
Abstract
An integrative review of the literature specific to leadership within the intensive care unit was planned to guide future research. Four databases were searched. Study selection was based on predetermined inclusion and exclusion criteria and a quality check was done. Data extraction and synthesis involved developing a preliminary thematic coding framework based on a sample of papers. The coding framework and all selected papers were entered into NVivo software. All papers were then coded to the previously identified themes. Themes were summarised and presented with illustrative quotes highlighting key findings. In total, 1102 relevant quotations were coded across the 28 included papers. Four themes pertaining to leadership were described and analysed: (a) leadership dimensions and discourses; (b) leadership experiences; (c) facilitators and/or barriers to leadership; and (d) leadership outcomes. The literature was found to focus on leader behaviours, as well as the leader dimensions of role allocation, clinical and communication skills and traditional hierarchies. Positive behaviours mentioned included good decision-making, staying calm under pressure and being approachable. Leadership experiences (and outcomes) are typically reported to be positive. Personal individual factors seem the biggest enablers and barriers to leadership within the intensive care unit. Training is considered to be a facilitator of leadership within the intensive care unit. This study highlights the current literature on leadership in intensive care medicine and provides a basis for future research on interventions to improve leadership in the intensive care unit.
Keywords
Introduction
There has been increased interest in leadership in healthcare over recent years.1–3 It is clear that effective leadership is important in optimising team performance in healthcare. 3 Within the most complex and intense clinical environments, such as intensive care units (ICUs), effective team leadership (as distinct from organisational leadership) may provide improved performance and patient outcomes. 3 Previous research has explored the barriers to leadership that can negatively impact on performance in healthcare teams. 4 It has also been suggested that leadership in ICU improves performance, but there are limited data on leadership within intensive care teams.5–7
Leadership is seen to be distributed across many professions and levels of healthcare. 1 One way to understand leadership is to consider the different ways in which it is conceptualised. Gordon and colleagues have described four discourses of leadership (i.e. particular ways of talking and thinking about it) within the context of medicine: individualist; relational; contextual; and complexity discourses. 1 An individualist discourse defines leadership through descriptions of individual actions, styles and responsibilities. A relational discourse looks at the leader-follower relationship and may be transactional (based on exchanges between them) or transformational (based on the leader’s abilities to inspire action). A contextual discourse can describe how different individuals demonstrate leadership appropriate to their position, where context determines how they behave. Finally, a complexity discourse may discuss an emergent process of leadership occurring within an adaptive system, where leadership can be distributed across different levels of an organisation and can represent a complex interplay amongst individuals and contexts. 1
Medical leadership can also be conceptualised as having different dimensions of leadership, including allocated roles, styles and behaviours. Note that we define dimensions as akin to the themes of leadership conceptualisations. 1 Leadership behavioural descriptors include delegating, making clear decisions and setting an example. 1 However, the ICU workplace is different to other areas of healthcare and as such, the dimensions and discourses may differ. The ICU is an environment of unwell patients and multidisciplinary teams including doctors and nurses; also many ICUs have rapid response teams (RRTs) who attend deteriorating patients in other parts of the hospital. Team training within this specific environment has been shown to improve skills. 8
Leadership is often described in the medical education literature as developed behaviour, and is therefore perceived as being learned. 1 Medical councils have even set leadership competencies for trainees to meet.9,10 However, a recent systematic review failed to find a substantial impact of current leadership training on physician behaviours. 11 Furthermore, leadership within intensive care medicine has been acknowledged for the first time in Fellowship training (in Australia and New Zealand), where the College of Intensive Care Medicine has included leadership competencies in the Fellowship training guide. 12 However, no published data or framework exist to guide this training.
This research therefore is aimed at discovering what is known about leadership within the ICU (based on medical and nursing literature). Specifically, the four research questions (RQ) were:
RQ1: What are the understandings of leadership in ICUs from the research literature? RQ2: What are ICU team members’ experiences of leadership? RQ3: What are ICU team members’ perceptions of the facilitators and barriers to leadership in the ICU? RQ4: What are the outcomes of leadership in the ICU?
This knowledge should help guide the development of future educational frameworks for leadership development within the ICU.
Methods
Searching for studies
Published peer-reviewed papers that explored leadership in intensive care or critical care teams were included in this review. Four databases (Ovid Medline, PsycINFO, Embase and Scopus) were searched in November 2017 for a combination of keywords: ‘leadership’, ‘team leadership’, ‘leadership qualities’, ‘leadership style’, ‘leadership behaviour’, ‘dynamic leadership’ OR ‘distributed leadership’ AND ‘intensive care units’, ‘ICU’, ‘critical care’, ‘critical care teams’, ‘resuscitation teams’, ‘code blue’, ‘medical emergency teams’ OR ‘MET teams’.
Study selection and appraisal
Endnote was used for the collation of search results and the removal of duplicates. Review of all abstracts from the above search was done by the primary author (DB) using Covidence software (Veritas Health Innovation Ltd, Melbourne, Victoria) for inclusion into a full-text review as per the inclusion and exclusion criteria (see Table 1). Review of a random sample of 10% of the total abstracts was done by a second author for quality assurance (WB).
Inclusion and exclusion criteria.
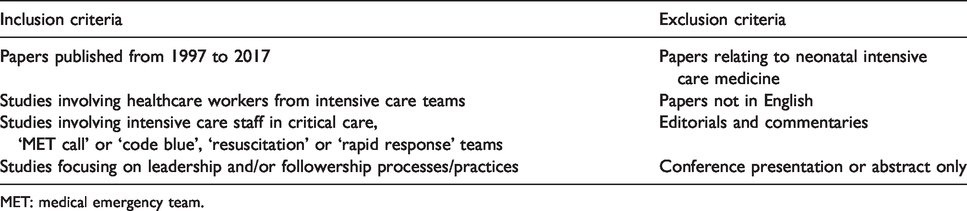
MET: medical emergency team.
All included studies were then divided between authors for full-text review, with the primary author (DB) reading all included studies and the other authors (CR, LG and WB) each reading a sample of at least 20% of the total number of studies. Relevant papers were limited to those published in English from 1997 to 2017, involving staff from ICUs (or intensive care staff in medical emergency teams) focusing on leadership approaches and outcomes and/or barriers and/or facilitators to leadership.
Following full-text review, all included papers were checked for quality by three authors (DB, CR and LG) using the Medical Education Research Quality Instrument for quantitative studies and Critical Appraisal Skills Programme tools for qualitative and mixed methods studies.13,14 All papers of low or medium quality were excluded. This resulted in a final sample of papers for this review. An integrative review was chosen given the mix of qualitative and quantitative studies. 15 It aimed to summarise and synthetise this methodologically mixed published research to create an understanding of leadership in the ICU. 15
Data extraction
Descriptions of the study characteristics were tabulated, enabling comparisons to be made of study designs and data collection methods, participants, country of origin and research questions. A preliminary thematic analysis of 20% of the final selection was done by three authors (DB, LG and CR) to develop a coding framework (see Appendix 1.) This framework was developed partly from the new data and partly by drawing on previous medical leadership literature. 1 The broad themes in the coding framework set out to answer the four original research questions. The coding framework and all included papers were entered into NVivo software version 12 (QSR International Pty Ltd., Chadstone, Victoria, Version 12, 2018). Firstly, a sample of 10% of papers were coded by two authors for quality assurance (DB and CR). All papers were then coded by DB using NVivo.
Data synthesis
All coded papers in NVivo were then subjected to analysis that was conducted to explore patterns in the coding. NVivo provides counts of the number of quotations coded to each theme/sub-theme, so it was first possible to identify the dominance of certain themes/sub-themes across the whole dataset, plus identify the dominance of themes by certain types of papers. For example, after exploring the co-occurrence of themes, matrix coding queries were used to explore the intersection between coded quotations for themes/sub-themes and different ICU settings (adult ICU, paediatric ICU (PICU) and RRTs), participant cohorts (medical, nursing or mixed) and publication year (2010 onwards versus pre-2010). Key themes were identified through continuous examination and probing of the data. Themes were summarised and presented in narrative form with illustrative quotes used to highlight key findings. This follows the classic methods for an integrative review. 15
Results
The literature search results, including quality checks, are summarised in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram (see Figure 1). The final 28 papers are tabulated (see Table 2). Of the 28 papers, the majority were quantitative (n = 16), with fewer qualitative (n = 10) or mixed-methods studies (n = 2). The methods used in the papers were (in decreasing order of frequency): questionnaires (n = 11), interviews (n = 10), observer scale through video analysis (n = 4), direct observation scale (n = 2), observer scale through audio analysis (n = 2) and focus groups (n = 2). The papers typically originated from the United States of America (n = 13), with fewer papers from the United Kingdom/Europe (n = 7), Canada (n = 3), Australia/New Zealand (n = 2), Jordan (n = 1), Singapore (n = 1) and South Africa (n = 1). The papers were primarily based in adult ICU (n = 18) or adult RRT (n = 4) settings, with fewer papers based in PICU (n = 5) or paediatric RRT settings (n = 1). Finally, participants in the studies included both doctors and nurses (n = 13), with fewer studies focusing on nursing participants only (n = 9) or medicine only (n = 6). Participant group sizes ranged from six to 518 across the 28 studies.
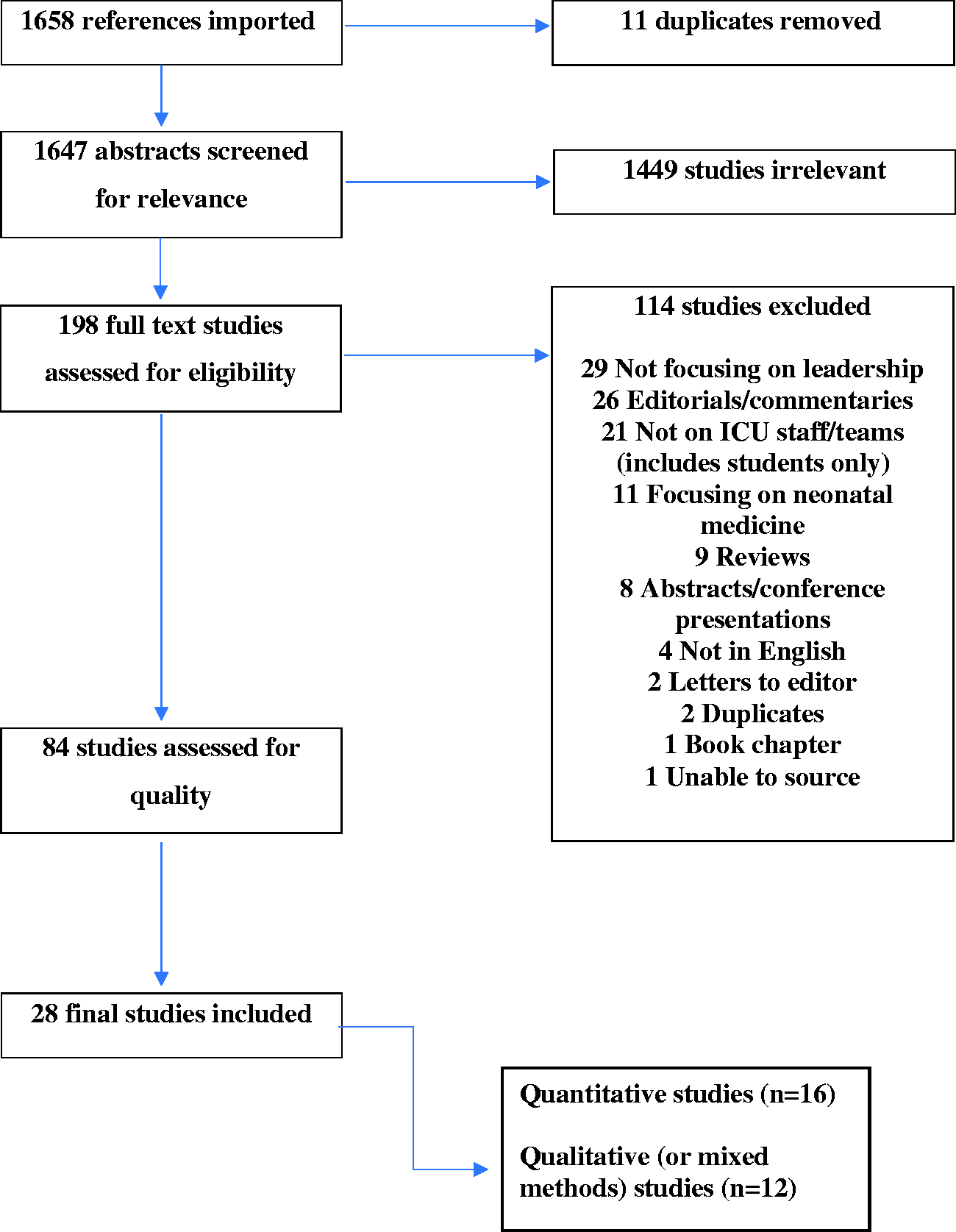
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram. ICU: intensive care unit.
Summary of included studies.
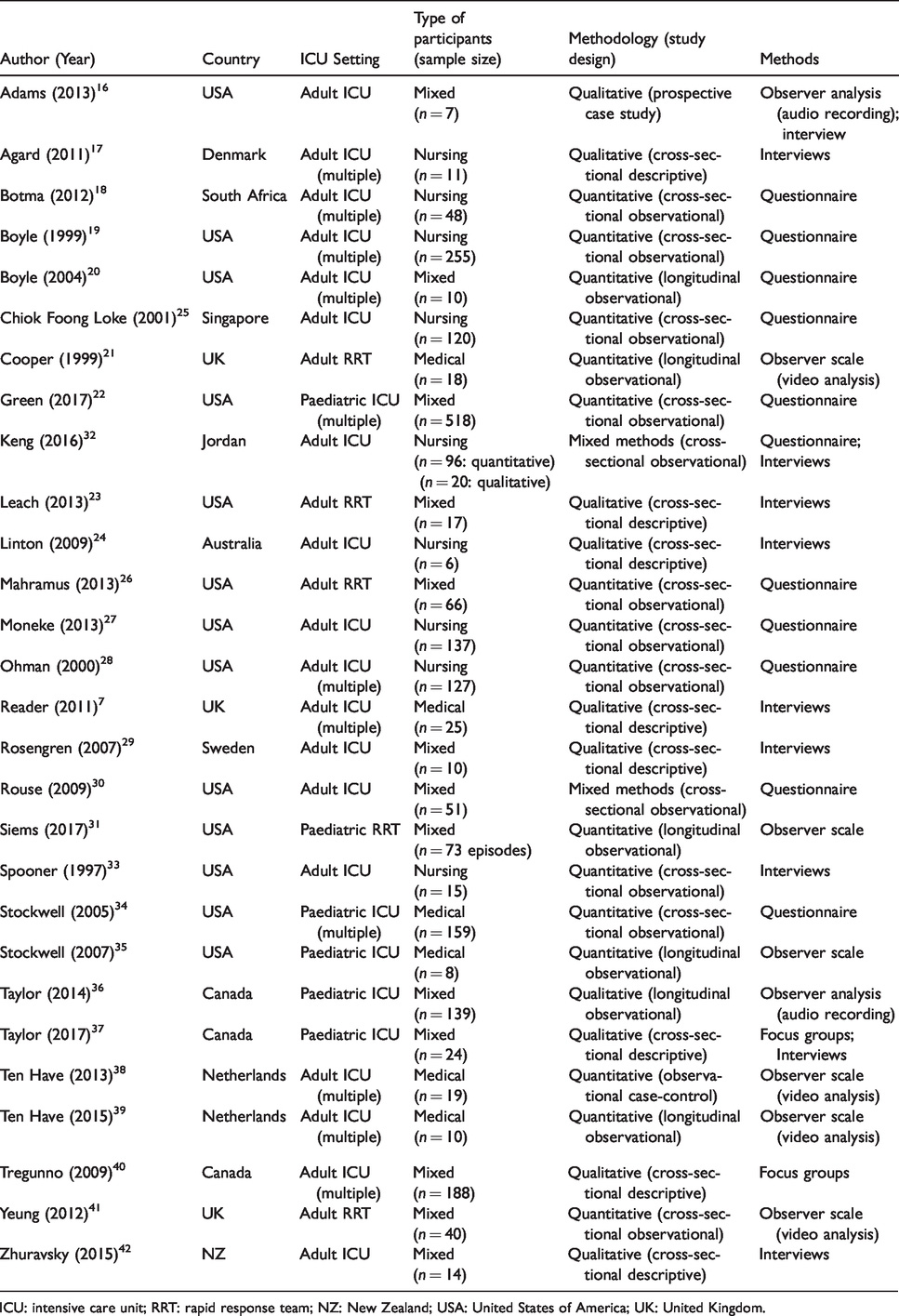
ICU: intensive care unit; RRT: rapid response team; NZ: New Zealand; USA: United States of America; UK: United Kingdom.
Results of the higher-level coding framework illustrating themes/sub-themes can be seen in Appendix 1. A total of 123 distinct codes were developed across all the sub-themes (a copy of the full coding framework can be requested from the corresponding author).
Theme one: Understanding leadership within the ICU
Leadership dimensions were identified in all but one paper, accounting for more than half of the coded references (571 of 1102). As Table 3 illustrates, leadership was most commonly conceptualised as the sub-themes ‘behaviour’, ‘profession’, ‘skills’ including clinical and/or communication, ‘management’ or ‘style’. The most commonly identified dimension was behaviour and included decision-making, calmness under pressure and being respectful.
Common leadership dimensions and discourses with illustrative quotes.
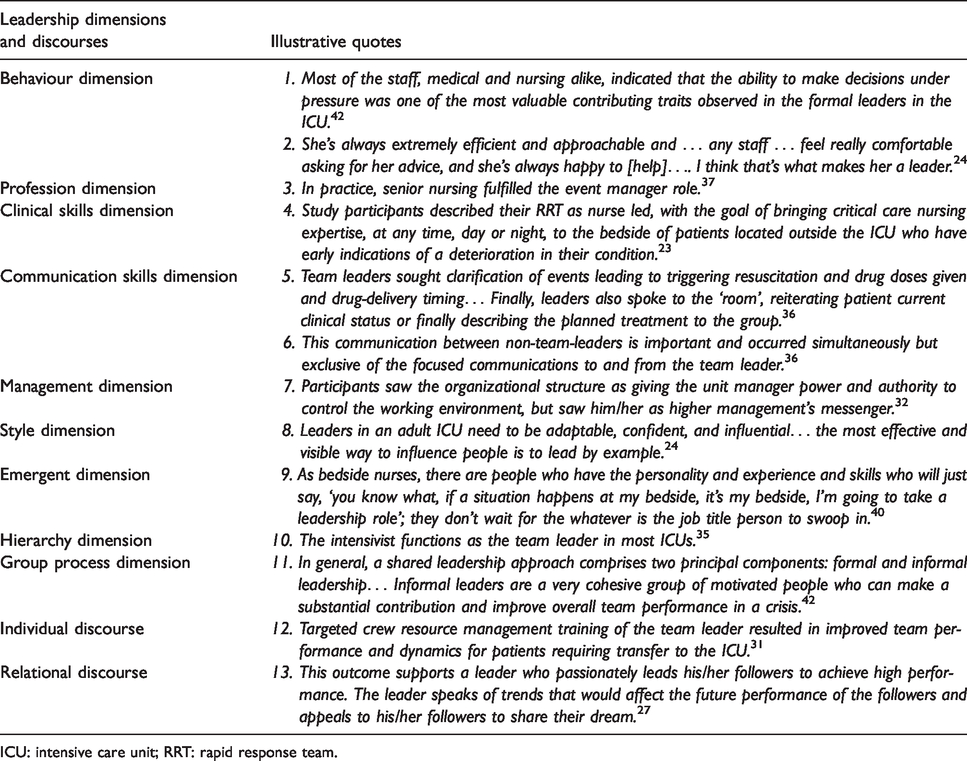
ICU: intensive care unit; RRT: rapid response team.
We noticed a variety of patterns in our data across this leadership dimension theme. For example, although medical leaders were most commonly described as the ‘decision makers’, and thus those needing to remain calm in a crisis (see quote 1, Table 3), nursing leaders were also often described as being sought out to lead by other staff (see quote 2, Table 3). Indeed, nurses were more often described as leaders not through assigned leadership roles, but instead as being approachable and clinically expert (see quote 2, Table 3). This emergence of leadership, identified in only 25% of papers, was mostly described in studies involving mixed participants (i.e. both doctors and nurses) but was seen across all settings (i.e. adult/paediatric ICUs and RRTs).
From the coded literature, the ICU workplace (and that of the RRT especially) required team communication, with communication skills being portrayed as a key dimension for leaders and followers (see quotes 5 and 6, Table 3). Conceptualisations of leadership as both traditional hierarchy and emergent shared leadership through group processes were also seen across the papers (see quotes 9 and 10, Table 3). Although leadership as hierarchy was almost specific to papers on medical and mixed cohorts (i.e. not studies with only nursing participants), understandings of leadership as a shared group process were entirely found in studies including nursing professions (see quote 11, Table 3). Conceptualisations of leadership as a shared group process seemed most evident in crisis situations and emergency team performance (such as the RRT).
Leadership discourses were identified in most of the 28 papers, with the individual discourse central in mixed and medical papers, as well as more recently published papers (from 2010 onwards). Although the individual discourse seemed evident across papers involving all ICU settings, it seemed particularly prevailing in papers discussing leadership of RRTs, both in clinical practice and training.
However, leadership as a relational discourse seemed more dominant in papers published before 2010, as well as those papers involving only nursing participants (see quote 13, Table 3). The relational discourse was almost exclusive to the adult ICU setting (as opposed to the paediatric ICU or RRT research). Interestingly, the relationship between nurse leaders and followers, especially ‘transformational leaders’, was more deeply explored than relationships involving medical staff.16,17 Leadership as complexity was identified less frequently but across all three settings and most dominant in the mixed participant research.
Theme two: Leadership experiences within the ICU
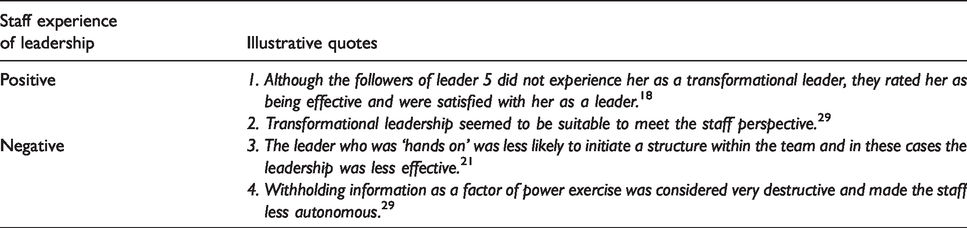
Leadership experiences in ICUs were described in about half of the papers with much less frequency than other themes. References to positive, neutral and negative experiences of leadership seemed to be evenly distributed across those papers (see quotes in Table 4). Research into nursing leadership demonstrated a higher dominance of positive leadership experiences reported than was illustrated from medical and mixed participant research. Leadership styles most commonly co-occurred with leadership experiences, both positive (see quotes 1 and 2, Table 4) and negative (see quotes 3 and 4, Table 4). Although not often coded, there seemed to be a link between transformational leadership styles and positive experiences (see quotes 1 and 2, Table 4).
Illustrative quotes for experiences of leadership specific to staff.
Theme three: Facilitators and barriers to leadership in the ICU
Facilitators and barriers to leadership within ICUs were widely identified across all 28 papers, accounting for 27% of all coding. Leadership within the ICU was reported to be facilitated at three distinct levels. Individual facilitators specific to leaders themselves were most dominant (compared with relational and organisational facilitators). The most frequently described individual leadership facilitators within the ICU were that of leader training and prior clinical and/or leadership experiences. Leadership training was commonly described in all settings and across all participants. Interestingly, training was often mentioned as a separate leadership facilitator to clinical skills (see quotes 1 and 2, Table 5). Prior experience as a leadership facilitator was most identified in the nursing literature (see quotes 3 and 4, Table 5). Inherent individual traits and abilities were often seen as facilitating good leadership, most commonly that of communication skills (see quote 5, Table 5). Barriers to leadership were also identified mostly at the individual level, with lack of confidence and poor communication the most frequently identified individual barriers to leadership (see quotes 6 and 7, Table 5). These barriers to leadership at the individual level were almost exclusively described in papers from the adult ICU setting and more commonly identified in the research involving mixed or nursing participants.
Illustrative quotes for leadership facilitators and barriers.
ICU: intensive care unit; PCCM: paediatric critical care medicine; RRT: rapid response team.
Theme four: Positive outcomes of leadership in the ICU
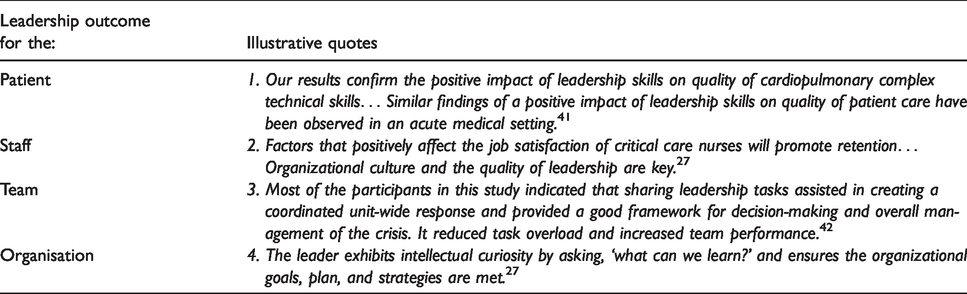
Outcomes of leadership within the ICU were identified in nearly all of the 28 papers and coded as outcomes at four levels: patient, individual, team and organisational (see quotes 1–4, Table 6). Nearly all (88.8%) of the coded leadership outcomes were positive. Positive outcomes for patients following good leadership within the ICU (such as improved resuscitation and patient safety) were predominantly seen in solely medical or mixed participant studies (see quote 1, Table 6), with nursing studies accounting for the majority of positive outcomes for staff (see quote 2, Table 6). Nursing papers illustrated strong links between leadership styles, especially relational styles, and positive staff outcomes such as clinician engagement, job satisfaction and intention to stay in the job (see quote 2, Table 6).
Illustrative quotes for outcomes of leadership at different levels.
Discussion
Summary and discussion of key findings
This review identified 28 studies of high quality relevant to leadership within the ICU. The majority were quantitative (57.1%), which reflects the typical scientific approach to research within the ICU. However, the included papers had diverse methods, suggesting an integrative review was optimal to analyse the data and suggest future directions for leadership research in the context of the ICU. 15 A coding framework was developed including four main themes aligned with the study research questions (leadership dimensions and discourses, experiences of leadership, facilitators and barriers to leadership, and leadership outcomes).
In terms of RQ1, we found that certain leadership dimensions (such as behaviour, profession, skills, management and style) dominated, as did individual and relational discourses. Leadership behaviours identified included good decision-making, staying calm under pressure and being approachable. First, we found that leadership behaviours and hierarchies were most often found in papers involving doctors, whereas leadership emergence and shared processes were typically found in papers involving nurses. Second, we found that individualist discourses dominated the literature post-2010, as well as studies with ICU staff from mixed professions, whereas relational discourses were more central in the pre-2010 literature and research involving nursing staff alone. This may be related to the rise of non-technical skills teaching, which advocates a very individualist way of thinking about leadership. Finally, the relational discourse was most commonly linked to positive outcomes for staff, which we believe was most likely identified due to variability in the study designs of the individual papers.
Surprisingly, we only identified experiences of leadership in half of the papers. Although this may be due to the study designs, their reporting methods and/or quality of articles, it perhaps represents a genuine gap in the literature. Most leadership experiences we identified were positive and predominantly seen in the nursing literature. The overwhelmingly positive nature of reported experiences may represent a publication bias, with literature reporting positive leadership experiences being more likely to be accepted for publication than literature reporting negative experiences of leadership. Furthermore, the notion of leadership by its nature has positive connotations and a heroic quality. 18
RQ3 led us to identify perceived facilitators to leadership within ICU, with most being found at the individual level such as leadership training, prior leadership or clinical experience and communication skills. Barriers identified to leadership were also identified mainly at the individual level, with lack of confidence the most commonly identified. These individual facilitators and barriers again followed the strong individualist discourse of leadership identified throughout the literature. 1 It is worth highlighting that communication skills were identified as both a key leadership dimension and facilitator to leadership in ICU. This is perhaps unsurprising given the extent to which ICU team members’ significant responsibilities rely on effective communication. 12 Leadership in the ICU can include clinical performance in stressful situations (such as resuscitation), end-of-life conversations between staff and patients’ families and the palliative care of complex patients. Leadership is also seen when leading a multi-disciplinary and interprofessional team in ICU that often involves numerous different practitioners from specialties outside the ICU.
Finally, we explored the outcomes of leadership in the ICU (RQ4) and found mostly positive outcomes of leadership, again possibly reflecting publication biases. The positive effects of ICU leadership on patients were most often linked to clinical (e.g. resuscitation) performance, but were not investigated in detail. Interestingly, we identified strong links between leadership and positive outcomes for staff, especially in the nursing literature. This finding may reflect the nursing literature, which may be more inclined to explore staff outcomes (such as job satisfaction and intention to stay) given that these are significant issues currently within critical care nursing worldwide.19,20 The finding that a relational leadership style may have a more positive effect on ICU staff (dominant in the nursing literature) needs further exploration.
Comparison of key findings with literature
Why should behaviours and hierarchies dominate the medical literature, but emergence and shared processes dominate the nursing literature? Why would individualist discourses be more contemporary than relational? We do not have any previous large literature reviews on leadership within the ICU with which to compare our results. However, our results support recently published works that identified a strong individual discourse when discussing leadership with medical trainees and a diverse range of leadership discourses within modern healthcare settings. 1 Our results also align with a recently published large review from the United Kingdom looking at leadership in the wider field of healthcare, which reports that both shared and individual leadership exists and that medical leadership behaviours vary significantly, as well as reporting positive outcomes at the staff level to nursing relational leadership styles. 3 The landscape of leadership within the ICU is, however, complex, with multiple examples of leadership possible concurrently. It is therefore possible that different approaches, be it individual and relational, may coexist depending on the staff (medical, nursing or mixed) involved in the context.
Strengths and limitations
Looking at the total sample of included papers, leadership is often discussed broadly and approached in an individualist fashion, which is consistent with the broader leadership literature in healthcare. We looked at studies from both medical and nursing participants (as well as mixed) that were published across four different continents, which makes the results more transferable to other contexts. Furthermore, our search strategy and coding processes were robust. Our study has some limitations, however, most notably the quality of published research on leadership within the ICU. However, we employed a quality check before inclusion to overcome this limitation, which we hoped would improve the credibility and translation of our results. Noteworthy for us was a distinct lack of published research on followership within the ICU. This should be seen as both a limitation of the overall current breadth of research on leadership within the ICU, as well as a key area to focus on with future research. Finally, the discourses we analysed were potentially the authors’ discourses and assumptions, with their participants’ responses heavily influenced by the authors’ questions.
Implications for further research
Our findings suggest future research should focus on the different leadership approaches within the ICU occurring during different clinical contexts. For example, individualist versus relational approaches should be explored further. Indeed, further exploration into the importance of relationships within intensive care teams, as well as situational contexts is needed to really explore leader-follower dynamics within the ICU. This could be done in a variety of contexts, such as leadership during daily ward rounds (and between nursing and medical leaders) and during advanced life support provision, as well as within adult and PICU settings. The emergence of leadership in more complex, interprofessional, team-oriented and high-stress clinical encounters (such as RRTs attending a cardiac arrest) should particularly be better understood. Future research should also explore ICU members’ experiences of leadership, which seems to be lacking in the literature. Additionally, the key facilitators of leadership in the ICU that we identified (training and communication) should be explored in further research, for both medical and nursing staff. Our study also highlights that there is significant opportunity to explore followership within the ICU. Finally, organisational and relational facilitators and barriers to leadership, which are poorly understood within the ICU literature, need further exploration.
Implications for educational practice
The educational framework and curriculum required to teach leadership in both medical and nursing training programmes within the ICU should be explored further. More specific research into the optimal communication and training of leadership within the ICU would enable the development of leadership education specific to the ICU. The appropriate training method, modality and frequency of training is unclear. We have shown that leadership is diverse within the world of intensive care, so the education underpinning its practice needs to avoid a one-size-fits-all approach. For example, programmes may need to facilitate learning from both a relational standpoint and an individualistic one. Education may be interprofessional to build on relational techniques, meaning that workplace-based, role-playing and/or simulation-based education may be required. There may also be a need to grow the broader ICU community’s understanding of leadership before leadership educational programmes can be effective.
Conclusions
Overall, we identified four themes relevant to leadership within the ICU. Leadership literature in the ICU focuses on leader behaviours, as well as other dimensions such as role allocation, clinical and communication skills and traditional hierarchies. Behaviours mentioned included good decision-making, staying calm under pressure and being approachable. A diversity of leadership discourses is present (mainly individual and relational) in the literature of both different health professions and different ICU settings. Leadership experiences within the ICU (and outcomes) are typically reported to be positive in the literature reviewed, especially in the context of nursing staff. Individual factors seem the biggest enablers and barriers to leadership within ICU. Training is widely considered to be a strong facilitator of leadership within the ICU, as are communication skills.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X20937319 - Supplemental material for Leadership in intensive care: A review
Supplemental material, sj-pdf-1-aic-10.1177_0310057X20937319 for Leadership in intensive care: A review by David J Brewster, Warwick W Butt, Lisi J Gordon and Charlotte E Rees in Anaesthesia and Intensive Care
Footnotes
Author contributions
All authors were substantially involved in the study design, acquisition and analysis of data, drafting and revising of the article and final approval of the version.
Acknowledgements
The authors would like to thank Diane Horrigan (Cabrini Institute Library, Melbourne) for search strategy support and Corinne Davis (Monash University, Melbourne) for NVivo support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.