
Abstract

We still believe that the administration of 100 per cent oxygen, or as near that percentage as it is possible to give, in cases where oxygen is indicated is conducive to the best therapeutic results and is without harmful effects to the patient.
John Evans and Clarence Durshordwe, October 1934. 1
Despite the growing popularity of nasal cannulae for the delivery of supplemental oxygen during the early 1930s, 2 researchers began to question the efficiency, economy and comfort of these devices, as well as their ability to supply the high concentrations of oxygen recommended by some clinicians. 1 , 3 , 4
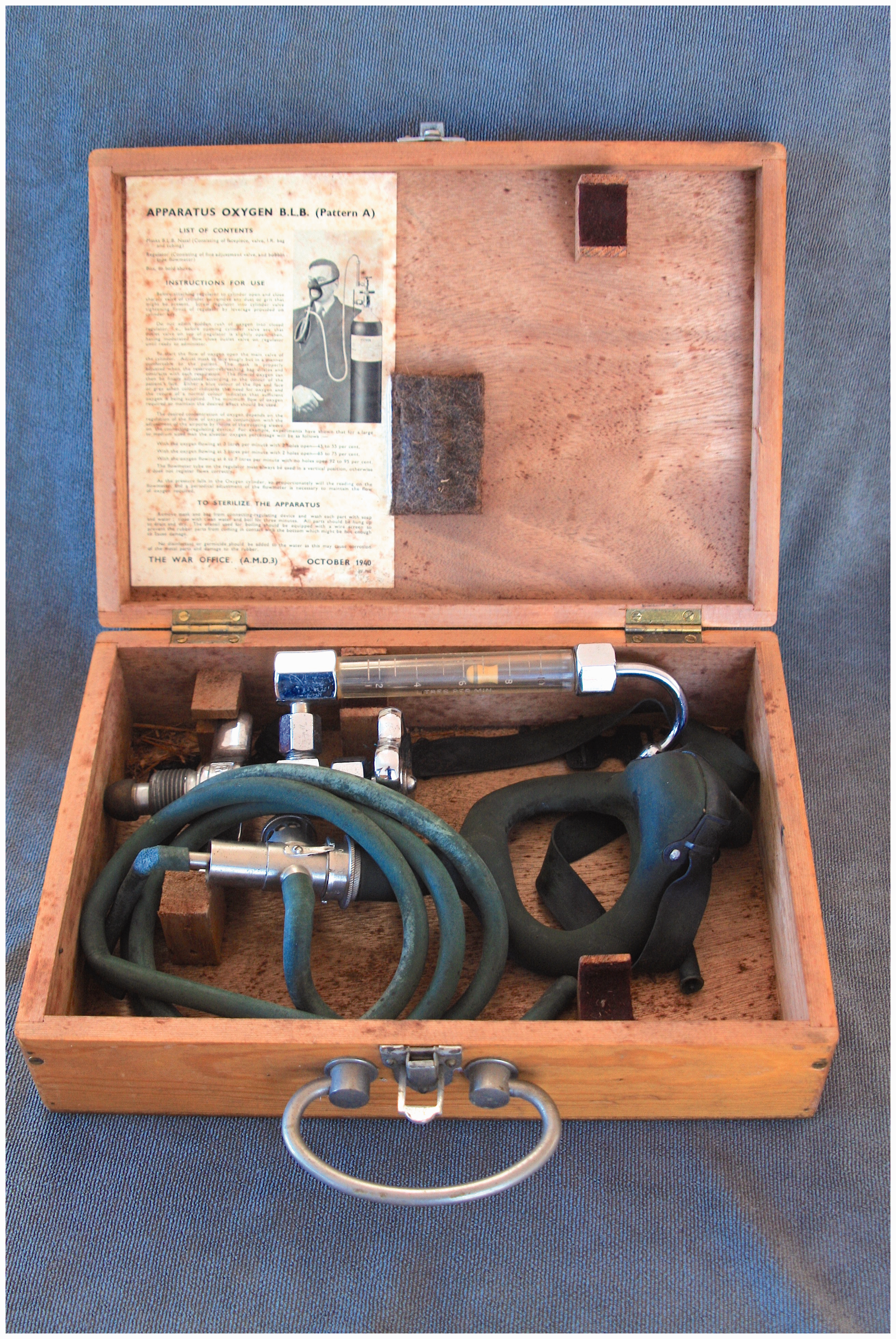
https://ehive.com/collections/4493/objects/1095439/blb-oxygen-aviator-mask-and-cylinder-attachment.
In 1936, J Argyll Campbell and colleagues at the National Institute for Medical Research, Hampstead, introduced a novel box mask made from thin aluminium, or cardboard. Oxygen entered the top of the mask via a No. 9 or No. 11 red rubber catheter, the end of which was either inserted three inches into the patient’s nasopharynx, or left hanging slightly above the level of the nose. The front of the mask included a door which could be opened to facilitate the administration of medication or consumption of food, and the rear incorporated a bottle-shaped opening to accommodate the nose, mouth and chin. The bottom of the mask was freely open to the air; a thin strip of lint was fitted around the lower edge to soak up condensation running down the inside of the mask. Campbell compared the performance and comfort of the box mask against existing nasal cannulae and forked nasal tubes, reporting that it required lower gas flows, delivered higher alveolar oxygen concentrations (60%–70% with a flow of 7 l/min) and proved more tolerable than the other devices. 3
One year later at Columbia University, New York, Alvan Barach developed an ‘oxygen face tent’. 4 This was similar in concept to Campbell’s box mask, but was fashioned from light, transparent ‘plastocoele’ (celluloid acetate). 4 Oxygen was introduced through a perforated rubber tube running horizontally along the top of the mask. Originally designed for the ‘treatment of anoxemia occurring in clinical disease’, Barach suggested that the face tent could also be used to prevent transcontinental airline pilots developing ‘mental impairment and physiologic alterations’ secondary to ‘oxygen want’ when flying their unpressurised aircraft above 10,000 ft. 4
Barach’s paper ‘vividly called the attention of the medical profession and individuals connected with commercial aviation to the dangers that could arise from oxygen want and the possibility of accidents arising therefrom’. 5 Soon after its publication, the President and Director of Northwest Airlines met with Charles W Mayo and Walter Boothby from the Mayo Clinic, Rochester, Minnesota, and expressed their desire to obtain a ‘simple and efficient apparatus for the administration of oxygen to aviators at high altitudes’. 6
Boothby, together with W Randolph Lovelace II and Arthur Bulbulian, went on to design an inexpensive, low maintenance device which, in addition to meeting the needs of the airline industry, was ‘equally as suitable for use by the family physician in the patient’s home’ as it was in ‘large well-equipped hospitals’. 6
Named after its three designers, the BLB mask permitted the ‘efficient, simple, comfortable, safe and economical’ administration of oxygen, or mixtures of oxygen and helium, ‘in any desired concentration’. 5
Made from rubber, the original BLB apparatus comprised either a nasal or oronasal mask, joined to a 500 cc. ‘reservoir-rebreathing bag’ by means of a metallic ‘connecting and regulating device’. 5 Fresh oxygen (or oxygen and helium) entered via an inlet on the connecting and regulating device and was delivered through a tube to the bottom end of the reservoir-rebreathing bag. Gas then passed up to the mask through the connecting and regulating device. In addition to the inlet valve, this included an air-regulating mechanism, consisting of three small openings, over which was mounted a rotating sleeve incorporating three similar sized ‘portholes’. 5 When aligned, these allowed a variable amount of atmospheric air to be entrained during inspiration. In the case of commercial aviation, it was envisaged that pilots would open two portholes below 15,000 ft, and one when flying between 15,000 and 30,000 ft. Above this height, all three portholes would be closed and ‘only pure oxygen … would be inspired’. 5 Expired gases passed back down into the reservoir-rebreathing bag, where they mixed with incoming fresh gas. Distension of the bag caused an expiratory valve on the connecting and regulating device to open, with preferential venting of expired alveolar gas.
The BLB apparatus was initially trialled on 125 patients at the Mayo Clinic over a five-month period. These included cases of pneumonia and acute pulmonary oedema, but also individuals with gaseous abdominal distension, and headache following air encephalography, in whom the prolonged administration of 95%–100% oxygen appeared beneficial. 7 Lovelace concluded that the mask’s ‘ability to administer high concentrations of oxygen economically opens up an entirely new field for oxygen therapy; many types of conditions hitherto not materially helped by … ordinary concentrations of oxygen … have been definitely benefited by high concentrations’. 5
Concomitantly, the device was subject to extensive ground and air testing at Wright Army Airfield, Ohio, before being utilised during a round trip flight between Minneapolis and Los Angeles in a Northwest Airlines Lockheed Zephyr. En route, the aircraft reached a maximum altitude of 31,000 ft; normal alveolar concentrations of oxygen and carbon dioxide were maintained with an oxygen flow of 1.8 l/min. 5
The mask subsequently underwent several modifications, and versions of the device were employed by allied air crews, as well as military and civilian hospitals throughout the Second World War. 8 During this conflict, several improvised masks capable of delivering high concentrations of oxygen were also devised. In London, Alice Rose and T Holmes Sellors described a cone-shaped face-tent made from a sheet of discarded X-ray film, 9 and Hugh Marriott modified a civilian gas mask by stretching the cut end of a rubber football bladder over the mask’s canister. 10 The inlet tube of the football bladder was then connected to tubing from an oxygen cylinder. The conversion from gas mask to makeshift oxygen face-piece could be achieved ‘within a minute’ and involved ‘no meddling with the construction of the respirator’. 10
While BLB-type masks remained in clinical use for several decades, 11 the dangers associated with the administration of high fractions of inspired oxygen were increasingly recognised. In 1960, EJ Moran Campbell argued that patients with respiratory failure should receive oxygen concentrations in the range 24%–35% controlled with an accuracy of ±1%. He designed the Venturi mask, which utilised the principle of high airflow with oxygen enrichment (HAFOE) to deliver a predetermined and fixed concentration of oxygen. 12