
Abstract
An example of the East–Freeman Automatic Vent from Oxford was found in the early anaesthesia equipment collection at St George Hospital, Sydney. It weighs less than 200 g and is representative of a group of miniature ventilators that were described in the 1960s, including the Minivent from South Africa and the Microvent from Canada. All relied on a pressure-operated inflating valve that was described in 1966 by Mitchell and Epstein from Oxford. The ventilators were compact, portable and were powered by the gas supply from the anaesthesia machine or other driving source that distended a reservoir bag. The main problem was that they could stick in the inspiratory phase. This led to pressure in the lungs rising towards the driving pressure. There was a risk of barotrauma to the patient if the system was not promptly disconnected. While theyhad provided an alternative to hand bagging, they were superseded, as more sophisticated and safer ventilators became widely available.
Keywords
An example of the East–Freeman Automatic Vent was found while cataloguing a collection of early anaesthesia equipment at the anaesthesia department at St George Hospital in Sydney. The catalogue of this collection is available online. 1
The device is a small, robust aluminium T-connector weighing less than 200 g, accompanied by a perished rubber bag (Figure 1). There is no record of how it came into the collection, or whether it had been used clinically at the hospital.

The East–Freeman Automatic Vent in the collection of the St George Anaesthesia Equipment Museum (courtesy of St George Department of Anaesthesia).
It was patented by Maurice Frederick Freeman of Cumnor Hill, Oxford, England on 2 June 1970 and manufactured by HG East and Company.
2
The patent describes it as Respiratory apparatus comprising a nonrebreathing valve capable of regulating the breathing of a patient during medical treatment where air or other gas to be administered to the patient is pressurized for forced ventilation.
2
Maurice Freeman’s early career was with HG East and Co, with his prime interest being in ventilators. He became managing director and was instrumental in the formation of Barema (the Association for Anaesthetic and Respiratory Device Suppliers) in 1976 together with BOC, Blease, Penlon, Cape Engineering and MIE, and was appointed chairman. He remained in that role until his retirement in 2012, with the membership comprising close to fifty companies. In 1991 he joined the European Commission as technical expert and chaired many groups and committees involved in the development of safer technical standards for medical equipment.
In 2000, Maurice Freeman received the Pask Award 5 from the Association of Anaesthetists of Great Britain and Ireland (AAGBI ) in ‘recognition of his wise and valuable advice to AAGBI over many years in the pursuit of the highest standards in the manufacture of equipment for anaesthesia and resuscitation’. He died in 2018. 6
The construction of the East–Freeman Automatic Vent is illustrated in Figure 2.
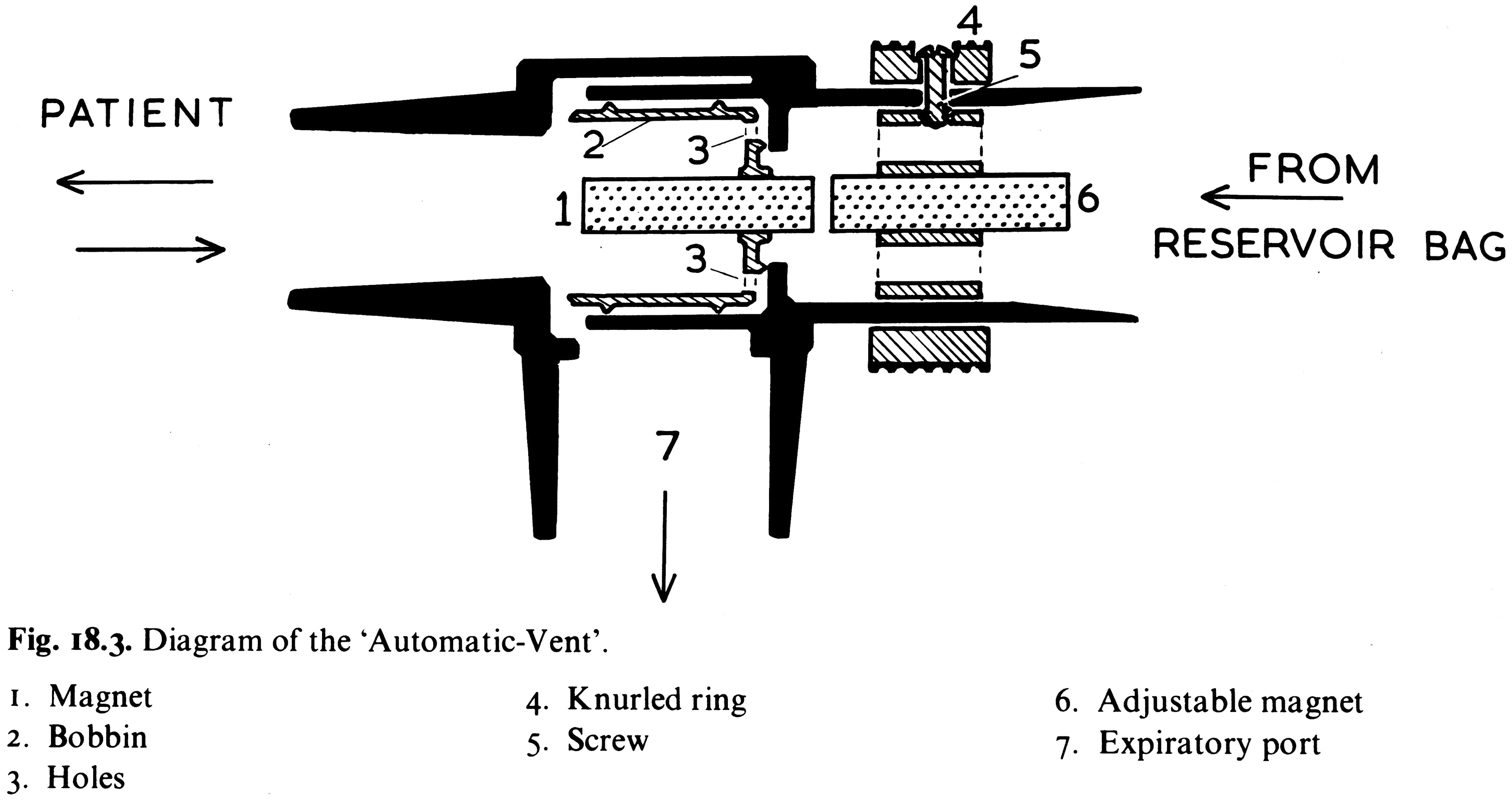
A diagram of the parts of the East–Freeman Automatic Vent from Automatic Ventilation of the Lungs 7 (courtesy of Blackwell Scientific Publications).
The East–Freeman Automatic Vent is set up by connecting a fresh gas supply, such as the common gas outlet of an anaesthesia machine, with a T-piece to a compliant 2 l rubber bag, like the ones on the circle system of an anaesthesia machine. This is connected to the inlet of the device. A bobbin is held closed by a magnet so that the bag fills and the patient’s airway is open to the exhale port. When the pressure in the bag is high enough the bobbin moves away from the magnet, closing off the exhale port and opening the inlet to the patient connector, inflating the patient’s lungs. As the flow decreases, the pressure falls enough for the magnet to cycle the valve back to the closed position.
The minute ventilation equals the fresh gas flow. A single control changes the position of one of the magnets to adjust the opening pressure initiating inspiration. This control ring allows limited change to the tidal volume, which is also influenced by the compliance of the reservoir bag. The respiratory rate is a function of the tidal volume and the minute ventilation. The operation and characteristics of the ventilator are well described in the excellent book by Mushin et al., 7 Automatic Ventilation of the Lungs.
The East–Freeman Automatic Vent originally cost £18.10.0d in 1969. 8
Mushin et al. also explain the similarity of the Automatic Vent to the Minivent described by Cohen 8 , 9 from Johannesburg, South Africa in 1966, and the Microvent by Carden 10 from Vancouver, Canada in 1969. Both of these were more complex with more moving parts requiring adjustment. Technical assessments and comparisons of these vents have been described elsewhere. 11 , 12
The Flomasta was described in 1977 by Jones and Hillard from Cardiff, Wales. 13 This design did not use a magnetically controlled valve, but was similar in many other respects. Forrest Bird also developed a series of ventilators using a magnetically actuated valve. These more sophisticated devices facilitated spontaneously initiated breaths as well as intermittent mandatory ventilation. 14 , 15
All of these designs appear to be derived from a pressure-operated inflating (POI) valve described by Mitchell and Epstein 16 in 1966 from Oxford, England, which they described as having been used successfully since 1956 at the Nuffield Department of Anaesthetics. It had a simple single moving part and required no adjustment. The POI valve was also manufactured by HG East and Co.
An antecedent ventilator was devised in Denmark during the polio epidemic in 1953 by Claus Bang. 17 Again, a rubber bag was in-line with the fresh gas flow. The flow to and from the patient was controlled by a piston non-rebreathing valve that was actuated electrically by a pair of solenoids. The power to these solenoids was controlled by the two limbs of a U-tube manometer monitoring the patient’s airway pressure. The manometer could be manipulated to change the peak inspiratory pressure, respiratory rate and inspiratory:expiratory ratio. The fresh gas flow determined the minute ventilation. An English version of Bang’s ventilator was described by Macrae et al. from Bristol in 1953. 18
There were several advantages of this group of non-rebreathing valve ventilators. They were compact and portable. They were powered by the gas supply from the anaesthesia machine or other driving source with reducing valve and flow meter, so no electrical supply was required. The flow meter allowed accurate setting of minute ventilation and the audible clicking of the valve gave an indication of the respiratory rate and continuing correct functioning. They were simple, rugged and easily dismantled for cleaning, and could be mounted on an anaesthesia machine for transporting anaesthetised patients. 19
Why are they no longer in use?
While they freed up the hands of the anaesthetist they required constant vigilance. The main problem was that they could stick in the inspiratory phase due to coughing, damage to the device or presence of secretions. 20 This led to sustained high pressure in the lungs requiring prompt disconnection from the patient to prevent barotrauma. They had provided an alternative to hand bagging but were superseded as the more complex and sophisticated ventilators became safer and more widely available. These simple designs are useful reminders of the many issues relevant to developing new ventilators during the current coronavirus pandemic.
Footnotes
Acknowledgements
Dr David Wilkinson, Dr Elizabeth Mackson.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.