
Abstract

Several variations in brachial plexus anatomy have been described.1,2 For example, since the popularisation of ultrasound-guided techniques, the musculocutaneous nerve (MCN) has been observed to exhibit variability in position, shape and echogenicity in the axillary fossa, differing from anatomical textbook descriptions.3,4 This may pose technical challenges, especially for those less experienced with axillary blocks, with the possibility of misidentification of the MCN and MCN block failure. We analysed a case series of ultrasound-guided axillary plexus blocks in order to investigate the characteristics of the MCN at this anatomical location.
This study was approved by the Macquarie University Human Research Ethics Committee (HREC/5201825912964). C.J. performed 162 ultrasound-guided axillary brachial plexus blocks on patients >18 years of age admitted for distal upper arm elective surgery between June 2015 and June 2017. A standardised imaging plane at the level of the anterior axillary fold and deltopectoral groove was used in order to report the location of the MCN at a reproducible fascial plane. When the MCN was not observed at this plane, dynamic imaging was used proximally and distally, as would be the case in routine clinical practice, to confirm its absence. Scans from this plane were saved and analysed by A.C. and A.S. The position of the MCN was recorded using a semicircular template divided into six equal segments of 30° each, from anterior to posterior, relative to the axillary artery (Figure 1). The nerve cross sectional area (mm2) was measured using the calibrated, electronic calliper software tool. The MCN shape was categorised as oval, flat-oval, round or triangular.
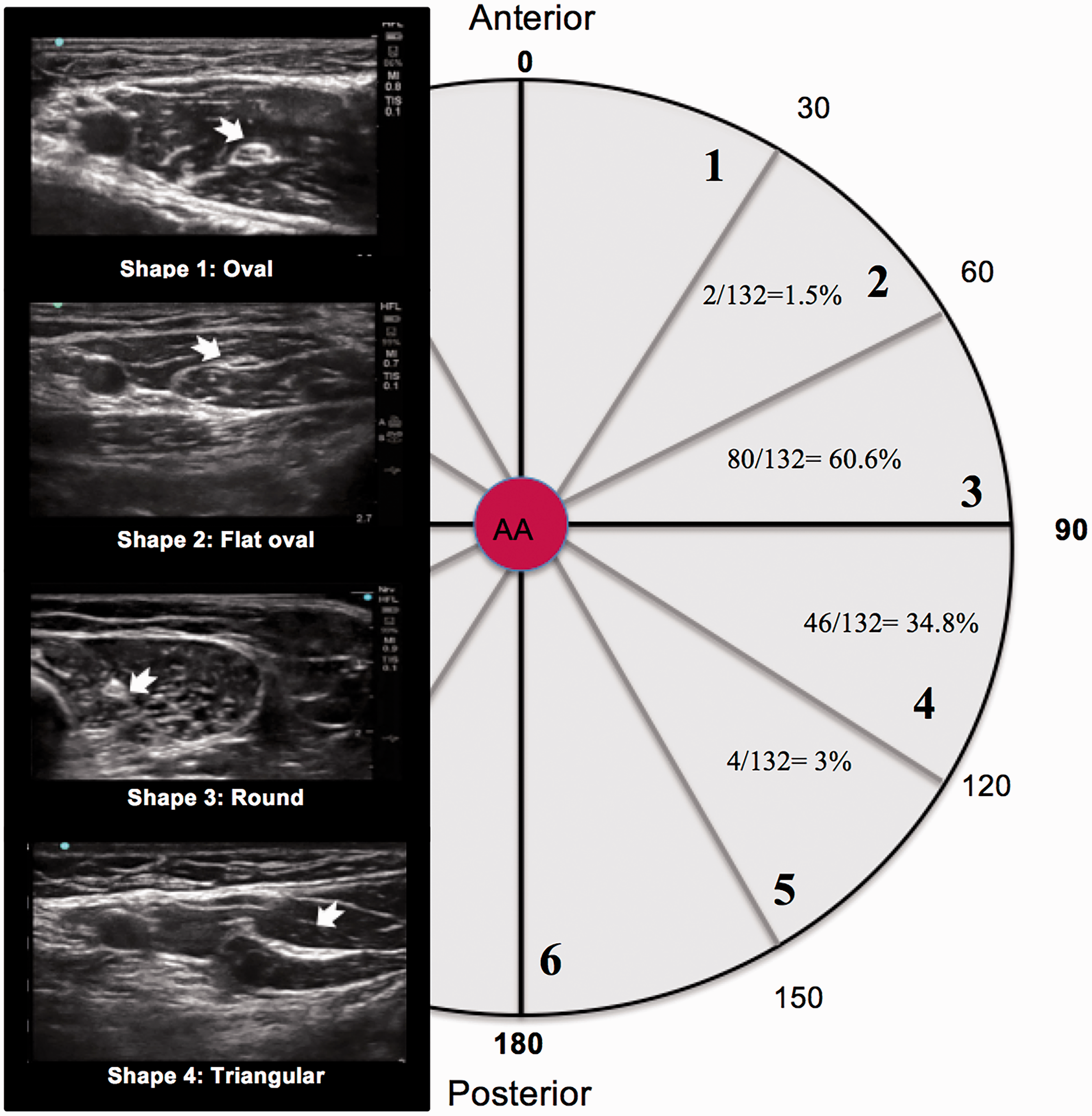
Location template centred on the axillary artery, and shape patterns found at the imaging plane between the anterior axillary fold and deltopectoral groove. The template has been divided into six segments of 30° each.
The MCN was visualised in 132/162 (81.5%) images, with characteristic honeycomb internal structure and hypoechoic fascicles. The MCN was located between segments two and five on the semicircular template, with the majority (95.4%) located in segments three and four (Figure 1 and Table 1). The most common shapes of the MCN were flat-oval and oval (total 87.1%). The median cross sectional area was 5 mm2 (interquartile range 3–6 mm2).
Shape of musculocutaneous nerve and its location relative to the axillary artery.
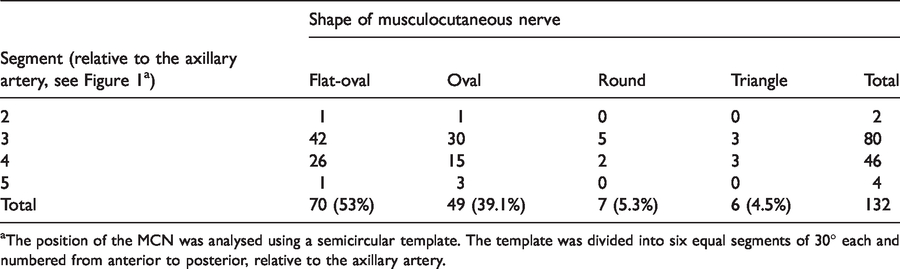
aThe position of the MCN was analysed using a semicircular template. The template was divided into six equal segments of 30° each and numbered from anterior to posterior, relative to the axillary artery.
Overall, the MCN was visualised in the majority of cases and located within a 120° arc lateral to the axillary artery, with the most common shapes being flat-oval or oval. These patterns may assist clinicians in identifying the MCN and potentially aid in the efficacy and safety of blocks.
These results were obtained at the anterior axillary fold, which was chosen as the typical imaging plane when performing ultrasound-guided axillary plexus blocks. For cases when the MCN was not seen at this location, dynamic imaging was used to confirm its absence and accounted for 30 (20%) cases. This may indicate an absent MCN, 4 or fusion of the MCN with other brachial plexus nerves such as the median nerve. 5 In the latter case, we found that a trace back manoeuvre from the anterior axillary fold towards the elbow may reveal the MCN branching off from a fused nerve more distally than anticipated.
This study demonstrated variability in both the shape and cross sectional area of the MCN at our standardised location. Previous studies have also reported that the shape of the MCN changes distally from the coracobrachialis to the elbow. 6 A limitation of our study is that we did not analyse the relationship between patient demographics (e.g. age, sex or weight) and the characteristics of the MCN.
No clinical outcomes were reported in regard to variation of the anatomy, as the study was strictly designed to investigate potential patterns relevant for regional anaesthesia.
In conclusion, we add further evidence demonstrating that traditional cadaveric descriptions of the MCN do not sufficiently describe the nuances of its shape and location. We provide relevant images of MCN variability so that patterns may be recognised when performing ultrasound-guided axillary plexus regional anaesthesia. Clinicians should be aware of such variability and modify their techniques to optimise efficacy and safety. The dynamic nature of ultrasound scanning should be used advantageously, particularly if neural structures at the traditional location for imaging are not immediately identifiable.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.