
Abstract
Microcirculatory alterations play an important role in the early phase of sepsis. Shedding of the endothelial glycocalyx is regarded as a central pathophysiological mechanism causing microvascular dysfunction, contributing to multiple organ failure and death in sepsis. The objective of this study was to investigate whether endothelial glycocalyx thickness at an early stage in septic patients relates to clinical outcome. We measured the perfused boundary region (PBR), which is inversely proportional to glycocalyx thickness, of sublingual microvessels (5–25 µm) using sidestream dark field imaging. The PBR in 21 patients with sepsis was measured within 24 h of admission to the intensive care unit (ICU). In addition, we determined plasma markers of microcirculatory dysfunction and studied their correlation with PBR and mortality. Endothelial glycocalyx thickness in sepsis was significantly lower for non-survivors as compared with survivors, indicated by a higher PBR of 1.97 [1.85, 2.19]µm compared with 1.76 [1.59, 1.97] µm, P=0.03. Admission PBR was associated with hospital mortality with an area under the curve of 0.778 based on the receiver operating characteristic curve. Furthermore, PBR correlated positively with angiopoietin-2 (rho=0.532, P=0.03), indicative of impaired barrier function. PBR did not correlate with Acute Physiology and Chronic Health Evaluation IV (APACHE IV), Sequential Organ Failure Assessment score (SOFA score), lactate, syndecan-1, angiopoietin-1 or heparin-binding protein. An increased PBR within the first 24 h after ICU admission is associated with mortality in sepsis. Further research should be aimed at the pathophysiological importance of glycocalyx shedding in the development of multi-organ failure and at therapies attempting to preserve glycocalyx integrity.
Keywords
Introduction
The microcirculation has been increasingly acknowledged to play a key role in the pathophysiology of various disease states.1,2 Microcirculatory derangements may include decreased microvascular density, perfusion and oxygen exchange, along with increased flow heterogeneity in patients with septic shock.3,4 The glycocalyx, a gel-like layer covering the luminal side of the vascular endothelium, is an important regulator of the microcirculation. It primarily consists of proteoglycans with covalently linked glycosaminoglycans, glycoproteins and glycolipids.5,6 Under physiological conditions the endothelial glycocalyx provides an important stabilising barrier as it regulates activation of coagulation factors such as protein C and tissue factor, prevents leakage of plasma components, inhibits platelet activation and blocks leukocyte adhesion.7,8
Glycocalyx degradation has been linked to increased oedema formation, enhanced leukocyte extravasation, and a decreased microcirculatory perfusion, leading to organ failure.9–11 A surrogate marker of glycocalyx shedding is the transmembrane heparan sulphate proteoglycan syndecan-1, which was found to correlate with sepsis severity and mortality.12–15 Interestingly, syndecan-1 levels in non-survivors remained elevated over the course of disease signifying ongoing glycocalyx shedding, while they decreased in sepsis survivors. 12 While there appears to be a clear relationship between biomarkers of glycocalyx degradation and mortality in sepsis, no studies are available that link direct visualisation of the glycocalyx with mortality in sepsis.
Over the last decade, the development of non-invasive imaging techniques such as sidestream dark field (SDF) imaging has resulted in a better understanding of the role of the microcirculation in disease.16–19 SDF imaging makes use of the easily accessible sublingual microcirculation to investigate the condition of microvessels in more detail. Several studies have indicated that the sublingual vasculature is representative for the rather inaccessible intestinal or cerebral microvascular beds, because it is affected in a similar manner.20–22 SDF imaging has been used in many clinical studies to investigate the microvasculature in pathological states such as stroke, 23 chronic kidney disease (CKD)24–26 and sepsis.3,4,19,27–30 One of the measured parameters is the perfused boundary region (PBR), an inverse parameter of glycocalyx thickness on endothelial cells of sublingual microvessels. 31 Thus, an increased PBR indicates a decreased glycocalyx thickness. The PBR was indeed shown to be significantly increased in critically ill patients as compared with healthy controls. 28 However, it remains unclear whether the PBR itself is a prognostic marker able to identify sepsis patients at high risk for organ failure and death.
In our study, we aimed to investigate the association between glycocalyx degradation and mortality in septic patients. The glycocalyx was assessed within 24 h after intensive care unit (ICU) admission by SDF imaging and results were related to biomarkers of glycocalyx degradation (syndecan-1 and heparin-binding protein (HBP)) and vascular permeability (angiopoietin (Ang)-1 and Ang-2)).
Materials and methods
Patients
For this study, 21 septic patients admitted to the ICU of the Maastricht University Medical Center (MUMC+) in Maastricht, the Netherlands, were included between May 2016 and September 2017. Inclusion criteria were: age > 18 years; absence of oral bleeding, wounds or infections; absence of variations in mean arterial pressure (MAP) > 10 mmHg in the ten minutes prior to measurements; absence of variations in medication and fluid administration in the ten minutes prior to measurements; and a diagnosis of sepsis according to the Sepsis-3 criteria. 32 Exclusion criteria were non-invasive ventilation and/or use of a high nasal flow cannula. In addition, the SDF camera had to be available and a researcher experienced with performing SDF measurements had to be present. Demographic variables, routine laboratory data and physiological parameters were collected during the first 24 h after ICU admission. A subgroup of patients with septic shock was identified according to the Sepsis-3 criteria, defined as sepsis accompanied by a lactate value of > 2 mmol/l and the use of vasopressors (norepinephrine (noradrenaline)) to maintain a MAP of ≥ 65 mmHg. 32
All procedures complied with the guidelines of the Declaration of Helsinki and were approved by MUMC Institution’s Medical Ethical Committee (project number 154269). Informed consent was obtained from all patients or their representatives.
Sublingual glycocalyx measurement
The sublingual endothelial glycocalyx thickness was studied by non-invasive SDF imaging. Image acquisition (CapiScope HVCS, KK Technology, Honiton, UK) and analysis was performed by GlycoCheck™ software (Microvascular Health Solutions Inc., Salt Lake City, UT, USA). In brief, images of approximately 14 mm2 are recorded when image quality is deemed sufficient by the software (this is based on focus, motion and intensity). All microvessels between 5 and 25 µm in diameter are then automatically identified. These microvessels are divided in vascular segments of 10 µm along the length of the detected vasculature. The lateral movement of red blood cells (RBCs) into the glycocalyx at these points can be detected, which is expressed as the PBR. A disturbed glycocalyx leads to an increased lateral movement of RBCs and thus an increased PBR. Each measurement consists of at least 3000 vascular segments. In our study, three consecutive measurements were performed by an experienced researcher and averaged to generate a mean PBR value per patient to improve data reliability and quality. Data collected in our ICU population showed that averaging three consecutive measurements improved reproducibility; intraclass correlation coefficient changed from poor to excellent. 33
Laboratory measurements
Values for creatinine, C-reactive protein, total haemoglobin, lactate, bilirubin, thrombocytes and leukocytes were obtained from routine clinical chemistry laboratory tests. At the same time as the glycocalyx assessment, blood from an arterial catheter was drawn into tubes containing either 3.2% citrate or ethylenediaminetetraacetic acid (EDTA; BD, Franklin Lakes, NJ, USA) and immediately centrifuged two times for 12 minutes at 2000 g at room temperature. Plasma samples were stored at –80°C until measurement of established markers of the microcirculation, reflecting increased vascular permeability (Ang-1, Ang-2 and HBP; R&D Systems, Minneapolis, MN, USA) or glycocalyx shedding (syndecan-1; Abcam, Cambridge, UK) by commercial enzyme-linked immunosorbent assay (ELISA) according to the manufacturer’s instructions.
Statistical analyses
For analysis of risk factors predicting mortality, patients were divided in two groups according to hospital mortality. Continuous variables are presented as median with interquartile range [IQR] and tested by the Mann–Whitney test. Proportional data were analysed using the Chi-squared test. A receiver operating characteristic (ROC) curve was generated to evaluate the discriminative ability of PBR for predicting hospital mortality. To that end the area under the curve (AUC), including a 95% confidence interval (CI), was used. Significance of the AUC was tested against an AUC of 0.5. Correlations between variables were calculated using the Pearson correlation coefficient if these variables were normally distributed, or the Spearman rank correlation coefficient for other variables. Data analysis was performed using SPSS version 24.0 (SPSS, Inc., Chicago, IL, USA). P-values < 0.05 were regarded as statistically significant.
Results
Study population
Baseline characteristics are shown in Table 1. Within our study population, 45% were male and the overall median [IQR] age was 67 [61–76] years, the median Acute Physiology and Chronic Health Evaluation IV (APACHE IV) score 99 [60–136] and the mortality rate 43%. Only median APACHE IV scores (67 [56–103] for survivors and 140 [94–145] for non-survivors P = 0.006) differed significantly between survivors and non-survivors.
Baseline characteristics for the entire study population as well as for survivors and non-survivors separately.
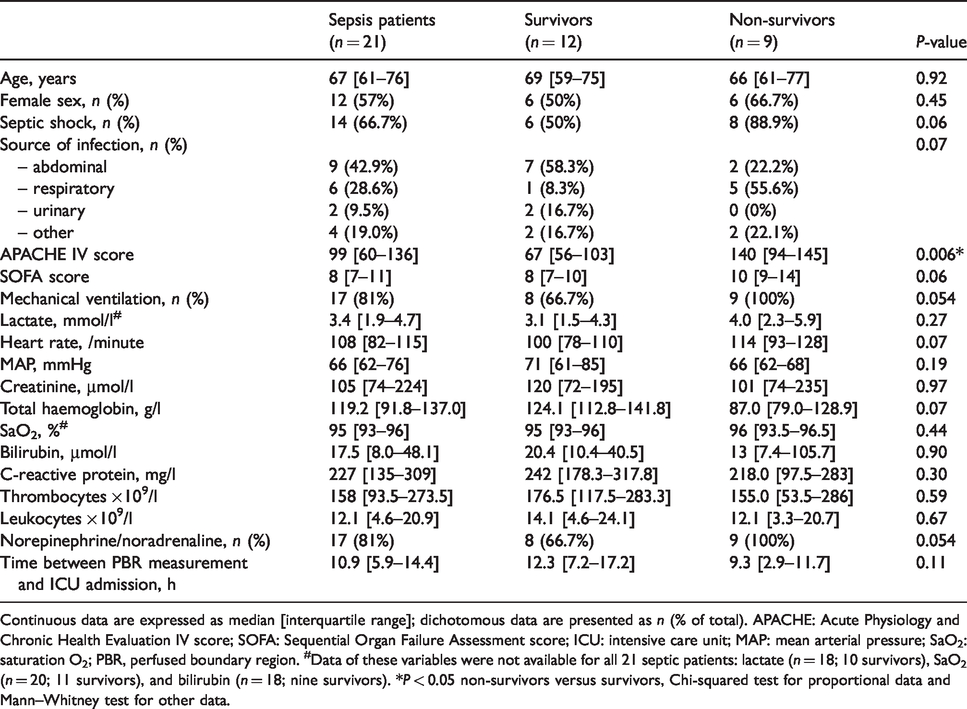
Continuous data are expressed as median [interquartile range]; dichotomous data are presented as n (% of total). APACHE: Acute Physiology and Chronic Health Evaluation IV score; SOFA: Sequential Organ Failure Assessment score; ICU: intensive care unit; MAP: mean arterial pressure; SaO2: saturation O2; PBR, perfused boundary region. #Data of these variables were not available for all 21 septic patients: lactate (n = 18; 10 survivors), SaO2 (n = 20; 11 survivors), and bilirubin (n = 18; nine survivors). *P < 0.05 non-survivors versus survivors, Chi-squared test for proportional data and Mann–Whitney test for other data.
PBR and mortality
The PBR was significantly lower in septic patients who ultimately survived to hospital discharge compared with non-survivors (median [IQR] 1.76 [1.59–1.97] µm, versus 1.97 [1.85–2.19] µm; P = 0.03) (Figure 1). Admission PBR can be considered a predictor of hospital mortality based on the ROC curve with an AUC of 0.778 (95% CI 0.578 to 0.977; P = 0.03) (Figure 2(a)). Other variables showed an AUC of 0.847 (95% CI 0.657 to 1.000; P = 0.008) for APACHE IV score and an AUC of 0.663 (95% CI 0.405 to 0.920; P = 0.25) for lactate.
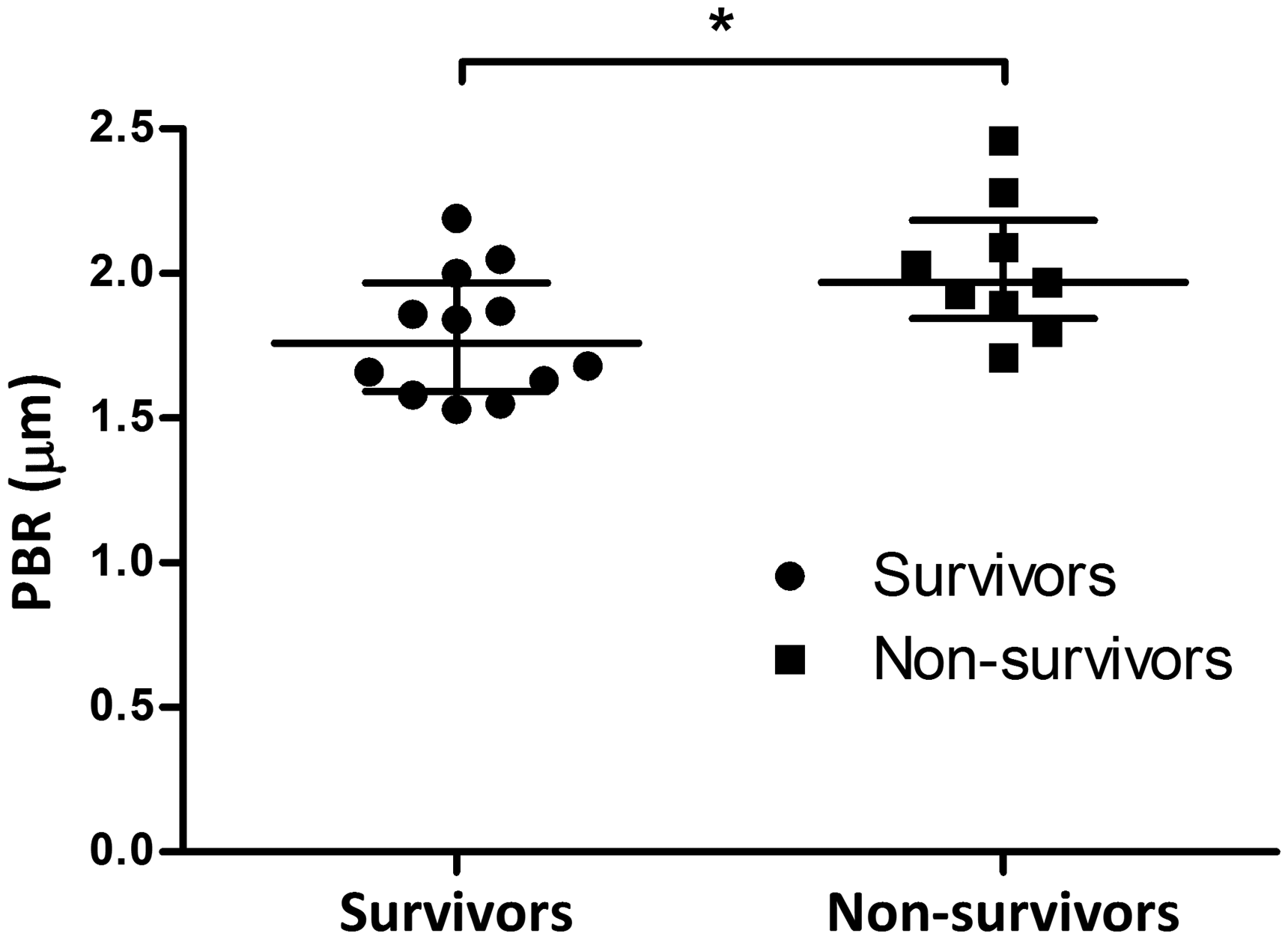
Perfused boundary region (PBR) measurements at admission in sepsis survivors (n = 12) and non-survivors (n = 9). Bars indicate median and interquartile range. *P < 0.05.
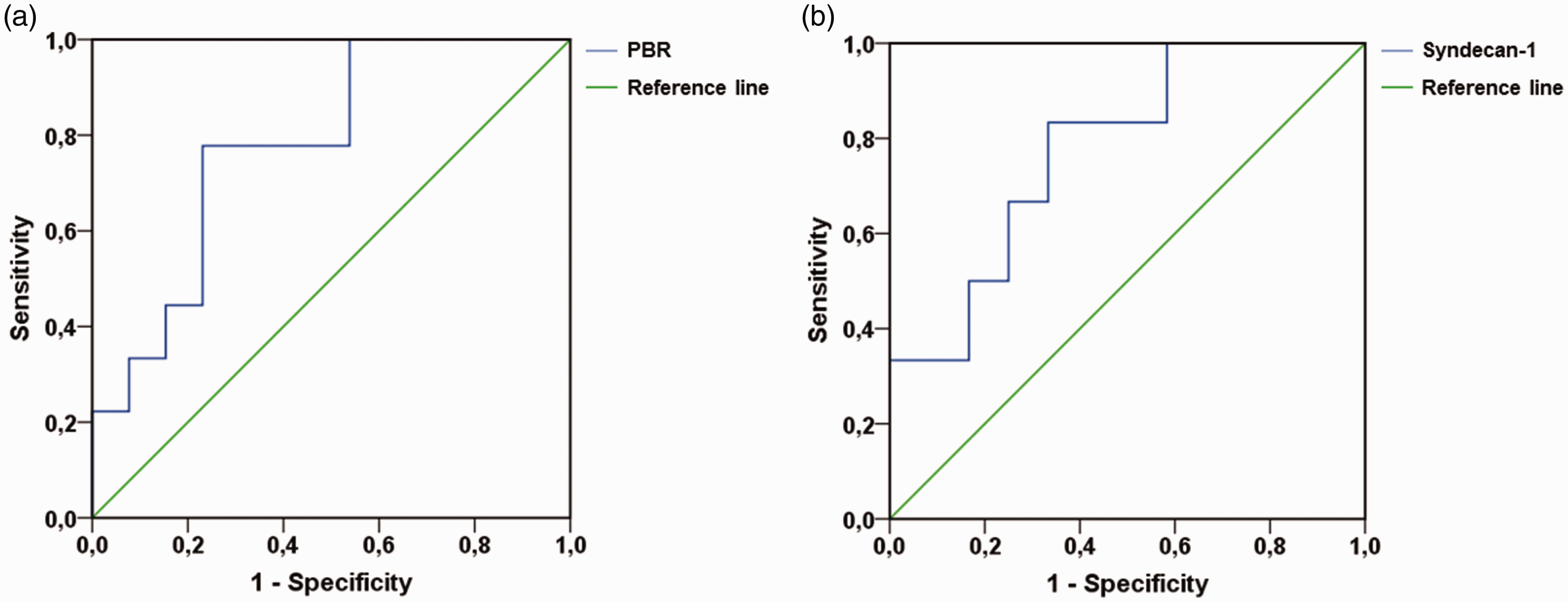
Receiver operating characteristic (ROC) curves of PBR and syndecan-1 for predicting hospital mortality in sepsis. (a) admission PBR (AUC = 0.778; 95% CI 0.582 to 0.977; P = 0.033) and (b) admission syndecan-1 (AUC = 0.781; 95% CI 0.610 to 1.000; P = 0.035). Reference lines have an AUC of 0.5. PBR: perfused boundary region; AUC: area under the curve; CI: confidence intervals.
PBR and circulating microcirculatory markers
We analysed circulating markers in plasma drawn at the moment of PBR measurements in 17 patients (11 survivors and six non-survivors). Syndecan-1 levels were increased in the group of non-survivors as compared with survivors of sepsis (P = 0.04). The ROC curve of syndecan-1 gives an AUC of 0.781 (95% CI 0.610 to 1.000; P = 0.04) (Figure 2(b)). Ang-1, Ang-2 and HBP did not show statistically significant differences between survivors and non-survivors (Table 2).
Biochemical data for sepsis survivors and non-survivors.
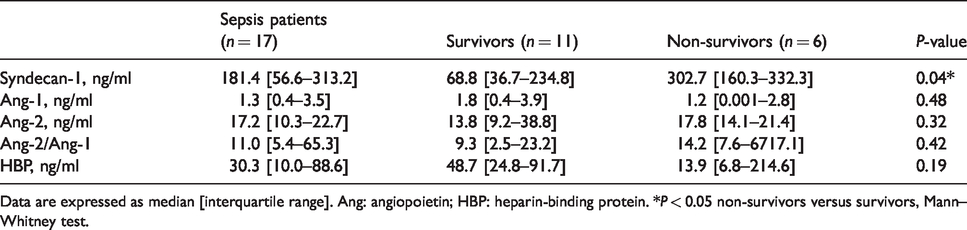
Data are expressed as median [interquartile range]. Ang: angiopoietin; HBP: heparin-binding protein. *P < 0.05 non-survivors versus survivors, Mann–Whitney test.
When studying the correlation between these plasma markers and the sublingual microcirculation as measured by non-invasive SDF imaging, admission PBR showed a positive correlation with Ang-2 levels (n = 17, rho = 0.532, 95% CI 0.069 to 0.806, P = 0.03) (Figure 3) but no statistically significant correlation with syndecan-1 (Figure 4) nor any of the other microcirculatory markers tested (Ang-1, Ang-2/Ang-1, and HBP, all n = 17, Table 3) or the clinical parameters APACHE IV (n = 21, r = 0.101, 95% CI –0.345 to 0.510, P = 0.66), lactate (n = 18, r = –0.053, 95% CI –0.424 to 0.507, P = 0.83) and Sequential Organ Failure Assessment (SOFA) score (n = 21, r = –0.040, 95% CI –0.463 to 0.398, P = 0.86).
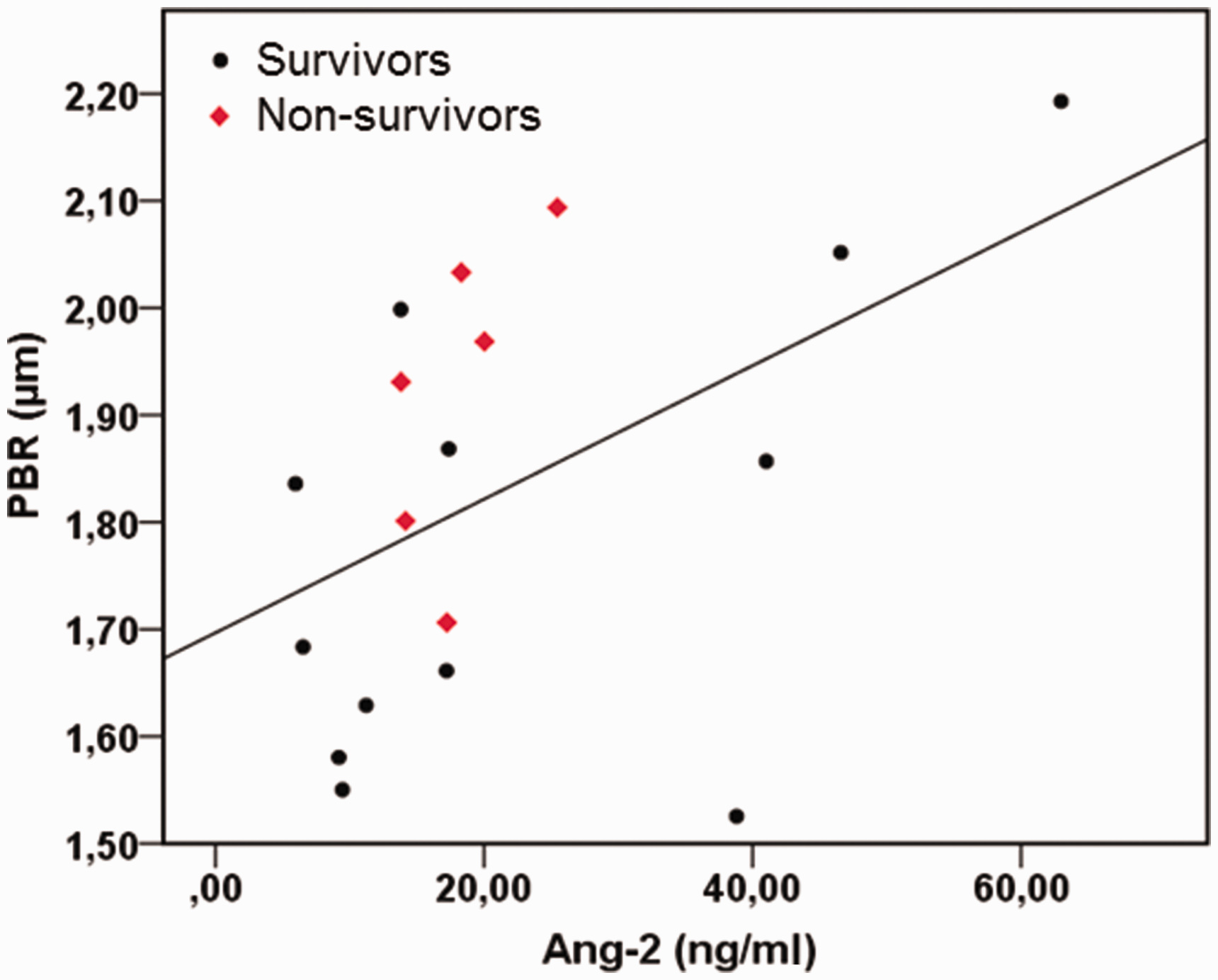
Correlation between admission PBR and angiopoietin-2 (Ang-2) in sepsis (n = 17). PBR showed a positive correlation with Ang-2 levels (rho = 0.532, 95% CI 0.069 to 0.806, P = 0.03). rho, Spearman’s correlation coefficient; PBR: perfused boundary region.
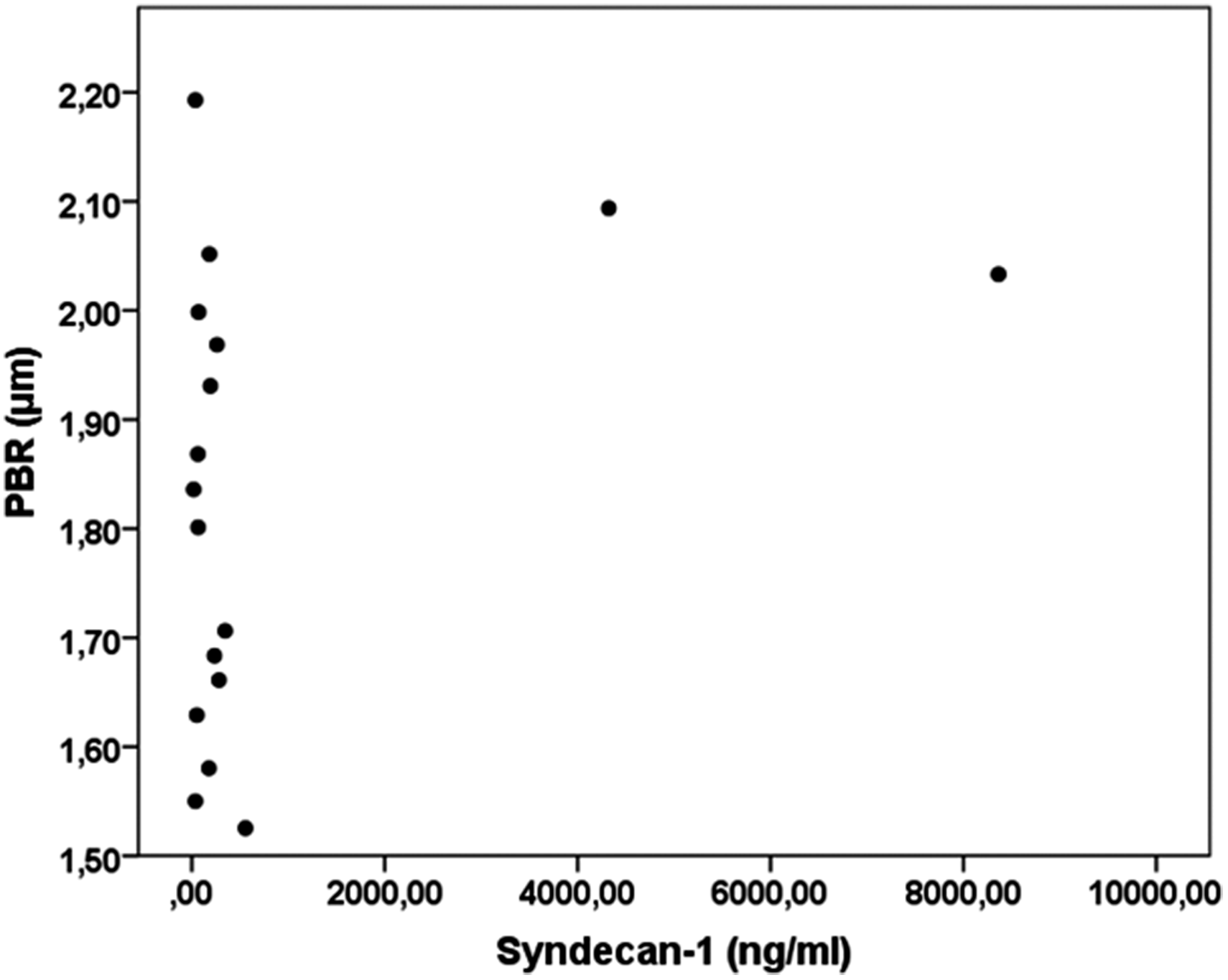
Perfused boundary region (PBR) measurements at admission versus syndecan-1 (n = 17). There was no correlation between PBR and syndecan-1.
Correlations between admission PBR and circulating markers.
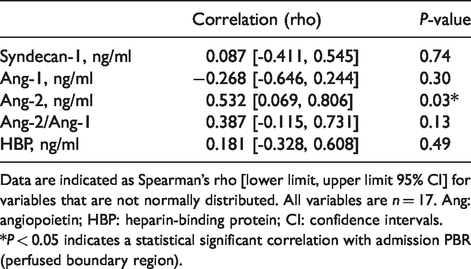
Data are indicated as Spearman’s rho [lower limit, upper limit 95% CI] for variables that are not normally distributed. All variables are n = 17. Ang: angiopoietin; HBP: heparin-binding protein; CI: confidence intervals. *P < 0.05 indicates a statistical significant correlation with admission PBR (perfused boundary region).
Discussion
We have found that PBR values during the first 24 h of ICU admission are associated with outcome in critically ill septic patients. Previous studies showed glycocalyx shedding to be associated with oedema, microthrombi, inflammation, leukocyte adhesion and low flow. 34 It is plausible that this negatively affects outcome. Whether the relationship is truly causal, however, remains a point of investigation.
In our cohort the PBR measured within the first 24 h was predictive for outcome. This finding should be confirmed in a larger validation cohort. Such a study should investigate the influence of factors such as age and chronic disease on the relationship between PBR and mortality.
Interestingly there was only a limited correlation between glycocalyx thickness as directly visualised using SDF imaging and measured using plasma markers of glycocalyx degradation and microcirculatory dysfunction. Only syndecan-1 was increased in non-survivors as compared with survivors. Our initial hypothesis was that syndecan-1 and PBR would also be correlated, as both are interpreted as indicators of glycocalyx degradation. However, our results did not support this assumption (rho = 0.087, P = 0.74), though the variability in our study population is rather great. These findings are in line with several other studies in various populations that did not observe a correlation between these parameters in haemodialysis,24,26 CKD24,25 and sepsis. 27 Discrepancy between PBR and the measured glycocalyx constituent is also observed by Cornelis et al., who measured increased syndecan-1 levels after haemodialysis, while PBR did not alter. 24 Moreover, Donati and colleagues also tested other constituents of the glycocalyx and its relation to PBR. Hyaluronan did not show a correlation with PBR and only a minor positive correlation was found for heparan sulphate (HS). 27 Several explanations can be conceived why glycocalyx thickness measured directly using SDF imaging does not correlate with plasma markers of glycocalyx shedding.
The PBR is defined as the cell-poor layer resulting from the phase separation between the flowing RBC and plasma, including the most luminal part of the glycocalyx that allows cell penetration. 23 HS is a more superficial glycocalyx marker that lines the inside of the glycocalyx, while syndecan-1 is the core protein binding HS and is anchored within the cell membrane. 35 It can be hypothesised that the earlier damage will first result in a shedding of HS, and that the more substantial damage which occurs later results in syndecan-1 release. However, Smart and colleagues showed in a cohort of septic patients in the emergency department that hyaluron, which is directly bound to the endothelium in the deepest layer, rose fast whereas syndecan-1 rose slowly. 36 In contrast, Gonzalez Rodriguez et al. found syndecan-1 to be high upon admission at the emergency department in trauma patients. 37 These findings would imply that PBR and syndecan-1 reflect different aspects of glycocalyx damage or that underlying pathologies can affect glycocalyx components differently. Another possible explanation could be a difference in the timing or localisation of syndecan-1 release and the measured PBR. Heterogeneity in underlying disease state could have resulted in a variation in the kinetics of syndecan-1 in plasma, with possible differences in release, basal turnover and/or clearance.38–40 Furthermore, the difference in individual glycocalyx thickness could lead to a greater variation in PBR and/or circulating syndecan-1 levels. Irrespective of the underlying mechanisms, our data indicate that PBR and syndecan-1 could be independent markers of glycocalyx disruption and combining these two markers may enhance discriminative ability. Unfortunately the sample size of this study precluded any such analysis.
PBR did correlate positively with Ang-2 levels. The positive relationship of PBR with Ang-2 supports the idea that glycocalyx degradation is connected to vascular permeability, 7 with Ang-2 being able to induce heparanase-mediated glycocalyx degradation. 41 This correlation has also been observed in patients undergoing kidney transplantation. 25 Another permeability marker measured in our study, HBP, was not found to be correlated with PBR. A possible explanation for this difference is that HBP is released by activated neutrophils, 42 while Ang-2 originates from Weibel–Palade bodies in endothelial cells. 43 In our study, we did not specifically look at endothelial activation markers, but in a study by Dane et al., PBR and soluble thrombomodulin levels were related to each other. 25 The glycocalyx and endothelium interact with each other in health and disease, and many markers of endothelial activation have been linked with sepsis severity and microcirculatory alterations.35,44,45 Other groups have shown low levels of Ang-1 and high levels of Ang-2 and HBP to be related with mortality and multiple organ dysfunction in severe infection46–48 and sepsis.49–51
A limitation of the present study is that we solely looked at admission levels of PBR and circulatory markers of the microcirculation. It is known that microcirculatory alterations can persist for days, with syndecan-1 remaining elevated up to at least 50 h in haemorrhagic shock 29 and seven days in sepsis. 12 Normalisation of these levels is observed in survivors, while syndecan-1 remained elevated in non-survivors.12,29 Syndecan-1 differed between survivors and non-survivors in our sepsis cohort. Other studies also found syndecan-1 levels to be higher in non-survivors of trauma 52 or sepsis.12,13 Other clinically relevant markers could not distinguish survivors from non-survivors in our cohort of relatively ill septic patients.
The present study was set up in a single centre with one expert measuring the glycocalyx thickness in all patients. While this approach limits inter-hospital and inter-operator variability, it may have introduced bias. In addition, one would ideally correct for possible confounders and covariates, such as APACHE IV and lactate, using multivariable logistic regression. The limited sample size, however, did not allow this. It would be interesting to see how confounders and covariates influence the relationship between PBR and mortality. Serial imaging of the microcirculation in the critically ill has also indicated that the changes in microvessel density and perfusion show good discriminative ability in distinguishing survivors from non-survivors.30,53 These studies all indicate that temporal improvements in these parameters were typically observed for survivors. Therefore, it would be interesting to investigate the course of serial PBR measurements in patients with sepsis and its relation with both circulating markers and clinical outcome.
In conclusion, we show that a thinner glycocalyx layer, as measured by PBR, is associated with increased mortality in ICU patients admitted with sepsis. It remains to be seen whether glycocalyx degradation merely is a marker of an adverse outcome of sepsis or whether it is actually causally related. In the latter case preservation of glycocalyx integrity may become an interesting focus for future therapeutic interventions aimed at reducing multi-organ failure and mortality in sepsis.
Footnotes
Acknowledgement
We would like to thank Dr. B. Winkens, statistician at the University of Maastricht, Faculty of Health Sciences, Department of Methodology and Statistics, for his guidance and advice regarding the statistics.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was received from an unrestricted grant from the Coenraad Hemker Foundation.