
Abstract
Summary
Grade V subarachnoid haemorrhage is associated with high mortality and morbidity, yet there are few contemporary reports on the treatment provided and outcomes of these patients. In this single-centre retrospective cohort study, we primarily sought to determine the 12-month mortality of patients admitted to the Royal Adelaide Hospital intensive care unit between 2006 and 2016 with grade V subarachnoid haemorrhage. Secondary objectives were to describe treatments provided, patient destination following hospital discharge, organ donation and hospital financial costs. Over the 11-year study period, there were 139 patients admitted with grade V subarachnoid haemorrhage. The annual number of admissions did not change over time. The median age was 56 (interquartile range 48–70) years, 88 (63%) were female and 77 (55%) had a procedure to isolate an aneurysm. There were 77 (55%) patients who died in the intensive care unit, 87 (63%) died in hospital and 89 (64%) had died at 12 months. Of the 52 patients who survived to hospital discharge, 33 (63%) were transferred to a rehabilitation facility, 17 (33%) to another acute care hospital and two (4%) were discharged. Of the 87 patients who died in hospital, 45 (52%) donated organs. The total hospital cost of managing this cohort was A$8.3 million, with a median cost of A$41,824 (interquartile range A$9,933–A$97,332) per patient. Grade V subarachnoid haemorrhage has a high mortality rate, with one-third of patients alive after one year.
Introduction
Spontaneous subarachnoid haemorrhage (SAH) is a potentially devastating condition, which can cause significant neurological injury and death. 1 The incidence rate of SAH is approximately 10 per 100,000-person years and typically affects middle-aged adults (45–65 years).2,3 Patients with SAH presenting with a Glasgow Coma Scale (GCS) score of six or lower are classified as having grade V haemorrhage as per the World Federation of Neurosurgical Societies. 4 Grade V haemorrhages account for 17%–35% of patients with SAH admitted to an intensive care unit (ICU) and are associated with the highest mortality and poorest functional recovery.5–11
Survival rates and functional outcomes following SAH have improved, which may represent advances in diagnostic modalities and treatment techniques (e.g. endovascular coiling).12–15 However, a limited number of studies have specifically assessed the outcomes of patients following grade V SAH. Cohort studies of patients with grade V SAH (managed since 2000) report that approximately half survive to hospital discharge and long-term ‘favourable’ outcomes occur in 9%–28%.6–8,16–18 An Australian and New Zealand ICU registry study of SAH reported that of 3861 patients with grade V haemorrhage, 40% survived to hospital discharge (compared to 88% hospital survival for all other grades of SAH), and highlighted the urgent need to further understand the treatment and outcomes of this group of patients. 5
Given the high mortality and morbidity associated with grade V SAH, its preponderance in a relatively young age group and limited data regarding critical care and outcomes, we undertook a retrospective cohort study of patients with grade V SAH. The primary objective was to determine survival one year after hospital presentation. Secondarily we sought to describe the treatments provided, hospital discharge destination, number of organ donors and hospital financial costs.
Materials and methods
Study design
We conducted a retrospective single-centre cohort study of patients admitted to the Royal Adelaide Hospital (RAH) ICU with grade V SAH. This study was approved by the RAH Human Research Ethics Committee (HREC/18/CALHN/229).
Study setting
The RAH is one of two tertiary neurosurgical referral centres serving South Australia’s population of 1.67 million, with approximately 80,000 hospital admissions, including 2100 ICU admissions and 1200 neurosurgical admissions annually.
Study cohort
The study cohort comprised patients admitted to the RAH ICU between 1 January 2006 and 31 December 2016 (11 years), with an admission diagnosis of SAH as identified by Acute Physiology And Chronic Health Evaluation IIIJ (APACHE-IIIJ) codes (402, 1503), a lowest GCS score of six or less in the first 24 hours (or just prior to commencing sedation) and aneurysmal aetiology. The diagnosis of aneurysmal SAH was confirmed retrospectively from event history, consultant radiologist reports of brain imaging and case review by a consultant neurosurgeon. The cohort was categorised into subgroups based on survival/mortality status 12 months after hospital admission.
Objectives
The primary objective was to determine the proportion of patients dying (in ICU, hospital and 12 months after ICU admission). Secondary objectives were to describe the treatments provided, destination following discharge from hospital, organ donation and hospital financial costs.
Data sources
Cases were identified from the RAH ICU dataset submitted to The Australian and New Zealand Intensive Care Society (ANZICS) Adult Patient Database (APD). 19 This dataset was used to determine patient age, gender, state of usual residence, indigenous status, GCS score, APACHE-IIIJ score (with and without GCS component), cardiac arrest prior to ICU admission, length of stay (ICU, hospital) and mortality (ICU, hospital). Collection of data was by ICU consultants until 2008 and thereafter by a single trained data collector. The collection of GCS scores followed ANZICS APD guidelines. Date of death following hospital discharge was extracted from the South Australia Registry of Births, Deaths and Marriages.
A neurosurgeon, blinded to patient outcomes, retrospectively reviewed computed tomography (CT) brain scans performed at hospital admission to allocate a modified Fisher Scale (mFS) grade. 20 The mFS grade describes the extent of subarachnoid blood on CT scan and is associated with an increased risk of vasospasm and poor outcome.7,20
Procedure data were obtained from hospital coding and crosschecked with the electronic medical record by a single investigator. These data elements included CT cerebral angiography (CTA), digital subtraction cerebral angiography (DSA), aneurysm treatment (clipping, coiling), neurosurgical procedures (external ventricular drain (EVD) insertion, decompressive craniectomy, ventriculoperitoneal shunt), tracheostomy and patient destination following hospital discharge (rehabilitation facility, another acute care hospital, home). Records of organ donation and transplantation were obtained from Donate Life SA. 21
Hospital financial costs for each patient were provided by the RAH Case Mix Unit. The Case Mix Unit calculates the costs of hospital admission (including investigations, operative procedures, ICU stay and hospital stay) based on data obtained from medical record coding. Costs were not adjusted for the year of admission and those incurred following hospital discharge were not included.
Data analysis
Categorical data are summarised as number (n, %). Continuous data are presented as mean (standard deviation, SD) or median (interquartile range, IQR), depending on their distribution. Between-group comparisons were performed by chi-squared, Fisher’s exact test, Student’s t-test or Wilcoxon rank-sum test as indicated. Survival times are presented as Kaplan–Meier curves. No imputation was undertaken for missing data. Deaths outside of South Australia may not have been identified in the South Australian registry of deaths; hence a sensitivity analysis of mortality was undertaken of those with usual residence in South Australia. All analyses were performed in Stata/MP 15.1.
Results
Study cohort
There were 600 patients with an ICU admission diagnosis of SAH over the study period. Five cases were missing a GCS score or outcome data and of the remaining 595 patients, 163 (27%) had a GCS score of six or less. Of these 163 patients, 139 had a confirmed spontaneous SAH, forming the grade V SAH study cohort (Figure 1).
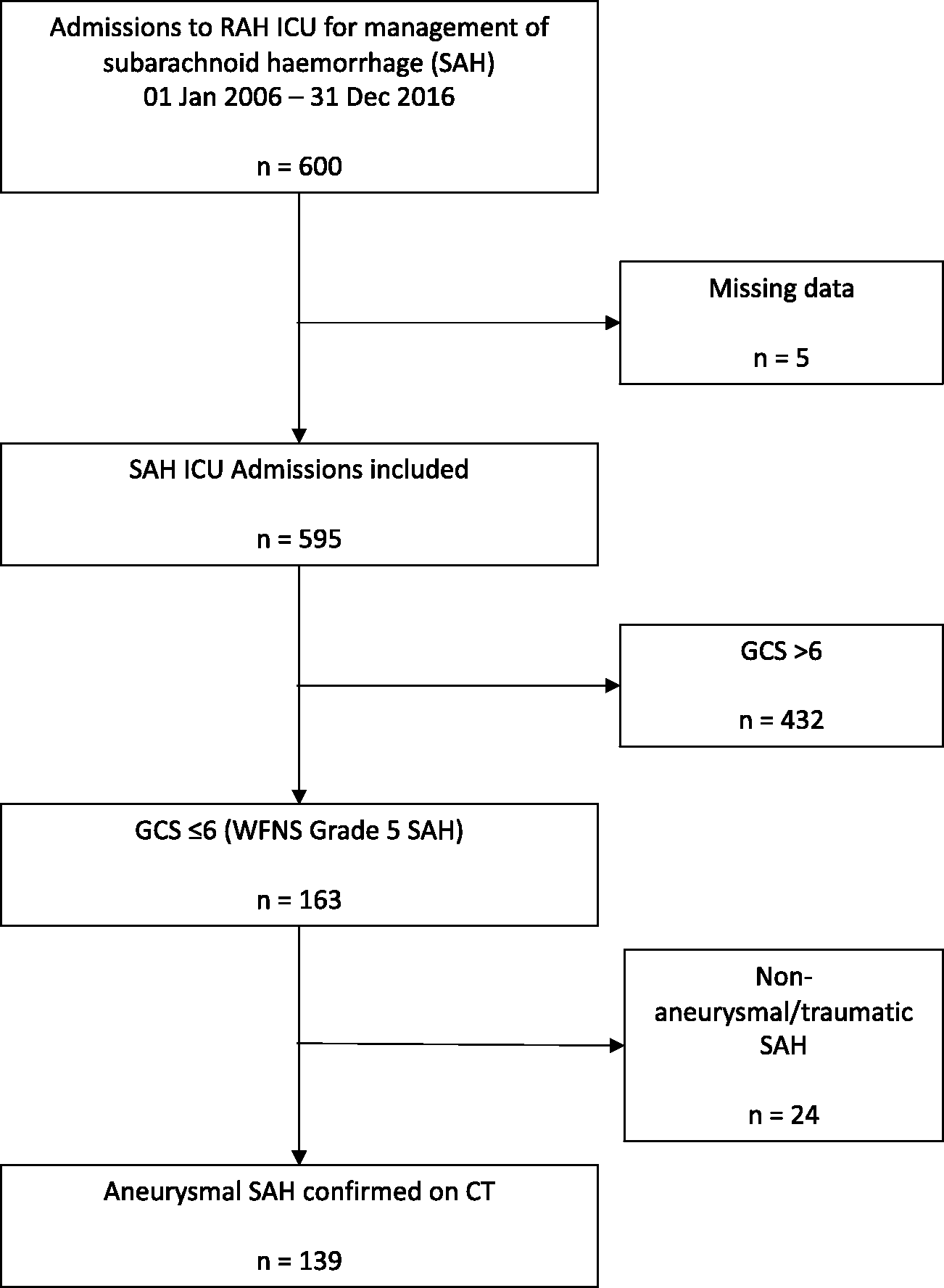
Flow diagram of cases used to identify the cohort of patients with grade V subarachnoid haemorrhage (SAH) admitted to the intensive care unit (ICU) at the Royal Adelaide Hospital (RAH) (2006–2016). GCS: Glasgow Coma Scale; WFNS: World Federation of Neurosurgical Societies; CT: computed tomography.
The mean number of patients admitted each year with grade V SAH was 13 (SD 5) and the proportion of all SAH patients with spontaneous grade V haemorrhage did not change over time.
Cohort characteristics and treatments
Cohort demographics are shown in Table 1. Median age was 56 (IQR 48–70) years and 88 (63%) patients were female. There were 13 (9%) patients with a usual residence outside South Australia and seven (5%) patients were recorded to be Indigenous. A cardio-respiratory arrest prior to admission occurred in 19 (14%) patients. There were 132 patients (95%) with an mFS grade of 4.
Characteristics, treatments and costs of managing patients with grade V subarachnoid haemorrhage.
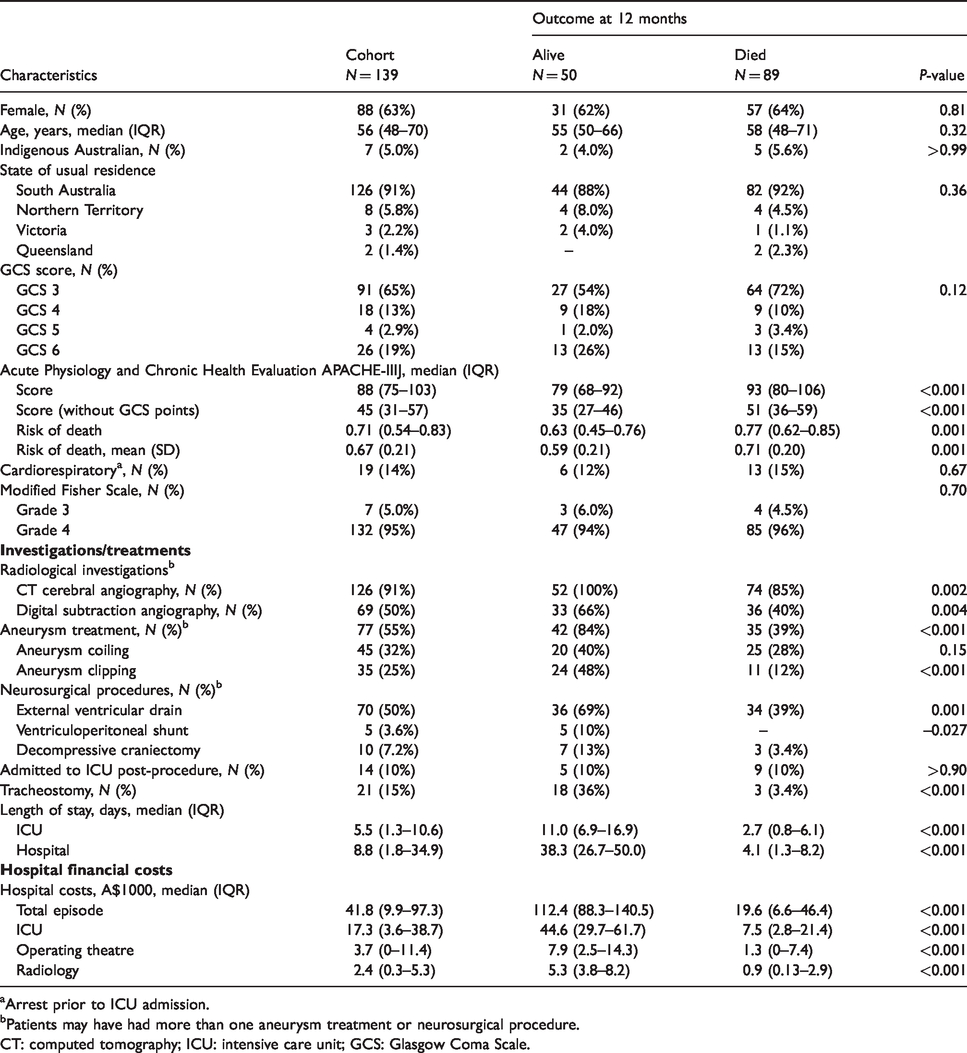
aArrest prior to ICU admission.
bPatients may have had more than one aneurysm treatment or neurosurgical procedure.
CT: computed tomography; ICU: intensive care unit; GCS: Glasgow Coma Scale.
Most patients had imaging of the cerebral circulation; 126 (91%) had a CTA and 69 (50%) had a DSA, of which 19 patients had more than one. A procedure to treat a cerebral aneurysm was undertaken in 77 (55%) patients; 45 (32%) had aneurysm coiling and 35 (25%) had aneurysm clipping. An external EVD inserted was inserted in 70 (50%) and 10 patients (7%) had a decompressive craniectomy. A tracheostomy tube was inserted in 21 patients (15%).
Median ICU and hospital lengths of stay were 5.5 (1.3–10.6) days and 8.8 (1.8–34.9) days respectively.
Mortality
There were 77 (55%) patients who died in ICU, 87 (63%) died in hospital and 89 (64%) had died at 12 months (Figure 2). The proportion of patients that had died at each timepoint did not change over the study period. Sensitivity analysis of the 126 patients with usual residence in South Australia revealed 82 (65%) had died at 12 months.
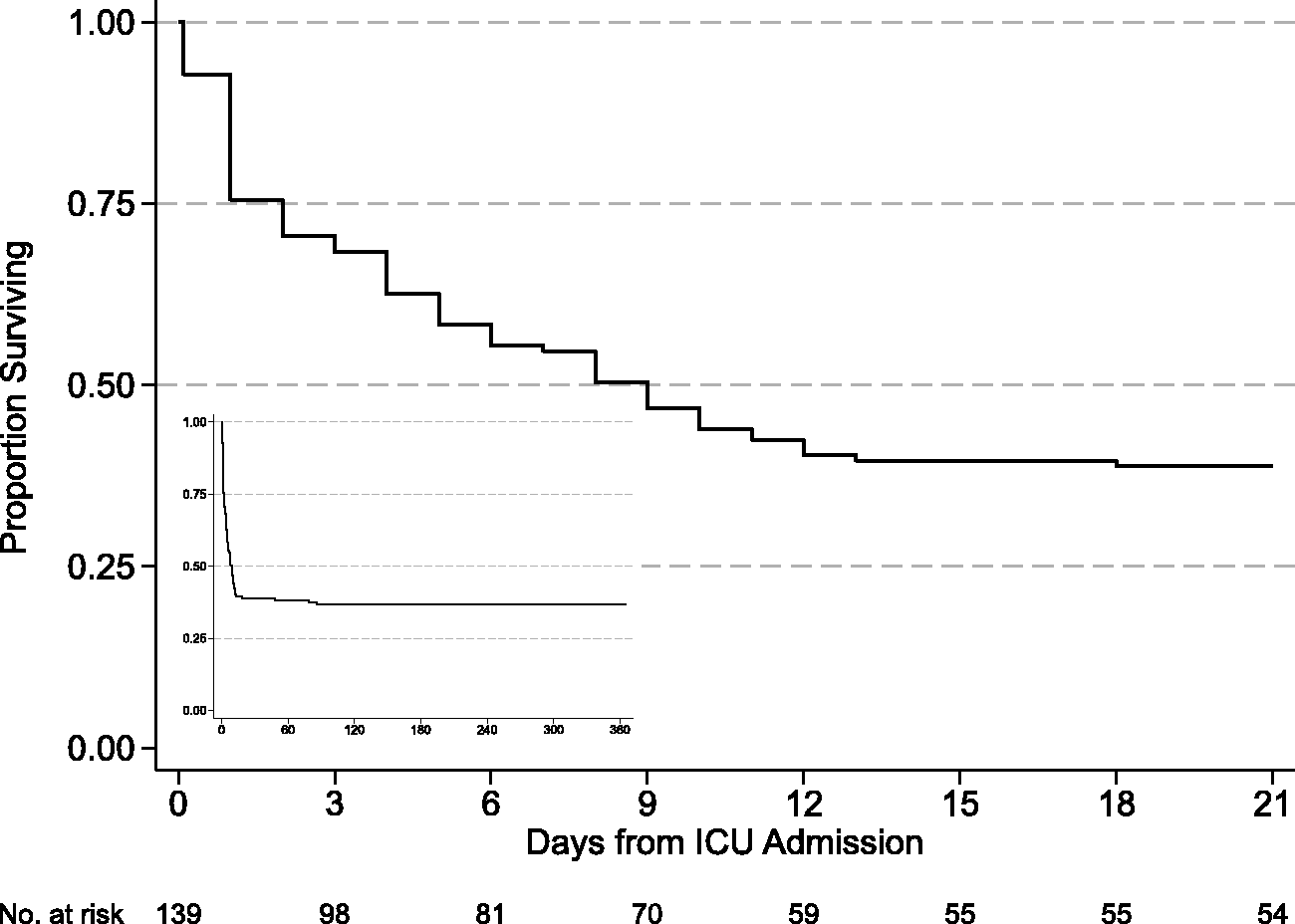
Kaplan–Meier survival curve of 139 patients admitted to the intensive care unit (ICU) with grade V subarachnoid haemorrhage (SAH). Inset figure is the survival curve over 12 months.
Discharge destination
There were 52 (37%) patients who survived to hospital discharge; 33 (63%) were transferred to a rehabilitation facility, 17 (33%) to another acute care hospital (awaiting rehabilitation, a care facility, or returning to an interstate hospital) and two (4%) were discharged.
Organ donation
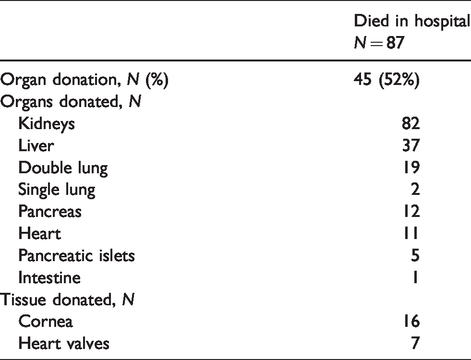
Of the 87 patients who died in hospital, 45 (52%) donated their organs, with 169 organs and 23 tissues transplanted (Table 2). These patients accounted for 23% of the 199 who donated organs from the RAH over the study period.
Organ donation from patients who died following grade V subarachnoid haemorrhage.
Costs
The total hospital cost of managing this cohort was A$8.3 million. The median (IQR) total cost for hospitalisation per patient was A$41,824 (A$9933–A$97,332); this comprised A$17,250 (A$3615–A$38,748) for ICU admission, A$3720 (A$0–A$11,407) for operating theatre and A$2448 (A$264–A$5258) for radiology. All costs were significantly lower in the subgroup of patients who died (Table 1).
Discussion
In this contemporary, single-centre study of patients with grade V SAH, approximately two-thirds died during hospital admission, with few dying over the following 12 months. The annual number of patients admitted with grade V SAH and mortality rates remained unchanged over the 11-year study period. Hospital costs of managing this cohort were substantial, with the ICU component being the most expensive. Half of the patients who died in hospital donated their organs, an important outcome to consider given the high mortality, life years lost and financial cost of this disease.
There have been a number of cohort studies of patients with grade V SAH, all from centres in the northern hemisphere. Patient demographics appear similar to those of our cohort and the hospital mortality rate of 63% appears within the mortality rates of 30%–70% reported in other studies.6,16,18,22–25 Some studies excluded patients who had absent brainstem reflexes or who did not receive aneurysm treatment and under-represent the true hospital mortality of grade V SAH.
We noted that one-third of patients survived to leave hospital and all but two of these were alive at one year. Although we were not able to reliably determine the functional status of hospital survivors, we note other studies of patients with grade V SAH have reported rates of ‘favourable’ outcomes ranging from 9% to 44%.6,8,16,17,22,26 A systematic review of ‘poor grade’ SAH (grade IV and V) reported that 30% of patients had favourable outcomes and this was unchanged over the past 30 years. 6 However, studies reporting functional outcomes have assessed patients at varying timepoints, using different assessment scales, derived functional status in different ways, applied different categories to define ‘favourable’ outcomes and some excluded patients who died or who did not receive aneurysm treatment. This highlights the need for comprehensive monitoring of the functional status of patients with SAH, ideally with a core outcome dataset.
Aneurysm isolation was undertaken in 55% of the study cohort, with 32% having endovascular coiling and 25% aneurysm clipping. By comparison, the prevalence of aneurysm treatment in other cohorts of patients with grade V SAH has been reported to be 67%–80%, with some centres securing aneurysms in all patients with intact brainstem reflexes.8,16,26 The proportion of patients with high-grade SAH having endovascular coiling has increased over time 6 and is consistent with increased use of this technique in lower grade SAH. 14 Furthermore, some advocate that all unconscious patients with SAH should have an EVD, 1 yet we note that the proportion of patients in our study cohort having an EVD inserted (50%) or decompressive craniectomy (7%) is comparable to other studies.6,8,16,18,22,25,27
Cerebral angiography, aneurysm treatment, neurosurgical procedures and tracheostomy were applied less frequently in the subgroup of patients that died. Similarly, their lengths of stay in the ICU and hospital were lower. This will likely represent a bias towards not treating patients considered to have a poor prognosis, contributing to a self-fulfilling prophecy of poor outcomes. For this reason, we deliberately avoided any interpretation of the relationship between therapeutic intervention and outcome.
Total hospital costs amounted to A$8.3 million for treating this cohort and appear expensive given only 52 patients survived hospitalisation. Keeping in mind this was a single-centre study, costs on a national scale would seem significant. Studies from the United Kingdom and United States of America have reported hospital costs per patient with high-grade SAH ranging from A$35k to A$225k (adjusted for 2019 Australian dollars) and there is much variability in what costs were incorporated.29,30 It is likely that greatest financial expense occurs with the care required after hospital discharge. 31 Further study is required to understand the financial implications of treating patients with a high likelihood of poor prognosis, and to understand what constitutes ‘cost-effectiveness’.
In this study, over 60% of patients with grade V SAH died in hospital, with half donating their organs. Organ donation is supported by most of the Australian population and benefits the community through transplant recipients.32,33 Bereaved family members can also find value in fulfilling their loved one’s wishes by altruistically helping other members of society. It is recognised that the net health benefit of organ donation for the community is an effective use of ICU resources in neurological cases with a hopeless prognosis. 34 For example, kidney transplantation (around A$180,000) is cost saving compared to long-term dialysis (around A$80,000 per year).35,36 Admission to ICU and support of patients with grade V SAH allows organ donation to be considered if ongoing active treatment will not achieve a favourable outcome. This is regarded as best quality end-of-life care and is expected by most of the Australian population.37,38
Limitations
There are several caveats to this study. It is a retrospective single-centre study and may not be generalisable to other settings. Independent predictors of outcome were not evaluated due to a relatively small cohort size and the influence of treatment bias. Other clinical variables such as limb motor response, brainstem reflexes, hydrocephalus, aneurysm size, re-bleeding, duration of EVD placement, seizures, cerebral arterial vasospasm and delayed cerebral ischaemia were not obtained. The high mortality rate may represent clinician bias regarding likely patient outcomes and it is not known what proportion of patients died following withdrawal of life-sustaining treatments. Reliable assessment of functional status was not available. Finally, the expenditure incurred following hospital discharge was not available and these costs are likely to be substantially greater than hospital costs.
Conclusion
Grade V SAH is a catastrophic event for most patients, their families and the community. Two-thirds of patients died within the 12 months following presentation and hospital costs were substantial. Of those who died in hospital, half donated their organs, partially offsetting the burden of this disease to the community. Further study is required to understand long-term functional recovery in patients with grade V SAH.
Footnotes
Acknowledgements
We would like to thank the RAH Case Mix Unit for providing data for this study.
Author contributions
All authors contributed to data interpretation and provided intellectual input into the manuscript. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.