
Abstract

As humans we tend to perceive what we expect to perceive. In a medical setting, this means that the type of language used to communicate with patients influences their expectations and experience. Research dating back to the 1960s has shown that good communication during the patient–anaesthetist interaction reduces anxiety, stress, postoperative analgesia requirements, length of stay and improves patient satisfaction.1–3 There is a variety of specific language techniques (Table 1) which research suggests can benefit or harm patients,4–7 many were mentioned in a recent article by Cyna in this journal. 3
Language and communication techniques explored in this audit.

We conducted an observational audit to assess the frequency with which senior anaesthetists used specific language techniques including rapport building (e.g. discussing personal topics, attentive listening, reflective listening), nocebo language, positive suggestion and simple relaxation techniques (e.g. guided relaxation, lived-in imagination). The investigator (ANC) observed a convenience sample of 30 specialist anaesthetists during 57 interactions in the operating theatre before the induction of anaesthesia.
Audit findings
Rapport building was used in 95% of interactions, with discussing personal topics the most common technique (85%). Reflective listening was observed in only seven interactions (12%). The investigator observed that anaesthetists frequently used attentive (or passive) listening (Table 1). For patients, attentive listening can increase anxiety, because it may be interpreted as a dismissal of their concerns.
7
For example: Patient: I’m scared. Doctor: That’s ok, it’s normal to be scared.
Attentive listening can be transformed into reflective listening by seeking clarification and then exploring what is being said, for example: Patient: I’m scared. Doctor: You say you are scared. What are you scared of?
A nocebo word or phrase was observed in 77% of interactions. The most common nocebo words were ‘scratch’, ‘burning’, or ‘sharp’, seen in 25%, 21% and 18% of interactions, respectively. The most used nocebo phrase, seen in 68% of interactions, was ‘to stop you feeling sick/pain’. The use of such language increases perioperative anxiety and pain.3,4,6,7 Neutral phrases and open-ended statements are an alternative to nocebo language.3,5,6 The following are some examples of nociceptive phrases (in italics) and possible alternatives: “It’s a sharp scratch and it may sting a little.” OR “This may hurt a little.” “I am going to apply the tourniquet on the arm. As I do this many people find that the arm becomes heavy, numb, and tingly.” “I'm using local anaesthetic to numb the skin and make the procedure as comfortable as possible.” “I am going to give you an injection now.” “You may or may not feel something.” “We will give you medicines to stop vomiting after your surgery.” “We will give you medicine to ensure that you can eat and drink as soon as you feel like it.” “We'll give you something to help settle your tummy so you can feel like eating and drinking.” “This medication may make you dizzy or lightheaded.” “You may feel some changes from the medication.” “What is your pain like?” OR “What is your pain score?” OR “How bad is your pain?” “Are you comfortable?” “Is there anything I can do to make you more comfortable?”
The observed use of positive suggestion or guided relaxation was 20% and 11%, respectively. Lived-in imagination was not used in any of the observed interactions. The use of these techniques by medical professionals has been shown to reduce anxiety, premedication use, postoperative pain, constipation and improve recovery time and appetite.2,3,7,8 As patients’ openness to suggestion (and susceptibility to nocebo language) increases when highly anxious, distressed, in pain or pregnant,8,9 the anaesthetist perioperative visit seems an optimal time to maximise these beneficial techniques.
Limitations
There were some clear limitations to this audit. First, the observations took place shortly before the induction of anaesthesia, and earlier interactions during assessment and consenting of patients were usually not observed. Second, the observations were made by a single observer (ANC) and there was no independent checking of observations by a second investigator. Third, anaesthetists may have altered their use of language knowing that they were being observed.
Practical implications
While this was a small audit in a single department, our findings may have relevance to other departments in Australia and New Zealand because of a similar training and work culture. The terminology related to communication techniques is variable and we have provided a simple classification with examples to aid understanding. The audit itself increased interest in and awareness of language use within our department, and our findings suggest clear areas for improvement: increasing the use of reflective listening, learning and using positive suggestion and basic relaxation techniques, and reducing the use of nocebo language. We have developed a communication lanyard card to raise awareness and provide prompts for improved communication in everyday practice (Figure 1). An intranet webpage has also been developed and two of the authors helped to organise a workshop on distraction and guided imagery. We hope to perform a study in the near future to compare the self-reported and observed use of specific language techniques.
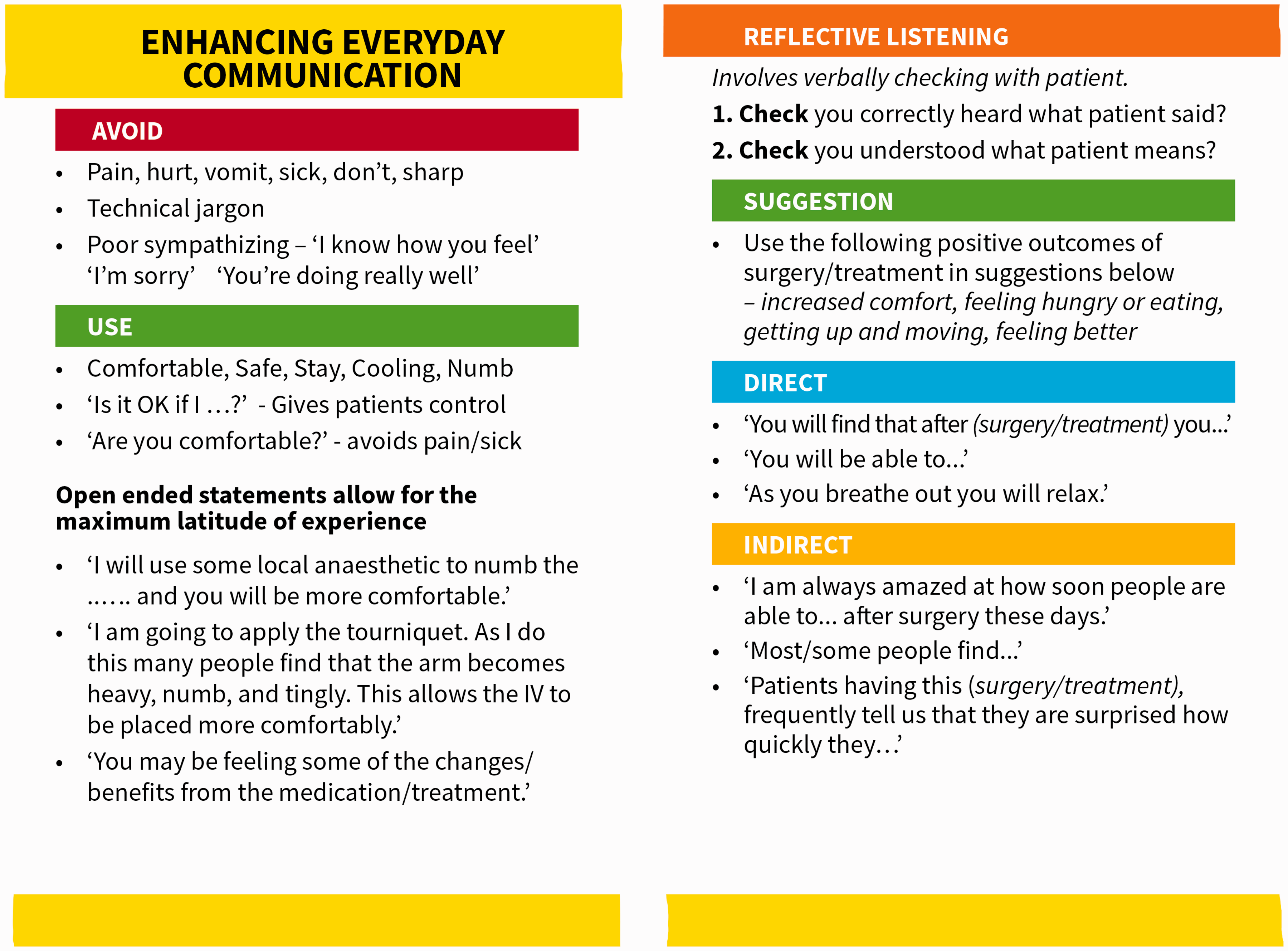
Lanyard card.
In summary, research has consistently shown that improved communication skills increase patient satisfaction and decrease patient anxiety.3,10 This audit has increased awareness of communication techniques and suggested areas for improvement within our department. Communication is a vital part of an anaesthetist’s skill set—please mind your language!
Footnotes
Acknowledgements
The author(s) acknowledge the support from participating anaesthetists at Christchurch Hospital in New Zealand. They would also like to acknowledge the support and guidance from Associate Professor Ross Kennedy in writing this article.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.