spread of infectious material. Procedures associated with aerosolisation include intubation, extubation, nebulisation, bronchoscopy and coughing. Methods used to simulate the spread of fluorescent powder and dye include the use of latex balloons with compressed oxygen 1 or a cough simulator. 2 Here we describe a low-cost technique, using equipment readily available in the operating theatre, to simulate aerosolisation of these particles, which we hope will be useful for other investigators researching personal protective equipment (PPE) and the spread of infectious droplets.
We used Glo Germ (Marlatek Inc., Brockville, ON, Canada), an ultraviolet (UV) fluorescent powder 5 microns in size, for our simulation. To simulate a cough in a manikin, we removed one lung from a Laerdal airway management trainer manikin (Laerdal Medical, Stavanger, Norway) and passed a 12 Fr suction catheter into the bronchial opening for the lung up the trachea to around the level of the vocal cords. The suction catheter was then attached to a Sanders type manual jet injector. We applied 1 tsp and ½ tsp of Glo Germ into the oropharynx of the manikin and around a size 4 Ambu AuraGain (Ambu A/S, Ballerup, Denmark) laryngeal mask airway (LMA), respectively. The LMA was subsequently inserted and the cuff was inflated. We then delivered a very brief jet of less than one second at 4 bar. This generated a large dispersal of Glo Germ that could be captured in the darkened room using a UV light torch (Figure 1(a)). Figure 1(b) shows the resultant contamination of one of the authors simulating the LMA removal while in PPE, whereas Figure 1(c) demonstrates the simulated patient’s surroundings. Permission was obtained to publish these photos.
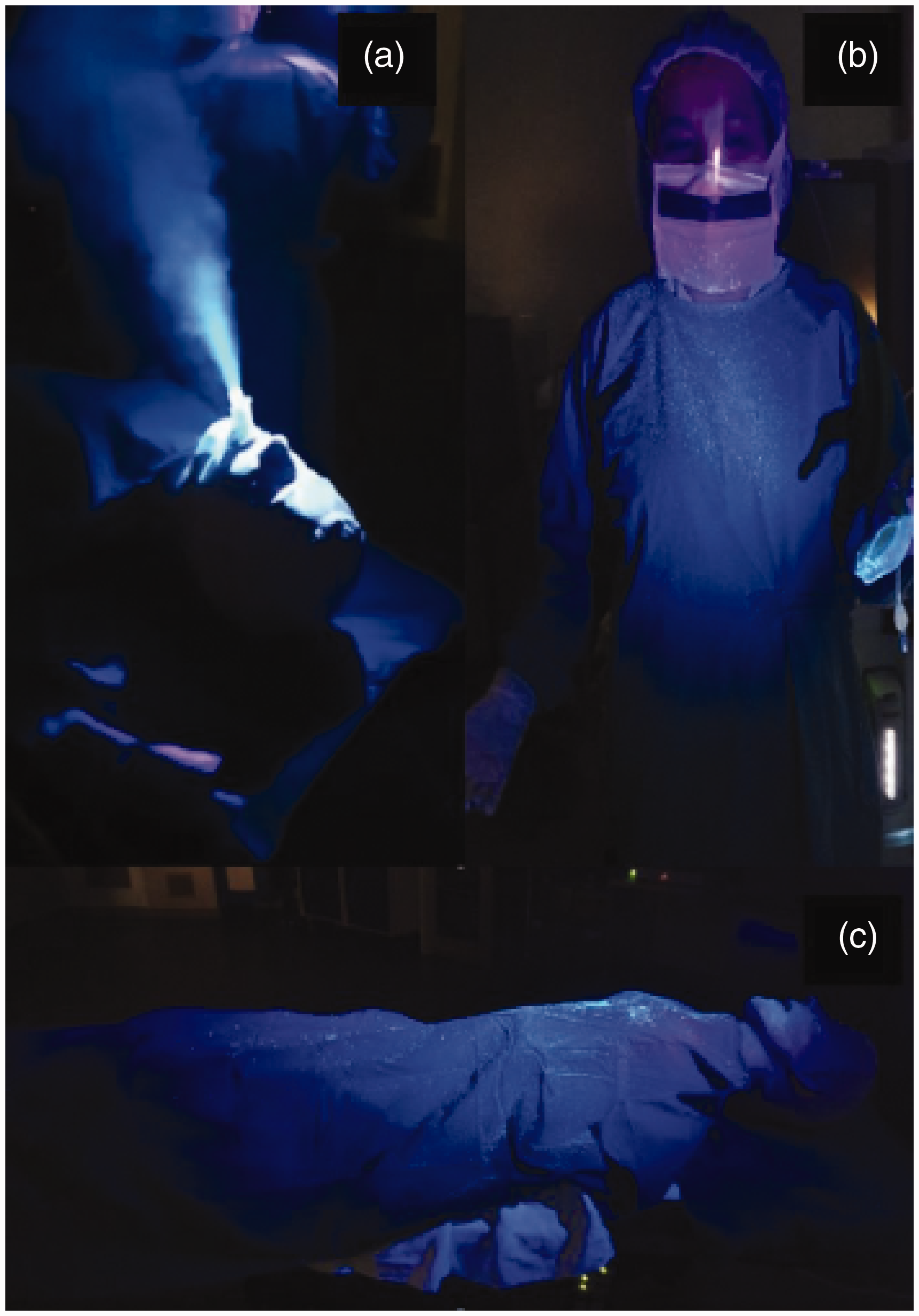
The dispersal technique for fluorescent powder to simulate the spread of aerosols: (a) ‘cloud’ generation; (b) healthcare worker contamination; (c) environmental contamination over torso of the manikin.
Previously, we used the technique described by Gardiner et al. 3 and inserted a 6.0 mm internal diameter tracheal tube filled with Glo Germ in the bronchial lumen, along with a 3 ml syringe with Glo Germ and an elbow connector, but failed to generate any dispersal of Glo Germ in our manikin by squeezing a self-inflating resuscitator bag. We postulate that this may be due to the type of manikin used, with some variation in anatomy and material.
As there has been interest in the aerosolisation of particles during nebulisation, we attempted to study the same spread with nebulisation, but this was not successful. This is likely to be due to Glo Germ affecting the viscosity of 0.9% saline in which it is suspended, leading to limited dispersal of Glo Germ when used with a nebuliser mask.
We hope that this will be a useful and accessible technique for researchers studying infection control practices.
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.