
Abstract
Smoke inhalation resulting in acute lung injury is a common challenge facing critical care practitioners caring for patients with severe burns, contributing significantly to morbidity and mortality. The intention of this review is to critically evaluate the published literature and trends in the diagnosis, management, implications and novel therapies in caring for patients with inhalation injury.
Introduction
Smoke inhalation resulting in acute lung injury (SI-ALI) is a common challenge facing critical care practitioners caring for patients with severe burns. A recent study evaluating the epidemiology of severe burn injury patients admitted to burn referral centres in Australia and New Zealand reported that among 496 patients included with 20% or greater total body surface area burn (TBSA), 40% had sustained an inhalation injury. 1 Evidence suggests SI-ALI contributes significantly to morbidity and mortality; in a landmark study reported by the United States Army Institute of Surgical Research, mortality appeared to increase by a maximum of 20% in the presence of inhalation injury and by as much as 60% when inhalation injury and pneumonia coexisted. The effect of inhalation injury and pneumonia on mortality were found to be both independent and additive. 2
Our group recently conducted a survey of critical care practice amongst Australasian intensivists caring for patients with severe burns 3 and demonstrated a remarkable degree of heterogeneity in the approach to diagnosis, fluid resuscitation and pharmacotherapy in this cohort of patients. The intention of this review is to critically evaluate the published literature and trends in the diagnosis, management, implications and novel therapies in caring for patients with inhalation injury.
Pathophysiology
The pathogenesis of SI-ALI is yet to be fully elucidated; however, it is well recognised that several components are involved in the ultimate injury and may include direct thermal injury, airway obstruction mediated by particulate matter and a complex inflammatory cascade activated by smoke particles (Figure 1).
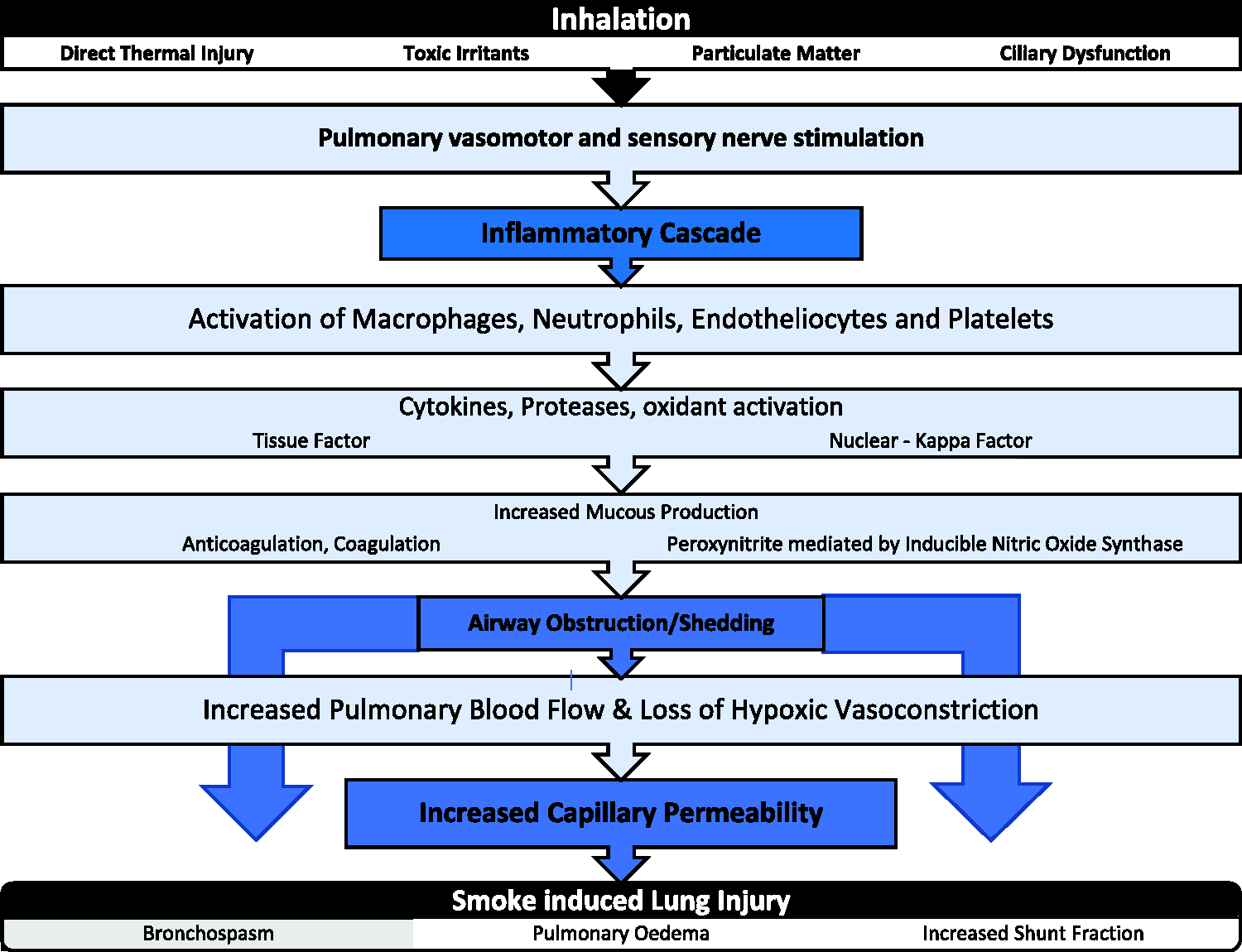
Pathogenesis of thermal/smoke inhalation injury.
Pulmonary injury from smoke inhalation potentially results from both direct thermal and chemical insults. Following inhalation, most heat is very effectively dissipated by the upper airways prior to the smoke reaching the carina. Super-heated inhaled gas (>150°C) may, however, immediately damage the mucosa with subsequent oedema and necrotic shedding. As a result of the highly effective gas cooling mechanism mediated through heat absorption by the capillary blood of the nose/pharynx and the protective reflexes of epiglottic closure, reflex laryngeal spasm and reflex constriction of the airways, direct thermal damage is most likely to affect the supraglottic airways. 4
Smoke contains toxic gases, as well as suspended particulate matter. Large inhaled particles are effectively trapped proximally in the respiratory tract, whereas toxic gases and particles smaller than 5–10 µm are deposited in the peripheral airways. Furthermore, in the presence of fire, oxygen is depleted resulting in a hypoxic environment, with products of combustion such as carbon dioxide generated that displace oxygen at the level of the alveolus, resulting in asphyxia. The production of carbon monoxide in the setting of combustion also contributes to hypoxia through its avid affinity for haemoglobin. This results in the competitive displacement of oxygen from haemoglobin and the binding of carbon monoxide to mitochondrial cytochrome oxidase. 5
Respiratory irritants including halogens, sulphur dioxide, formaldehyde and aldehydes may also be products of combustion depending on the substrate fuel. The ensuing airway irritation results in sloughing of respiratory mucosa and the establishment of an inflammatory cascade, leading to a profound local and systemic host inflammatory response (Figure 2).
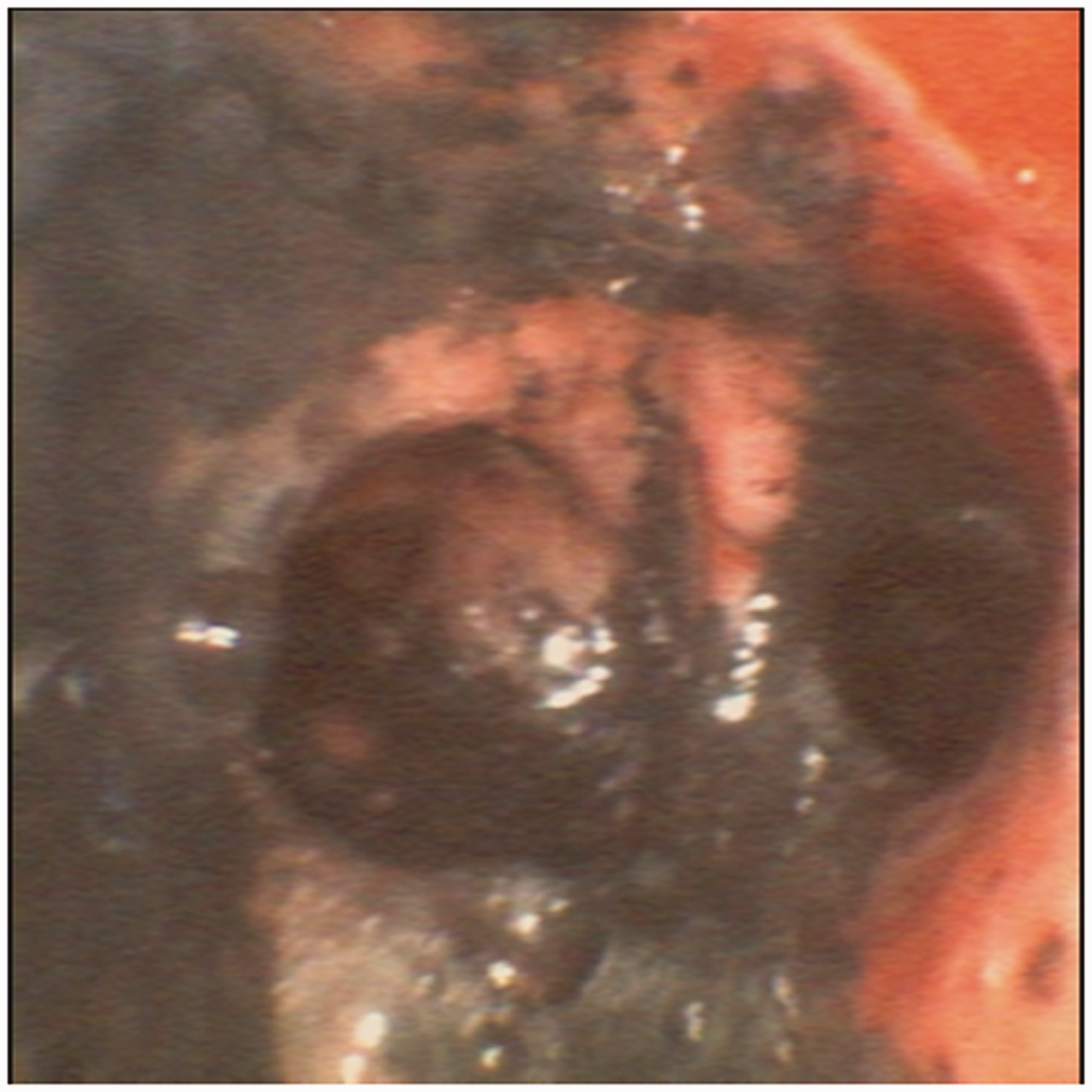
Grade 3 inhalational injury.
The pulmonary vasomotor and sensory nerves are believed to be stimulated by noxious inhaled material, with the subsequent release of neuropeptides that are also implicated in inducing an inflammatory response. Animal studies have demonstrated significant neuropeptide-induced pulmonary inflammation. 6
Smoke inhalation initiates cytokine release with upregulation of inducible nitric oxide synthase. The consequence of this upregulation is substantially increased bronchial blood flow with impairment of hypoxic vasoconstriction. This results in the increased delivery of activated leukocytes and cytokines, further amplifying the inflammatory cascade. Increased capillary permeability results from the inflammatory process, leading to subsequent loss of protein into the interstitial tissue with exudate and cast formation within the airways. Airway obstruction may then lead to alveolar collapse.
Clinical presentation
Most patients presenting to an emergency department with inhalational injury are conscious with a patent airway and unremarkable chest X-ray and arterial blood gas analysis. Full manifestations may occur as late as 48 hours after the inhalation insult. 7
Physical findings that support a concomitant inhalation injury include carbonaceous sputum, stridor, wheezing, facial burns, singed nasal hairs, cough and dyspnoea; however, these findings may be misleading. 8 Similarly, the history, including estimated duration of exposure, type of burning material, location of injury and any loss of consciousness, may raise suspicion for inhalational injury.
Diagnosis
Currently, there is no recognised standard for diagnosing and grading the severity of inhalational injury. Although most burn centres rely on fibreoptic bronchoscopy to diagnose inhalational injury, there are little data relating bronchoscopic findings to outcomes in burn patients. 9
Traditionally, inhalation injury was diagnosed based on physical findings and historical features including confined space exposure, loss of consciousness or exposure to chemicals and smoke. Clinical features on examination, such as labial burns, singed facial or nasal hair or carbonaceous staining of the face or in the sputum, have been regarded as compelling evidence for inhalation injury. However, recent work suggests history and these physical findings are not particularly sensitive or indeed specific for the presence of inhalational injury.8,10
It is therefore important the critical care physician confirms airway damage using alternative strategies. Clinical examination findings, although potentially unreliable, are useful as a screening tool to select appropriate patients for evaluation by bronchoscopy. Ching et al. found bronchoscopy to be a useful diagnostic modality in a large (n = 9775) study using the National Burns Repository, to diagnose inhalation injury and severity. In this study bronchoscopy proved useful in predicting mortality, days of ventilation and duration of intensive care unit (ICU) admission. 11 Therefore bronchoscopy may have the advantage of securing the diagnosis while simultaneously allowing severity assessment (Table 1) and facilitating bronchial toilet and specimen collection. 12
Bronchoscopic inhalation injury grade.
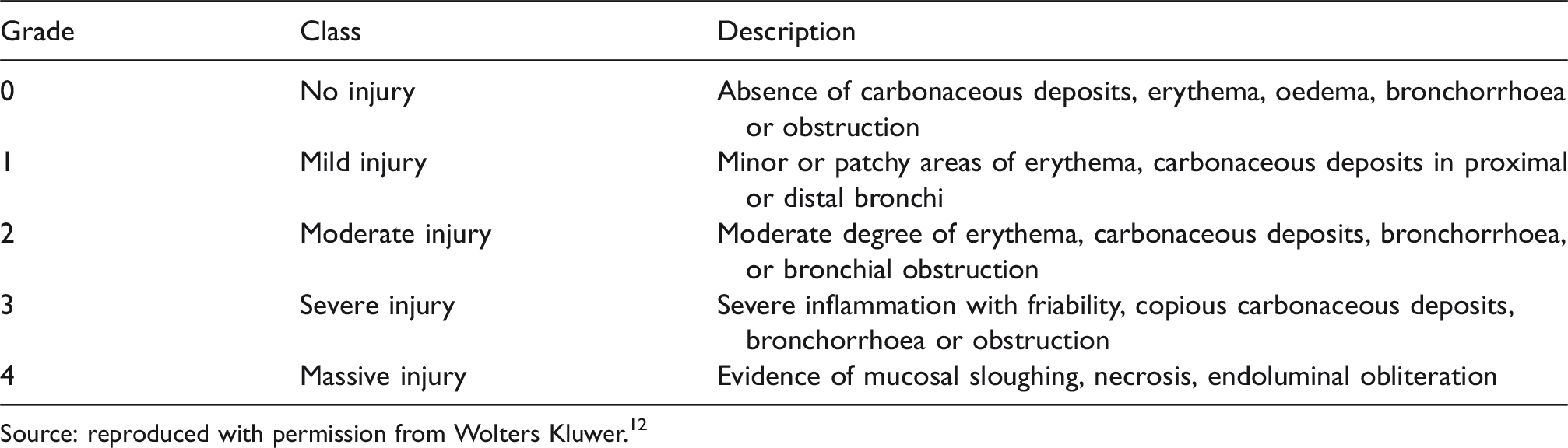
Source: reproduced with permission from Wolters Kluwer.12
Helical computed tomography (CT) can effectively evaluate airway wall thickness and airway-lumen dimensions in asthma and chronic obstructive pulmonary disease. There is increasing evidence that using thoracic CT scans in patients with inhalational injury, obtained within a few hours of admission, is predictive of the development of pneumonia, ventilator days and ICU stay.13,14 Oh et al. performed 14 a retrospective study on 25 inhalation injury patients, applying a CT grading system previously developed for an ovine smoke inhalation model 15 (see Table 2).
Radiologist’s scoring table (RADS score) for inhalation injury.
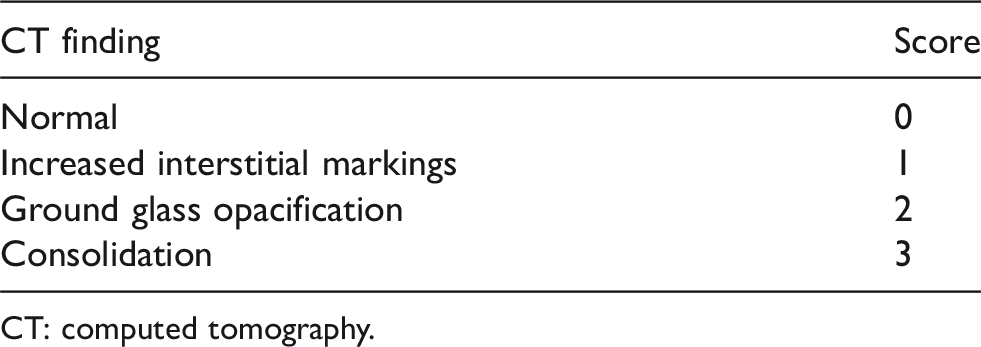
CT: computed tomography.
They were able to demonstrate that the presence of inhalation injury on bronchoscopy and an elevated radiologist’s score on a thoracic CT performed in the 24-hour period following admission was associated with a 12.7-fold increase in the incidence of the composite endpoint of pneumonia, ventilator days and mortality. 14
Resuscitation
Appropriate resuscitation with intravenous fluids based on estimated percentage body surface area burn and patient weight is the initial challenge of acute burns management. The implications of an associated inhalational injury on fluid resuscitation in burn patients are not entirely clear. In a recent survey of practice among intensivists working at burns referral centres in Australasia, 3 there was substantial variation in the approach to fluid resuscitation in patients with inhalation injury. Half the intensivists surveyed indicated that inhalational injury would not alter their initial fluid resuscitation, whereas the other half would modify their fluid delivery. Again, there was significant variation, with some intensivists increasing the resuscitation volume and others decreasing it. A sentinel case report, describing an isolated inhalational injury in the absence of cutaneous involvement, reported a resuscitation fluid volume requirement equivalent to a 27% TBSA cutaneous burn. It was this publication that initially informed the debate as to the fluid requirements in inhalation injury. 16 The fluid requirements in patients with an inhalational injury have been studied, but largely in retrospective patient cohorts.17,18 The consensus opinion currently indicates a significantly increased fluid demand in the presence of inhalational injury compared to patients with the same percentage cutaneous burn but without inhalational injury. 19 Inoue demonstrated an additional and independent increase in fluid delivered in the presence of an inhalational injury. 20 Navar reported a statistically significant increase in mean fluid requirement from 3.98 ml/kg per % TBSA to 5.76 ml/kg per % TBSA in patients with an inhalational injury. 17 However, Dai demonstrated lower total fluid resuscitation volumes, but also a modest increase in those with inhalational injury (3.1 ml/kg per % TBSA versus 2.3 ml/kg per % TBSA without inhalational injury). 21 However, other studies have failed to demonstrate this increased resuscitation fluid requirement in patients with an inhalational injury. Interpretation of these studies is challenging because of the significant differences in the resuscitation approach employed, including clinical endpoints and fluid type used.
Fluid type
The fluid of choice in the resuscitation of a burns patient with an inhalational injury is yet to be resolved. An ovine model demonstrated the use of albumin as a means of supporting colloid osmotic pressure minimised the increase in extravascular lung water and the authors also inferred smoke inhalation does not lead to a dramatic increase in alveolar capillary membrane permeability to protein. 22
A study with patients distributed across albumin and crystalloid groups equally failed to demonstrate different outcomes in the first 14 days on the development of multiple organ dysfunction scores, including duration of mechanical ventilation in the patients with inhalational injury. 23 A recent meta-analysis specifically evaluated the prescription of albumin in inhalational patient groups and concluded that limited evidence and uncertainty suggests adequately powered, high-quality trials are necessary to determine the impact of albumin resuscitation on mortality in burn patients. 24
The transfusion requirement in the presence of an inhalational injury has also been studied by way of a secondary analysis of data from the TRIBE study. 25 The authors reported that patients with inhalation injury received more blood transfusions than those without. However, inhalation injury itself was not responsible for the increased transfusion requirement, but rather a function of this group of patients requiring mechanical ventilation, their advanced age, larger burn size and increased incidence of bloodstream infections. The rational use of blood products in the burn population, particularly those with inhalation injury, remains an important area for prospective study.
Respiratory support
The potentially progressive nature of the airway oedema requires a low threshold for intubation and mechanical ventilation be maintained in suspected inhalation injury. An estimated 33% of burn patients require mechanical ventilation and this increases substantially when there is a concomitant inhalational injury. 26 Usually the attending clinician has time to evaluate the patient’s airway; however, immediate intubation may be required in the setting of a reduced level of consciousness, impending or actual airway obstruction, cardiac arrest or inadequate ventilation. There is a recognition that there is a significant proportion of patients who do not require intubation that are subjected to this intervention, but the consequences of not proceeding to intubation may be life-threatening, therefore increasing the need to establish reliable guidelines.27,28 In this regard, nasolaryngoscopy has increased in popularity as a screening tool, although the definitive role of this strategy is yet to be established. The major benefit of nasolaryngoscopy is preventing intubation in a few, select symptomatic patients with a negative study. 29 In the presence of facial burns, following intubation it is the practice at our institution to have an alveolar ridge screw placed at one of the early visits to the operating theatre. This effectively and safely secures the endotracheal tube without compromising facial tissue or the tapes becoming soiled (Figure 3).

Alveolar ridge screws to secure the endotracheal tube.
There is very limited value for non-invasive ventilation in patients with potential inhalation injury, as they have an ongoing risk of airway compromise in the setting of resuscitation, often a requirement for several visits to the operating theatre and significant analgesic requirements. An important consideration in the potential success of non-invasive ventilation is patient selection. Patients must be awake, cooperative, spontaneously breathing and be able to protect their airways. Haemodynamic instability also precludes the use of non-invasive ventilation. High secretion production and facial burns are often associated with inhalational injury, making this group of patients unsuitable for non-invasive ventilation.
Invasive ventilator strategies employed for patients with inhalational injuries are required to preserve gas exchange and minimise further injury. There is no ideal ventilatory mode that can be advised; however, certain respiratory support strategies can be recommended based on general consensus recommendations for mechanical ventilation. 30 The use of low tidal volumes, tolerating moderate hypercapnia and maintaining plateau pressures less than 30 cmH2O is an appropriate approach to preserve aerated lung tissue. Prevention of intrapulmonary shunt-induced hypoxaemia requires the preservation of open lung units for gas exchange through the judicious use of positive end-expiratory pressure (PEEP). In the setting of atelectasis or oedema, PEEP may increase functional residual capacity, optimise compliance on the pressure volume curve, decrease the work of breathing and minimise venous admixture. In burn patients with oedematous and eschar-constricting chest walls and abdomens, it is possible that insufficient transpulmonary pressures are generated and inadequate lung opening is achieved based on accepted pressure limits. In this situation, urgent escharotomies maybe required together with a liberalisation of pressure limits.
There are reports of the beneficial effects of high-frequency oscillatory ventilation (HFOV) in improving oxygenation in burn patients with acute respiratory distress syndrome following inhalation injury. 31 This initial enthusiasm for the use of HFOV in burns patients is moderated by conflicting evidence in the literature surrounding its use in nonburn critically injured populations, which failed to demonstrate benefit and even showed potential harm with HFOV use.32,33 A recent systematic review concluded high-frequency percussive ventilation may decrease in-hospital mortality and pneumonia incidence when compared to standard controlled mechanical ventilation. However, the authors conceded the absence of ‘good’ quality evidence precluded performing a meta-analysis. 31
The epidemiological findings of the National Burn Repository published in 2014 reported that pneumonia remains the most frequent complication in burn injury patients, particularly in those patients receiving longer than four days of mechanical ventilation. 34 Therefore, prevention strategies, including elevation of the head of the bed, frequent position changes, judicious use of sedation, chlorhexidine oral care and supraglottic suction, should be fastidiously enforced. Antibiotic prophylaxis in burn patients appears ineffective and may increase infection rates and therefore should not be routinely employed. 35 It is also vital these patients receive adequately humidified oxygen to prevent secretions from thickening.
Inhaled therapy
There is no specific therapy that targets inhalational injury; however, there are a range of supportive interventions, based on biological plausibility, that are potentially suitable to treat the physiologic perturbations associated with smoke inhalation.
Anticoagulation
In inhalational injury, airway obstruction results from the formation of airway casts generated by the presence of mucous, sloughed epithelial cells and fibrin. Fibrinogen, which is present in the inflammatory exudate associated with inhalational injury, transforms into fibrin (Figure 1). Aside from forming casts in the airway that are difficult to mobilise and evacuate, the presence of fibrin disrupts the function of surfactant, diminishing the surface tension and precipitating atelectasis.
There are several animal models and single-centre clinical trials that have investigated the use of inhaled heparin therapy in inhalation injury.36,37 Importantly, this therapy appears safe and is not associated with clinically significant systemic anticoagulation or bleeding. However, there are no multicentre, prospective trials confirming a clinical benefit from inhaled heparin in this setting.
Nebulised heparin in combination with N-acetylcysteine gained popularity as a treatment strategy following a study that demonstrated decreased mortality in paediatric patients with inhalation injury. 38 However, these findings were not confirmed by a subsequent retrospective review of 150 patients with inhalation injury and the combination of heparin and N-acetylcysteine provided no significant improvement in clinical outcome. 39
Inhaled heparin has also been combined with systemic lisofylline, an anti-inflammatory agent, in an ovine model. Sheep received one of three treatment strategies: nebulised saline alone, nebulised heparin alone or nebulised heparin and intravenous lisofylline. Treatment with nebulised heparin in isolation was unable to ameliorate pulmonary dysfunction following severe smoke injury. The combination of nebulised heparin and systemic lisofylline had beneficial effects on pulmonary function in association with a decrease in blood flow to poorly ventilated areas of lung and less lipid peroxidation. 40
Unfortunately, the utility of inhaled heparin in inhalational injury remains to be confirmed, although the evidence would suggest it is safe. The HEPBURN study results are still to be reported. This is an international multicentre, double-blind, placebo-controlled study that aims to recruit 116 intubated and ventilated burn patients with confirmed inhalation trauma. Patients will be randomised to nebulisation with heparin or nebulisation with normal saline every four hours for 14 days or until extubation. The primary endpoint will be the number of ventilator-free days. 41
Nebulised tissue plasminogen activator (TPA), a fibrinolytic agent, has been used in an ovine model with animals subjected to a combined burn or smoke inhalation injury. Treatment of injured sheep with 2 mg of TPA improved pulmonary gas exchange, decreased pulmonary oedema, and decreased airway obstruction. 42 The same group of investigators also explored the value of aerosolised heparin and recombinant human antithrombin in an ovine inhalation injury model. 43 The two agents in combination conferred an advantage with respect to improved lung compliance, less pulmonary oedema and decreased airway obstruction. It is important these strategies are evaluated in humans with thermal inhalation injury.
Bronchodilators
Airway mucosal hyperaemia occurs soon after inhalation injury, with a 20-fold increase of blood supply resulting in a physical narrowing of the airways. 44 This hyperaemia also enhances oedema and generates increased airway exudate/fibrin. Bronchospasm is further exacerbated by neuropeptide release (Figure 1). Bronchospasm is also generated by the chemical irritants and toxins present in the inhaled smoke.
The use of salbutamol (a β2 agonist) via continuous nebulisation in a sheep laboratory model of inhalation injury has been tested. 45 Sheep subjected to a severe smoke inhalation and 40% TBSA burn injury were treated with continuous nebulised salbutamol at 20 or 40 mg/hr and compared with sheep treated with nebulised saline. Sheep nebulised with continuous salbutamol displayed a 30% reduction in peak and plateau airway pressures, improvement in PaO2/FiO2 ratio and a decreased pulmonary shunt fraction. 45 Despite this work, prospective clinical data on the efficacy of β2 agonists in inhalation injury are lacking. The therapeutic value of β2 agonists in inhalation injury needs to be confirmed with rigorous trials in human subjects.
The parasympathetic nervous system contributes to bronchospasm via acetylcholine secretion in response to airway irritation. Acetylcholine then occupies the muscarinic receptors, resulting in airway smooth muscle constriction and stimulation of submucosal gland secretion. Therefore, inhibition of these muscarinic receptors could inhibit these effects and decrease bronchospasm and inflammation. The muscarinic antagonist, tiotropium bromide, has been tested in an ovine inhalation model. 46 Sheep with an inhalational injury receiving tiotropium bromide showed decreases in ventilatory pressures and upper airway obstruction and an improved PaO2/FiO2 ratio as compared to untreated controls. Again, prospective human studies are required.
Conclusions
Inhalational injury in patients with thermal injury is common and adversely effects mortality, the subsequent development of pneumonia, duration of ventilation and length of intensive care admission. Furthermore, the presence of inhalational injury has important implications for diagnosis, airway management, fluid resuscitation, ventilation strategies and adjuvant therapies. Although our understanding of the pathophysiology has substantially improved, the evidence base to guide critical care physicians is not only weak but conflicted in many areas of management. 47
Based on the current available evidence, it is our practice to employ the strategies outlined in Table 3, in the delivery of care to burns patients with potential inhalation injuries.
Management principles applied in burn patients with inhalation injury.
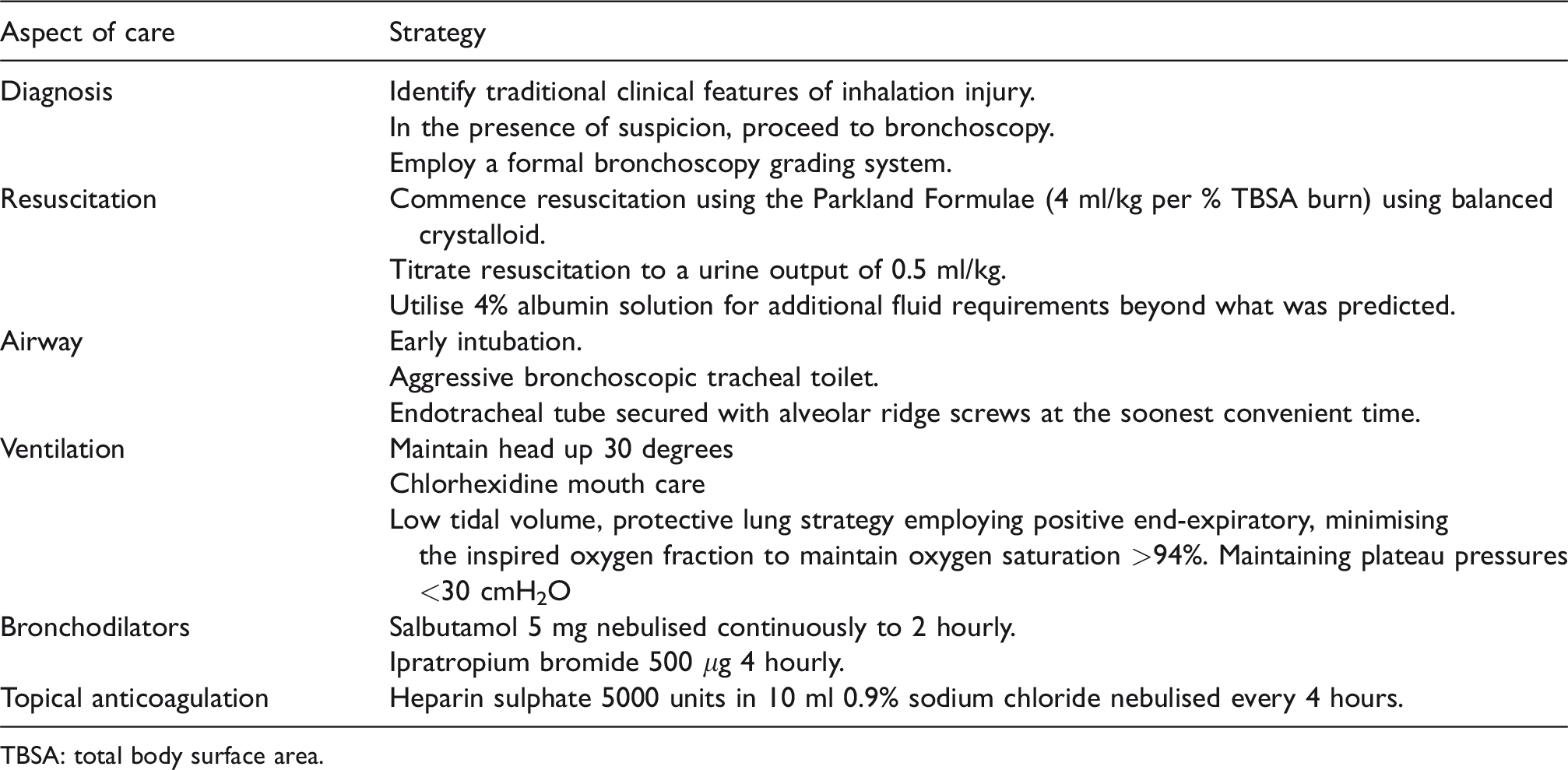
TBSA: total body surface area.
It is important that Australasian intensive care establish a reliable burns critical care data repository to collect relevant, prospective information that will ultimately facilitate the development of evidence-based guidelines to assist in the complex management of inhalational injury. Well designed interventional studies can then follow to answer many of the unresolved issues we have considered.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. None of the authors have a conflict of interest in respect to publication of this paper to declare. There was no funding received to support this publication. Informed consent was obtained for the photographs and subsequent publication.