
Abstract
Burnout is a work-specific syndrome with high incidence among intensive care unit personnel. Although several risk factors have been proposed, data regarding the association of anxiety and burnout among intensive care unit physicians are scarce. The aim of this study is to investigate the incidence of burnout and its association with state and trait anxiety and other sociodemographic, behavioural and occupational-related parameters, among intensivists. A population of intensive care physicians was evaluated using the self-completed Maslach Burnout Inventory and the State-Trait Anxiety Inventory Form Y, and data regarding sociodemographic and occupational-related variables were also recorded. From the 98 intensive care physicians addressed, 80 returned fully completed questionnaires; 26.9% of them presented with high emotional exhaustion, 37.5% with high depersonalisation and 41.5% with low personal accomplishment scores. Trait anxiety, fear of having committed a medical error and self-reporting difficulty when having to act accurately were independently associated with high burnout. In conclusion, burnout is common among intensivists and is associated with specific behavioural characteristics and personality traits, but not with work-related factors.
Introduction
Burnout syndrome (BOS) is usually described as an emotional condition characterised by mental fatigue, physical fatigue, frustration and disengagement.1–4 It is a work-specific syndrome of emotional exhaustion, depersonalisation and a reduced sense of personal accomplishment among individuals who work with people in some capacity 5 and is more likely to occur when goals and expectations are too high, or reality is too low, 1 resulting in an imbalance between invested and gained resources. BOS has a clearly relational character, especially affecting people working in highly demanding jobs in which they develop intense relationships; given the characteristics of the work in an intensive care unit (ICU), which is a highly demanding task engaging life or death decisions, it is expected that ICU practitioners are exposed at a high risk of burnout. Published literature data confirm that ICU physicians constitute a high-risk population, reporting a burnout prevalence up to 50%, 6 although incidence might be somehow overestimated or underestimated, mainly because diagnosis is based on subjective and self-reporting criteria. 1 Although heavy workloads, workplace environment, issues related to patient care and end-of-life decisions have been previously associated with the presence of burnout among critical care personnel,6,7 published literature varies widely regarding the identification of independent risk factors related to burnout occurrence among ICU physicians.
The ICU is a complex working environment characterised by a high level of work-related stress. 8 As Maslach and Leiter have recently highlighted, BOS is the result of prolonged interpersonal stressors at work. 9 However, under the same working conditions, some individuals burn out and some others have no symptomatology; 10 therefore, a person’s reaction to work stressors might range from minor to significant stimulation. 11 This varies employees’ reactions to working in a stressful environment and might be due to different personality characteristics. 11 Personality can either involve to a coping mechanism that allows individuals to acquire and/or conserve resources and protect themselves from deviant behaviour or it can make someone more susceptible and vulnerable to stressors. 12 One crucial psychological phenomenon that is related to personality is anxiety. 11 Although anxiety is a psychological condition that acts as a protective factor against threatening situations, prolonged anxiety might result in psychological distress affecting an individual’s everyday functioning. 13 Anxiety is further divided into two related components: trait and state anxiety. 14 In more detail, trait anxiety is a stable characteristic of an individual’s personality and the degree to which they perceive stressful situations as threatening. In contrast, state anxiety is the individual’s reaction toward a situation after having appraised it as threatening. 15 In other words, an individual’s proneness to anxiety reflects trait anxiety, whereas an individual’s reaction after a situation has been characterised as threatening is state anxiety. 11
Previous published studies have reported an association between occupational burnout and increased anxiety in various populations, such as healthcare workers, 16 nurses 17 and medical residents,18–20 with emotional exhaustion being the burnout dimension that established the strongest correlation to anxiety. However, to the authors’ knowledge, literature data exploring such an association among ICU physicians is scarce. Nevertheless, establishing such a relationship is important for the identification of the physicians at ‘higher risk’ for burnout and, consequently, for the prevention, follow-up and adequate treatment of the disorder. Thus, we conducted a cross-sectional study aiming to investigate: (a) the incidence of BOS, (b) the potential association between the three dimensions of BOS and the levels of anxiety, as assessed by the State-Trait Anxiety Inventory (STAI), and (c) the potential association of BOS with other individual and occupational-related factors, in a population of intensivists employed in ICUs of two European countries.
Materials and methods
Study design and study population
This is a cross-sectional, multicentre, non-interventional study that was conducted in seven adult ICUs in Greece and two adult ICUs in Cyprus, which had a similar structure and treated both surgical and medical patients. All physicians employed in these ICUs (either consultants or ICU medicine residents) were considered eligible for participation. The health system in these two European countries is similar, as is the organisational structure of the ICUs in general. The participation was voluntary and the ethics committees of the relevant institutions in Greece and Cyprus approved the conduct of the study.
Data collection
A detailed letter describing the purpose of the study and the data collection procedure along with a sufficient number of questionnaires were mailed to each ICU, addressing all employed physicians. All completed and anonymised questionnaires (each one placed in a closed envelope) were collected in a separate file and were either mailed back to a given address or picked up from the ICU by MK, depending on the personnel’s convenience. A total of three reminder mails were sent to each ICU within a two-month time frame to increase the response rate. Each participant was administered the following questionnaires:
Questionnaire 1 recorded sociodemographic data, occupational data and data regarding the structure of the ICU (e.g. number of ICU beds, working hours per week, number of shifts per month, etc.). Questionnaire 2 comprised 15 separate questions that investigated the specific circumstances and working conditions that physicians: (a) wished to be different or (b) find difficult to cope with (e.g. ‘Do you find it difficult to cope when you have to rush into decisions? (yes/no)’). Questionnaire 3 recorded information on hobbies, smoking and alcohol consumption, and leisure time. Questionnaire 4 was the STAI Form Y
21
, which is a 40-item self-completed questionnaire, comprising two subscales (Y-1 and Y-2). The STAI Form Y-1 consists of 20 items that measure transient stress, which is the stress at the time of the survey (state anxiety), and the STAI Form Y-2 consists of another 20 items that measure permanent stress as a personality trait (trait anxiety). All items are rated on a four-point Likert-type scale. The scoring weights for the anxiety-present items are the same as the blackened numbers on the test form. The scoring weights for the anxiety-absent items are reversed.
21
The total score ranges from 20 to 80 for each STAI subscale and the higher the score, the higher the stress. The STAI has been previously translated and validated in the Greek population.
22
Questionnaire 5 was the Maslach Burnout Inventory-Human Services Survey™ (MBI-HSS) used under licence from Mind Garden (granted 6 April, 2014). MBI is a 22-item self-completed questionnaire that assesses the three dimensions of burnout: Emotional Exhaustion (EE) (nine items), Depersonalization (DEP) (five items) and Personal Accomplishment (PA) (eight items).
23
Each item is scored on a 0–6 point Likert-type scale. The MBI evaluates the attitudes, feelings and perceptions of physicians concerning their work environment. It is the most widely employed measure, it has high reliability and validity
6
and has been previously translated and validated for the Greek population.
24
The MBI-HSS authors have validated the following definitions of low, moderate and high scores for each of the burnout dimensions: EE: high ≥27, moderate: 19–26 and low ≤18; DEP: high ≥10, moderate: 6–9 and low ≤5; and PA: low ≤33, moderate: 34–39 and high ≥40 (the latter is an inverse scale). High, moderate and low levels of EE or DEP, or low, moderate and high levels of PA are used to indicate high, moderate and low levels of burnout, correspondingly.
23
Statistical analysis
All analyses were conducted using the SPSS Edition 18 for Windows XP. The Shapiro–Wilk test of normality was utilised to evaluate the normality of distribution of values; P ≥ 0.05 indicated a normal distribution. Continuous variables are presented as mean (standard deviation) or median (range), according to their distribution of values and categorical variables as percentages. As MBI is a norm-referenced scale, one-third of respondents are expected to score high in each subscale. 23 Thus, the observed number of responses were compared to the expected ones, using a Chi-square test to define whether the number of respondents with high levels of burnout were significantly different than the expected one. All subjects with high levels of burnout based on the score of any of the three subscales (high BOS group) were compared to the rest of the subjects (non–high BOS group); the independent sample student’s t-test or Mann–Whitney U test were utilised to compare continuous variables and Chi-square or Fisher’s exact test were used to compare categorical variables between these two groups, according to the distribution of their values. The Bonferroni correction for multiple comparisons was applied and a level of P < 0.025 (after correction) was considered significant for group comparisons. Univariate logistic regression analyses were conducted to identify potential associations between the establishment of high BOS and (a) the two dimensions of the STAI questionnaire and (b) any of the rest of the recorded parameters. Variables that were found to be univariately associated with high BOS were then entered in a multivariate logistic stepwise regression analysis model for potential predictors of BOS to be identified. Correlations between the STAI subscales and the three dimensions of MBI-HSS were further studied using the Pearson correlation coefficient, r. Odds ratios (OR) and corresponding 95% confidence intervals (CI) were calculated for all multivariate predictors; a level of P < 0.05 was considered significant for all regression analyses.
Results
Eighty fully completed questionnaires were returned out of 98 sent, which corresponded to a response rate of 81.6%. Respondents comprised of 40.2% (n1 = 33) male and 59.8% (n2 = 49) female physicians aged an average of 43 (32–65) years.
BOS incidence and group differences
High BOS, established as a high score in either EE or DEP or low score in PA dimension, was present among 68.8% (N = 55/80) of physicians. High EE was present among 21 physicians (26.9%), high DEP among 30 (37.5%), whereas PA was low among 34 (41.5%) of them. However, as the expected count for a high score in each MBI dimension for this population was 26.7, these numbers were not significantly different from the expected population norm (P = 0.197). Five physicians (6.3%) had high EE and high DEP and low PA, whereas in 25 subjects (31.3%) two out of three MBI dimensions corresponded to a high BOS. All subjects with high levels of burnout, based on the score of any of the three dimensions, constituted the high BOS group, whereas the rest of the subjects were the non–high BOS group.
Baseline differences in sociodemographic data, occupational data, habits and leisure time between the two groups (high BOS and non–high BOS) are presented in Table 1. Data regarding the level of anxiety, job satisfaction and physicians’ feelings regarding specific work-related circumstances are presented in Table 2.
Sociodemographic, occupational and leisure time data among physicians with and without high burnout.
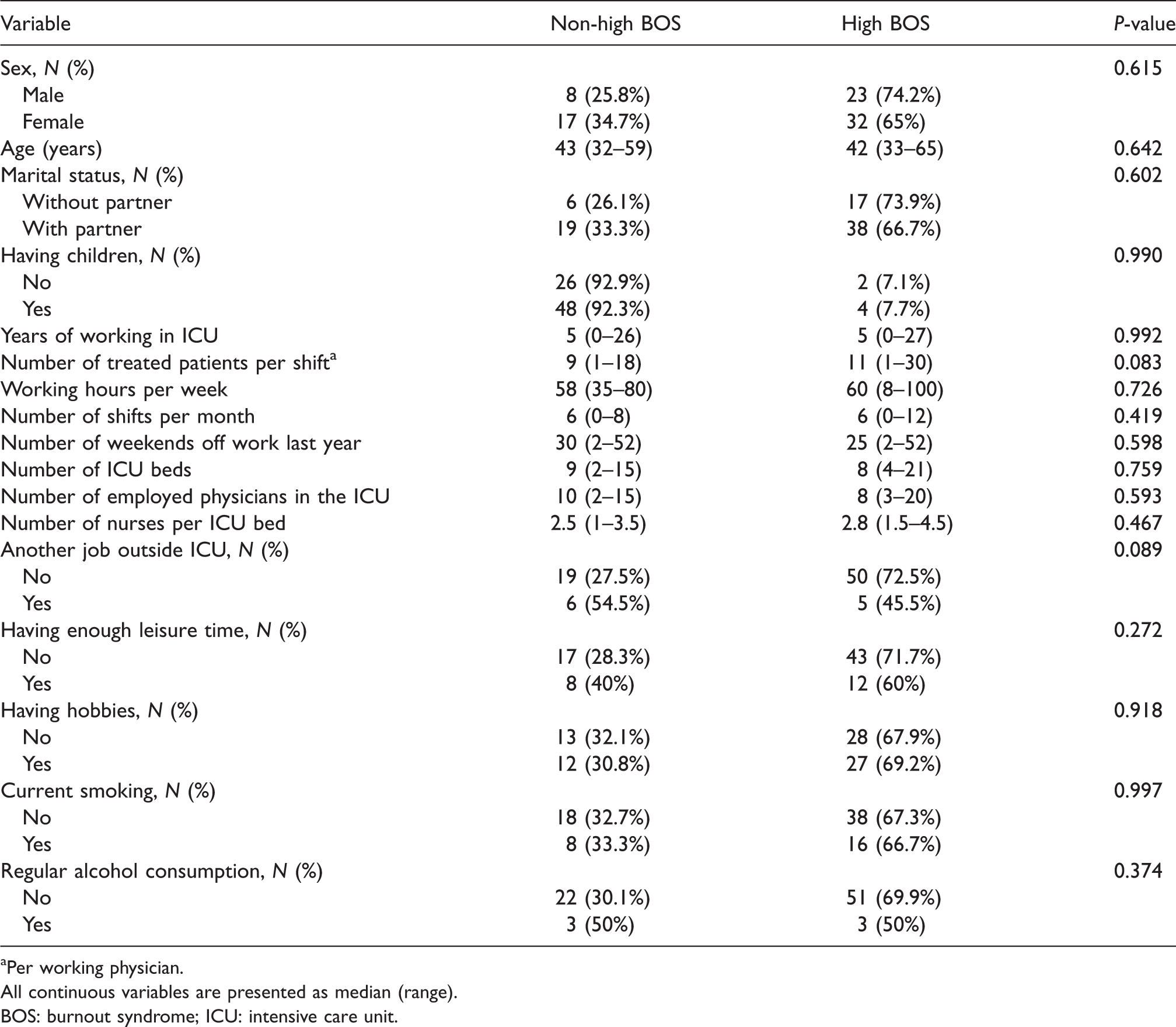
Per working physician.
All continuous variables are presented as median (range).
BOS: burnout syndrome; ICU: intensive care unit.
State and trait anxiety, job satisfaction and physicians’ perceptions on specific work-related conditions.
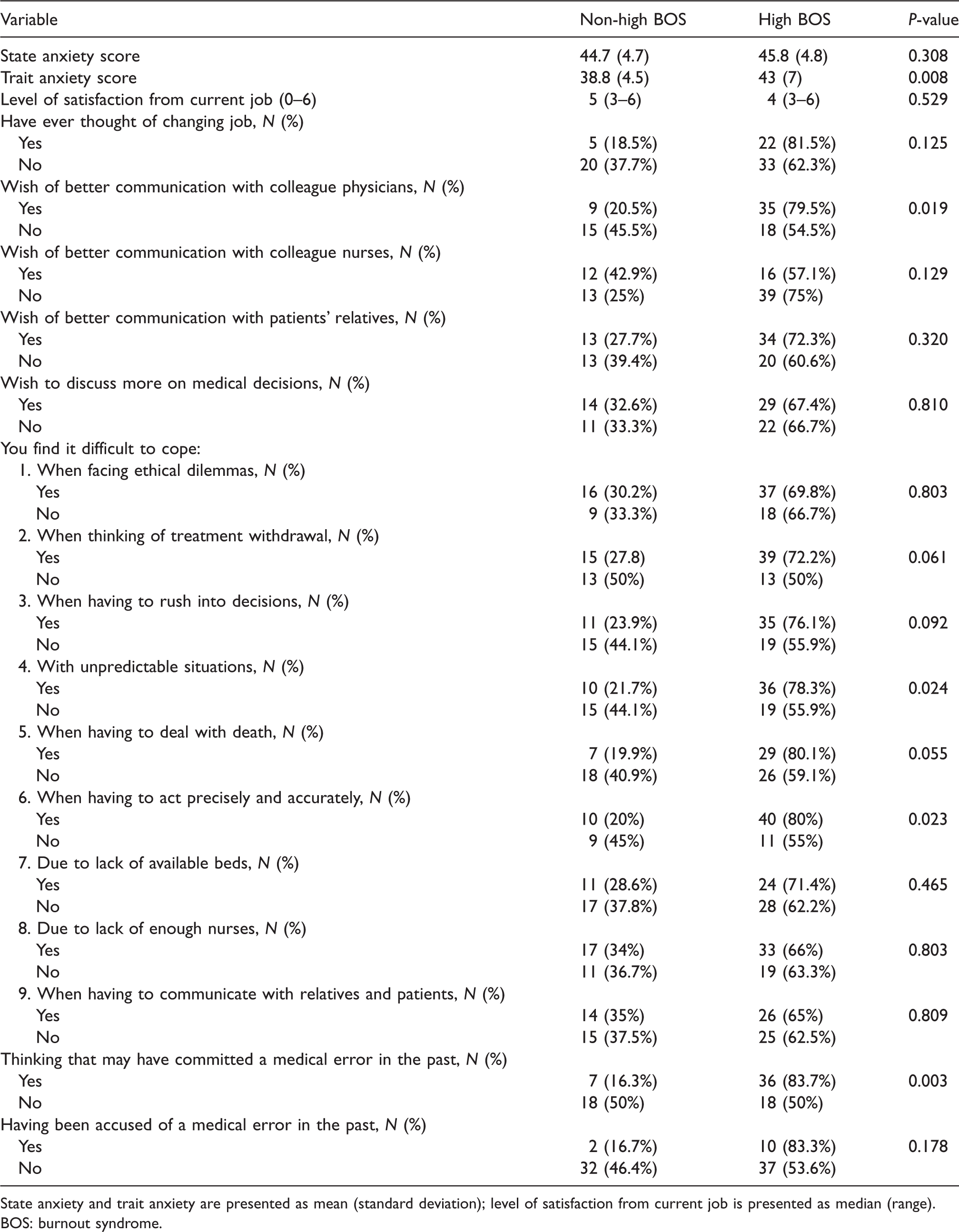
State anxiety and trait anxiety are presented as mean (standard deviation); level of satisfaction from current job is presented as median (range).
BOS: burnout syndrome.
Overall, physicians who had high (or low for PA) score in any BOS dimension were no different in terms of age, sex and marital status. Most working conditions were also similar because the numbers of ICU beds, employed nurses per ICU bed, treated patients per shift, working hours per week, weekends off work per year, shifts per month and number of employed physicians did not differ. Leisure time, hobbies, smoking and alcohol consumption were also similar between the groups (Table 1).
In terms of stress, although the state anxiety score was similar, trait anxiety was significantly higher in the high BOS group (43 (7) versus 38.8 (4.5); P = 0.008), compared to the rest. A larger proportion of physicians in the high BOS group wished that communication with colleague physicians (P = 0.019) was better. Moreover, they reported more frequently that they find it difficult to cope when they have to deal with unpredictable situations (P = 0.024) and when they have to act precisely and accurately (P = 0.023), whereas a significantly larger proportion of physicians in the high BOS group think they may have committed a medical error in the past (P = 0.003) compared with physicians with non–high BOS (Table 2).
Univariate and multivariate predictors of BOS
Table 3 presents all variables that were univariately associated with high BOS, with corresponding ORs. These five variables—STAI trait anxiety score, thinking of having committed a medical error in the past, wishing of better communication with colleague physicians, difficulty to cope with unpredictable situations, and difficulty to cope when having to act precisely and accurately—were all then included in the final binary logistic multivariate regression model.
Variables univariately associated with high burnout. a

All odds ratios have been calculated for the group yes versus no (as reference group).
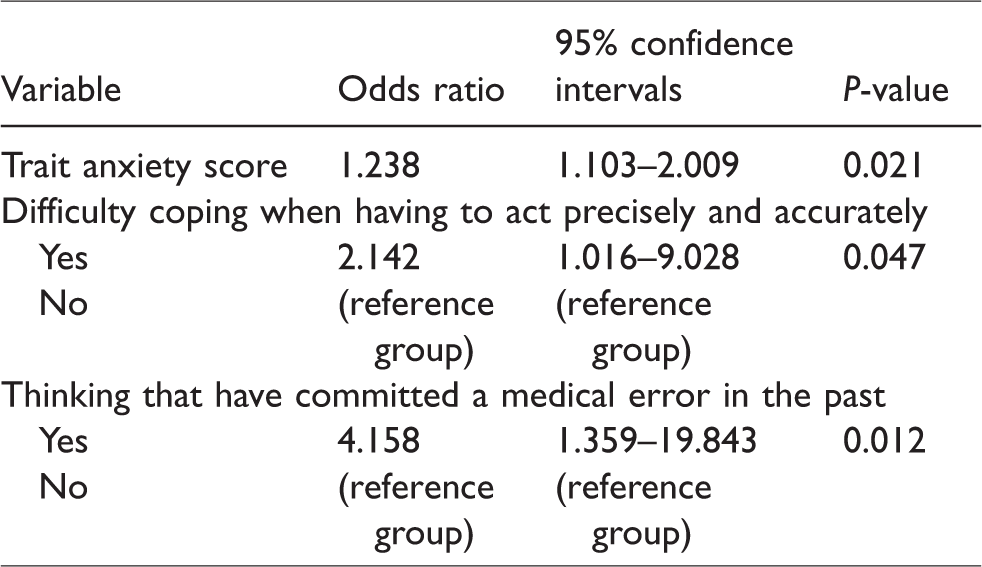
The Nagelkerke R Square of this model was 0.372. The three variables that were found to be independently associated with high BOS among ICU physicians were trait anxiety (STAI Y-2 score) (OR = 1.238; P = 0.021), difficulty to cope when having to act precisely and accurately (OR = 2.142; P = 0.047), and thinking of having committed a medical error in the past (OR = 4.158; P = 0.012) with the latter posing the strongest association (Table 4).
Independent predictors of high burnout in the final multivariate regression model.
Correlations between STAI sub-scores and dimensions of the MBI
The Pearson correlation was adopted to investigate the association between the state anxiety, the trait anxiety and each of MBI dimensions in the total population. Correlations between state anxiety and EE (r = −0.71, P = 0.549), DEP (r = 0.176, P = 0.128) and PA (r = −0.113, P = 0.337) were not significant. Trait anxiety was not correlated to DEP (r = 0.146, P = 0.207) and PA (r = −0.113, P = 0.337); however, the correlation between trait anxiety and EE dimension was significant (r = 0.472; P < 0.001) (Figure 1). This correlation remained significant when the analysis was repeated in the subpopulation of physicians with a high BOS (r = 0.478; P = 0.001).
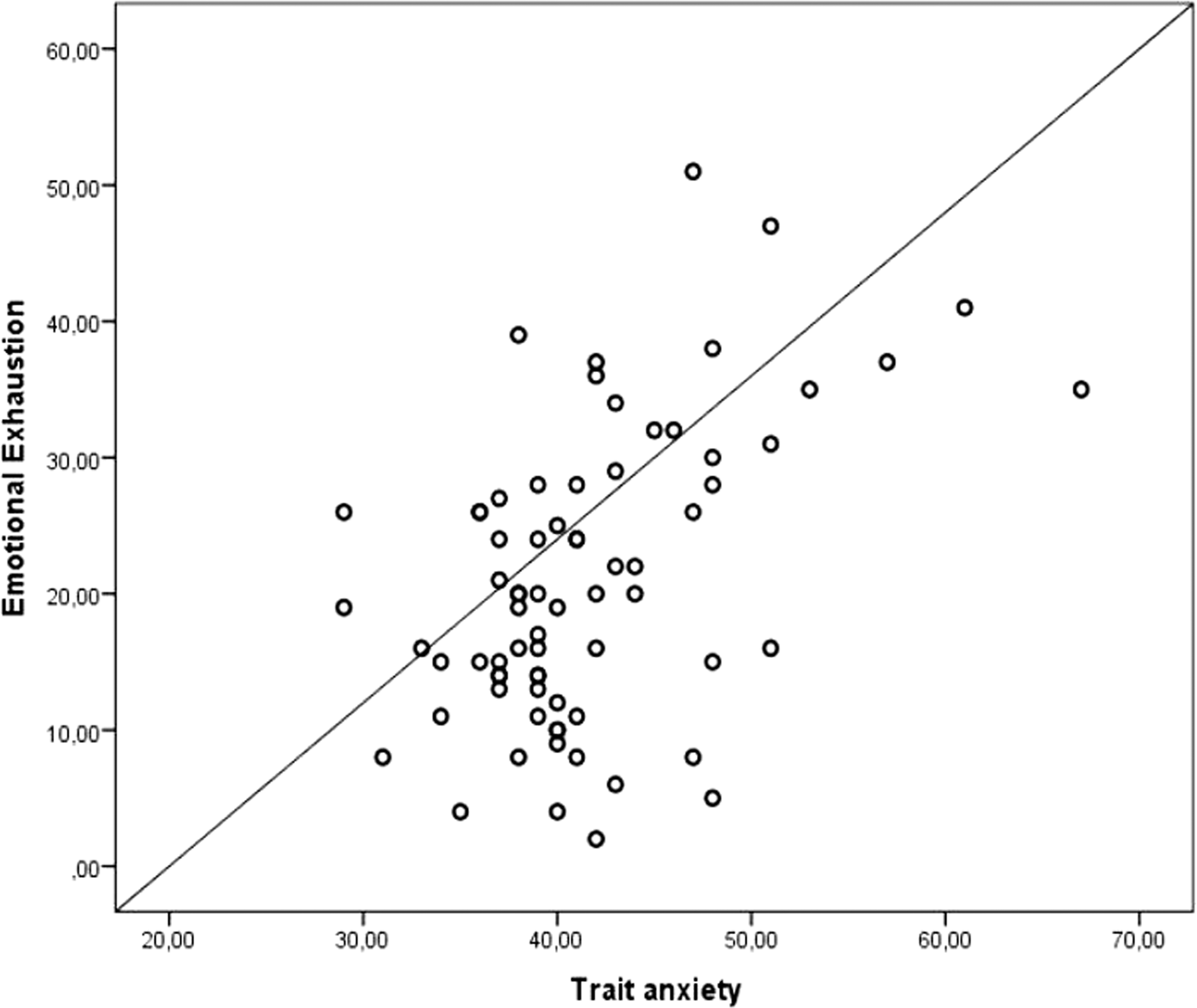
Correlation between emotional exhaustion and trait anxiety score, in the total population.
Discussion
In this cross-sectional multicentre study, approximately 27% of ICU physicians presented with high EE, 37.5% with high DEP and 41.5% with low PA; however, this prevalence was within the expected range for this population. The presence of a high BOS was associated only with behavioural and psychological characteristics, that is higher trait anxiety, difficulty when having to act precisely and fear of having committed a medical error in the past, whereas no sociodemographic or occupational factor was associated with a high BOS in the multivariate analysis.
The prevalence of BOS among ICU physicians varies widely in published literature, ranging from approximately 35% 25 to over 90%. 26 Several reasons can be identified for this discrepancy and conducting studies in various countries, which are characterised by several differences in the organisation of health systems, is one of them. Limitation of health resources, differences in the availability and the level of experience of ICU physicians and dissimilarities in their overall working environment could partially explain this variation in BOS incidence. 27 However, the most important reason for this discrepancy is probably the variable tools, especially definitions, that have been previously used to diagnose its establishment. Although the MBI remains the most frequently applied tool for the diagnosis of BOS, published studies have used a variety of different cut-offs for the three MBI dimensions. Moreover, the MBI authors originally designed the tool with burnout subscale scores reported as a continuum; 23 however, the presence of BOS has been analysed as a dichotomous variable in several studies, making comparisons between studies difficult and even unreliable. 27 In our study, the cut-offs for MBI-HSS have been applied according to the manual and the incidences of a high score in EE and DEP or a low score in PA are reported separately, confirming the findings of other studies that adopted similar methodology.6,28
In our study, trait anxiety was positively associated with the presence of a high BOS, in multivariate analysis. Moreover, trait anxiety correlated linearly with EE, which is the core symptom of BOS. It has been previously reported that anxiety levels are higher in healthcare professionals, compared to the general population, resulting from frequent night-time working, with few hours of sleep and exhausting workloads, among other causes.18,19 Moreover, Mark et al. 17 found that job demands, extrinsic effort and over-commitment were associated with higher levels of anxiety in a population of nurses. In another study among healthcare workers, 16 the emotional exhaustion and cynicism subscales were positively related to anxiety symptoms, whereas professional efficacy was negatively related to them. Similarly, Turnipseed et al. 14 found that burnout and anxiety symptoms are significantly correlated with each other, with the stronger link between anxiety and emotional exhaustion; our study confirms these findings. According to a most recent meta-analysis there is a definite association between burnout and anxiety, but no conclusive overlap between these two entities; 11 this would mean that burnout, apart from a psychological syndrome per se, is accompanied by the presence of other psychological disorders, such as increased anxiety, probably resulting in magnified effects on mental and psychological health.
The factor that established the stronger association with a high BOS in our study was the fear of a medical error having being committed in the past. In agreement with our results, a previous study among emergency medicine professionals identified the fear of medication errors as a significant risk factor for PA, 29 whereas in a large nationwide study among United States physicians, major medical errors were independently associated with burnout. 30 It is most interesting that the fear of medical error was based on the physician’s perception because the percentage of physicians who were officially accused of malpractice was similar between the two groups. Whether this behaviour is indicative of a loss of self-confidence because of BOS, as has been previously indicated among nurses, 31 is a hypothesis that needs to be further studied.
Another factor that was independently associated with a high BOS was the reported difficulty to act accurately and precisely. It has been reported that self-efficacy is negatively associated with emotional exhaustion among physicians, 32 whereas Wang et al. indicated a significant association between emotional labour and clinical performance among interns and residents. 33 Working in an ICU is a demanding task that often engages life or death decisions that have to be taken accurately and in a hurry. Although a more in-depth evaluation of the medical skills of the studied physicians was not carried out, the results suggest physicians with BOS may feel less capable to fulfil their tasks in regard to patient care.
The cross-sectional nature of our study may reflect just a ‘snapshot’ in the association between high BOS and anxiety, as there may be fluctuations in the working experience of the participants; a longitudinal study could have further elucidated the link between BOS and anxiety in the ICU setting. However, this cross-sectional design has been repeatedly used in similar published studies in the field.34,35 A strength of our study is that it was conducted in general ICUs of similar structure, so variations regarding different type of treated patients and various workload were minimised. Moreover, in Greece and Cyprus both residents and consultants employed in ICUs are already specialists in another medical field, so variations in medical skills and experience that could potentially impact the results are minimum. The sample size is relatively small, but the response rate was satisfying and similar to other studies in the field. A study limitation is that no formal questionnaires were provided to assess physicians’ medical and social skills and whether they are affected by BOS, as this was not included in the study aims.
In conclusion, in our study high burnout was found to be quite common among intensivists. The fact that personality traits and behavioural characteristics, rather than sociodemographic and occupational variables, were independently associated with its establishment indicates that improving the working environment may not be sufficient for its prevention; instead, early recognition of the group of physicians at risk of developing BOS and offering them the proper behavioural and psychological support may be more efficient. Further work is needed to identify the optimum intervention, when it should be initiated and how long it should last, so the incidence and adverse effects of this syndrome can be minimised.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.