
Abstract
The insertion depth of the left-sided double-lumen tube needs careful positioning and bronchoscopic confirmation. Several formulae based on body height have been used for estimating the optimal insertion depth of a left-sided double-lumen tube. We conducted this prospective study to test the hypothesis that our earlier developed height-based formula (0.25 × body height0.916) could predict the accurate insertion depth of a left-sided double-lumen tube. After obtaining ethical approval, 66 patients who underwent thoracic surgery were included. A left-sided double-lumen tube was advanced blindly to the predicted depth of insertion calculated using our formula. The optimal position of the left-sided double-lumen tube was confirmed using a fibreoptic bronchoscope. The primary outcome was the percentage of tubes placed in the optimal position without the need for further adjustments. The secondary outcomes included the need for bronchoscopic adjustments and the final correct insertion depth of the left-sided double-lumen tube. The formula resulted in an optimum position of the left-sided double-lumen tube without further adjustments in 45 patients (70%) (95% confidence interval 58%–80%). The left-sided double-lumen tube was withdrawn or advanced in 18.2% and 12.1%, respectively, to achieve the optimal insertion depth. We found that our formula provided satisfactory positioning in about 70% of patients and that in the remaining patients, the adjustments required to achieve satisfactory positioning under fibreoptic bronchoscope guidance were minimal. Nevertheless, as it is not possible to predict which patients will have a satisfactory tube position, bronchoscopic confirmation for the final positioning is still required.
Introduction
Accurate placement of a left-sided double-lumen tube (LDLT) is essential for effective one-lung ventilation in thoracic surgery. Optimal insertion depth of LDLT, defined as the endobronchial cuff placed just below the carina would decrease the incidence of obstructing the trachea and the contralateral bronchus. Additionally, too deep an insertion of the bronchial cuff of the tube would obstruct the upper lobe bronchus. 1 Careful adjustment of the insertion depth and optimal positioning of the LDLT typically requires a fibreoptic bronchoscope (FOB). 2
Several methods have been described to predict the correct insertion depth of LDLT. Chow et al. developed a formula based on the clavicular-to-carinal distance of the trachea and the body height in 78% of their patients. 3 Brodsky et al. demonstrated that a height-and-gender-based formula could predict the insertion depth of LDLT. 4 Liu et al. reported an accurate insertion depth of LDLT in 90% of their patients by measuring the distance between the vocal cords and carina according to chest computed tomography (CT). 5
In a pilot study, we have developed a formula for predicting the accurate insertion depth of LDLT into the left main bronchus based on the body height (BH) as follows: (0.25 × (BH)0.916). 6 We previously compared our formula with five other height-based formulae to predict the optimum insertion depth of the LDLT.3,4,6–8 Our formula correlated well with these formulae (Chow et al., 3 r = 0.71, P < 0.0001; Brodsky et al., 4 r = 0.75, P < 0.0001; Bahk and Oh 7 r = 0.74, P < 0.0001; Takita et al., 8 r = 0.65, P < 0.0001; Lin and Cherng 9 r = 0.72, P < 0.0001). Chow et al. reported that their formula, based on the clavicular-carinal distance of the trachea and patient’s height, provided an acceptable position of the LDLT without further adjustment in 78% of the patients. 3
We hypothesised that our formula 6 would predict the accurate insertion depth of LDLT at least as accurately as Chow et al.’s formula. We aimed to investigate the efficacy of this formula to predict the correct insertion depth of the LDLT, which we confirmed by FOB.
Materials and methods
After local ethical committee approval (Institutional Review Board, Health Sciences Colleges Research on Human Subjects, College of Medicine, King Saud University, Riyadh, Saudi Arabia, E-18-3064/IRB on 6 May 2018) and registration on www.clinicaltrials.gov (NCT04329416), informed written consent was obtained from patients included in this prospective observational single-centre study. Included patients were aged older than 18 years who underwent thoracic surgery using a LDLT (Mallinckrodt Endobronchial Tube; Medtronics, Minneapolis, MN, USA) for one-lung ventilation. Excluded patients were those with anticipated or known difficult airway.
Intraoperative monitoring and anaesthesia techniques were left to the discretion of the anaesthesiologists according to the local protocol. The LDLT size was selected according to sex: 35–37 Fr and 37–39 Fr for female and male patients respectively. The predicted insertion depth of the tube was calculated using the formula (0.25 × BH0.916) (degree of accuracy r = 0.75) before induction of anaesthesia. 6 We used an application (app) saved on a smartphone to perform the calculation of the LDLT’s depth of insertion. An Android app was developed using Java to incorporate the tube calculation process into an easy intuitive interface. After the user installs the application, they are presented with the calculator where they enter the height of the patient. This is then fed as an input to the formula to produce the insertion depth of the tube in centimetres. In this study we calculated the insertion depth of LDLT using a free Android app using this link on the Play Store: https://play.google.com/store/apps/details?id=com.ldlt.ldltCalculator.
The LDLT was introduced beyond the vocal cords when the train-of-four stimulation of the ulnar nerve revealed one or two twitches, the stylet was removed, the tube was rotated 90° anticlockwise then advanced blindly to the predicted depth of insertion. The optimal position of the tube, defined as the inflated endobronchial cuff in the left main bronchus just below the carina without herniation, was confirmed using FOB in both the supine and lateral decubitus positions. If the endobronchial cuff was placed too distal or too proximal, the tube was withdrawn or advanced, respectively, under FOB guidance until the optimal position of the tube was achieved. After optimising the position of the tube with the patient in the supine position, the ‘final correct depth of insertion’ (defined as the external centimetre marking of the tube that corresponded to the distance from the distal opening of the bronchial lumen to the outer lip of the corner of the mouth) was measured. Caution was exercised to maintain the patient’s head and neck in a neutral position in both the supine and lateral decubitus positions. The same experienced thoracic anaesthesiologist (>1000 thoracic cases) inserted and confirmed the optimal position of the LDLT. The primary outcome was the percentage of tubes placed in the optimal position without need for further adjustments. The secondary outcome included the need for bronchoscopic adjustments and the final correct insertion depth of LDLT.
Statistical analysis
Data were tested for normality by visual inspection of histograms. Data were expressed as means (standard deviation, SD), number (percentage) or median (interquartile range). Analyses were performed using the IBM SPSS Statistics (BM SPSS Statistics Subscription, Base Edition) programme (IBM Ireland Product Distribution Limited, IBM House, Dublin, Ireland).
Results
In total, 66 patients completed the study; the mean (SD) age was 47.1 (16.03) years and height was 165.3 (11.81) cm, and the median (range) weight was 70 (60–80) kg. All tubes were placed into the left main bronchus. Overall, 61% were male. The tube positioning data are presented in Table 1.
LDLT intubation data.
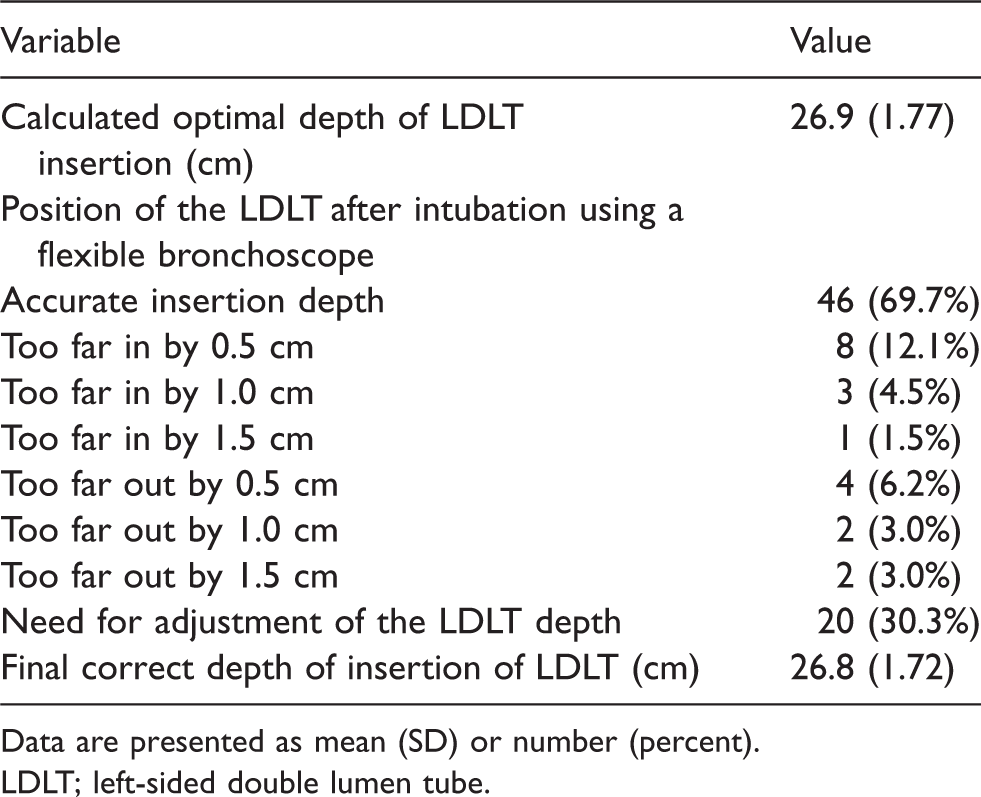
Data are presented as mean (SD) or number (percent).
LDLT; left-sided double lumen tube.
The use of our formula to calculate the predicted insertion depth of LDLT resulted in the optimal position of the tube without further adjustments in 46 of 66 patients (70%). The LDLT was withdrawn or advanced in 12 patients (18.2%) and eight patients (12.1%) respectively, until the optimal position of the tube was achieved (Table 1). In all patients, FOB checks revealed no tracheal or left upper lobe bronchus obstruction by the endobronchial cuff secondary to either too proximal or distal displacement of the tube.
Discussion
Using our novel formula 6 to calculate the optimal insertion depth of the LDLT resulted in optimal position without further adjustments in 70% (95% confidence interval: 58%–80%) of our patients. This was confirmed using FOB. The remainder required withdrawal or advancement in 18% and 12% respectively of patients to achieve optimal position. Most required only 0.5–1 cm adjustment for optimal positioning and none had a compromised airway due to obstruction of a bronchus or a lobe by a cuff. Nevertheless, as we were not able to predict which patients would require an adjustment of tube placement, our findings reinforce the necessity of using an FOB to check and adjust the correct insertion depth of LDLTs. If an FOB is not available, clinical methods are required to ensure there are no bronchial obstructions when tube cuffs are inflated.
Our previous pilot study showed that our formula 6 was well correlated to previously established formulae. 3 , 4 ,7–9 Of note, for patients who were 160, 170 and 180 cm tall, the model of Brodsky et al. 4 predicts the optimum depth of placement of 28, 29 and 30 cm respectively. In contrast, our model predicts 26, 27.5 and 29 cm respectively. Similarly, Lin and Cherng 9 demonstrated a large deviation between the correct insertion depth and the estimated insertion depth in both taller and shorter patients using Brodsky et al.’s 4 formula. The Chow et al. formula was based on the clavicular-carinal distance of the trachea and patient’s height. It provided an acceptable position of the LDLT without further adjustment in 78% of patients. 3 Our formula was based on the patient’s height only and provided an acceptable position of the LDLT in about 70% of patients; in the remaining 30% of patients, the adjustments required to achieve satisfactory positioning under FOB guidance were minimal. The hypothesis that our formula 6 would predict the accurate insertion depth of LDLT at least as accurately as Chow et al.’s formula was not achieved. However, our formula may still have merit, because it still had a high success rate (70%), did not require much adjustment in the remaining 30% of patients and it could be derived using a calculator based on the patient height alone, in contrast to Chow et al.’s formula that requires calculations based on measurements from chest X-rays as well as height. The calculation of our formula can be performed on most calculators, including those on a smartphone, but also on a free Android app.
Our formula has a higher rate for the acceptable position of the LDLT than the height-based formula developed by Takita et al. 8 (70% versus 62.3%). Unsurprisingly, our height-based formula was less accurate for predicting the accurate depth of LDLT than the radiological-based formulae by Chow et al. 3 and Liu et al. 5 (70% versus 78% and 90%, respectively). There are at least three other published formulae that predict the insertion depth of LDLTs. However, the authors of these formulae indicated they should be used as a guide and not to determine the final insertion depth of LDLT. 5
The LDLT is commonly used for thoracic surgical procedures, with typically less than 1% incidence of major complications (mainly from improper selection of the tube size). 10 However, LDLTs can be associated with malposition and dislodgement, which are influenced by multiple factors, among them the insertion depth. Currently there is no method to predict the optimal depth of LDLT insertion in all cases. However, some prediction methods may be more accurate than others, thereby reducing the number of tube placements that require adjustment or the amount of adjustment required once a check with an FOB is performed. 11 We propose that our formula based on height alone could be used as an initial default with the caveat that confirmation of correct and final positioning of the tube is still required using FOB.
This study has several limitations. First, it was not possible to blind investigators to the technique. Second, our formula may not be applicable to LDLT other than Mallinckrodt’s. Third, the study was registered retrospectively, although the protocol was already published prior to the start of recruiting. 6
In conclusion, our height-based formula (0.25 × BH0.916) could be used as an initial default to guide the initial insertion depth of LDLT. We found that it provided satisfactory positioning in about 70% of patients and that in the remaining patients the adjustments required to achieve satisfactory positioning under FOB guidance were minimal. Nevertheless, as it is not possible to predict which patients will have a satisfactory tube position, bronchoscopic confirmation for the final positioning is still required. Further studies are also required to validate the accuracy of our formula in other settings.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X20946051 - Supplemental material for Efficacy of height-based formula to predict insertion depth of left-sided double lumen tube: A prospective observational study
Supplemental material, sj-pdf-1-aic-10.1177_0310057X20946051 for Efficacy of height-based formula to predict insertion depth of left-sided double lumen tube: A prospective observational study by Abdelazeem A Eldawlatly, Mohamed R El Tahan, Naveed U Kanchi, Ahmad Al Qatari and Abdulaziz E Ahmad in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
We thank the College of Medicine Research Centre and Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia. We would also like to thank Mr Mahmoud Abdelazim Ali El-Dawlatly (MSc in Artificial Intelligence) for developing the android application of our formula.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.