
Abstract

Diabetic ketoacidosis (DKA) associated with sodium-glucose cotransporter-2 inhibitors (SGLT2i) can present with either elevated blood glucose levels or near normal to low blood glucose levels which is described as euglycaemic diabetic ketoacidosis (EDKA). 1 We analysed the spontaneous adverse event reports from the Australian Government Department of Health Therapeutic Goods Administration (TGA) where SGLT2i were suspected as contributing to the occurrence of DKA in surgical patients. A search of the TGA Database of Adverse Event Notifications (DAEN) for reports of SGLT2i-associated DKA was undertaken up until October 2018. We categorised EDKA as blood glucose level (BGL) <14 mmol/l, and DKA as BGL >14 mmol/l. 1
Of the 321 SGLT2i-associated DKA notifications, 53 (16%) occurred in the surgical setting. Three were in the context of emergency surgeries (one coronary artery bypass grafting and two unspecified). The remaining reports were presumed elective (Table 1). In 44 cases, where the specifics of surgery were known, 12 were cardiothoracic and six were bariatric procedures. Of the 20 notifications which specified the type of diabetes, all were listed as type 2 diabetes. Testing for anti-GAD/glutamic acid decarboxylase autoantibody (GADA) and islet tyrosine phosphatase 2 antibody were reported in two cases to rule out type 1 diabetes, and were not detected.
Demographic and disease features of surgical patients notified with diabetic ketoacidosis as an adverse event with sodium-glucose cotransporter-2 inhibitors.
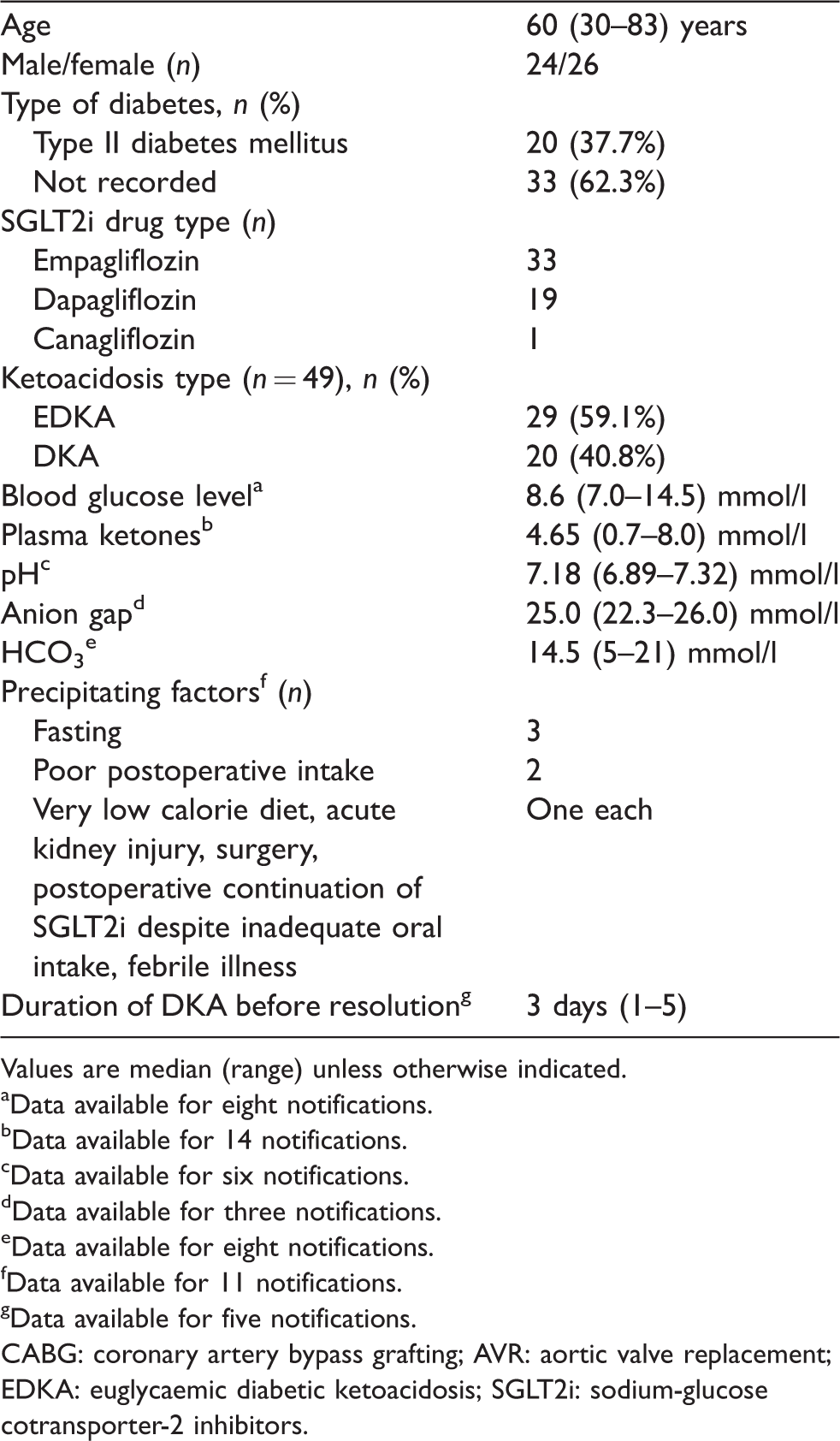
Values are median (range) unless otherwise indicated.
aData available for eight notifications.
bData available for 14 notifications.
cData available for six notifications.
dData available for three notifications.
eData available for eight notifications.
fData available for 11 notifications.
gData available for five notifications.
CABG: coronary artery bypass grafting; AVR: aortic valve replacement; EDKA: euglycaemic diabetic ketoacidosis; SGLT2i: sodium-glucose cotransporter-2 inhibitors.
Data on time to presentation was available in 33 reports. This varied from preoperatively (n = 2), during surgery (n = 2) and up to three weeks postoperatively (n = 28). Two cases were identified within the operating room; one occurred during elective coronary artery bypass grafting (CABG) in a case where the SGLT2i was ceased the day prior and another for an unspecified emergency surgery where the drug could not be withheld prior. EDKA occurred twice within the same individual after emergency CABG surgery: the first episode on day 1 postoperatively, the same day the SGLT2i was ceased, followed by a second episode on day 5 postoperatively when the SGLT2i was reintroduced. Information on the perioperative SGLT2i management was limited from the DAEN reports. SGLT2i medication was withheld on the morning of surgery in two reports, the day before in one report, three days before in two reports and for an unknown duration preoperatively in one report. SGLT2i were not ceased preoperatively in seven cases, two of which were emergency cases. The event presented on day 1 postoperatively in three cases and on day 4 in one case. Data on SGLT2i management post event was missing in all seven reports. Five reports mentioned continuing SGLT2i postoperatively, for up to four days in one report.
Symptoms at presentation included nausea, vomiting, tachycardia, abdominal pain, altered mental status, poor oral intake, malaise and presyncope. Symptoms resolved over 48 hours upon cessation of the drug and treatment of DKA/EDKA. Only three reports listed HbA1c levels; these ranged between 6.6% and 9.0% (48.6–74.9 mmol/mol).
Seventeen cases reported insulin treatment (intravenous in 14 cases, unspecified route in two cases and subcutaneous in one case), and nine noted intravenous dextrose infusion. One case required inotrope and vasopressor support. Full recovery was reported in 19 cases, whilst eight cases were notified during ongoing management. Acute kidney injury was reported in two cases; hepatic failure and hospital-acquired pneumonia were reported in one case each. One death was reported. This occurred in the context of liver failure, and the notifiers felt that the mortality was not directly attributed to SGLT2i exposure.
EDKA appears to be the more common presentation in the surgical setting, which is in line with the primary literature. 1 SGLT2i-associated DKA can present during the surgical procedure—a key finding that has not been previously reported. 1 Hence, a high index of suspicion is essential during major surgeries with unexplained acid–base disturbances. Cardiothoracic (n = 13) and bariatric procedures (n = 6) were found to have a higher chance for developing this adverse event.
It is approximated that an SGLT2i-associated DKA episode occurs for every 1000 patient years. 2 However, in the perioperative setting, the event rate remains unknown. In the perioperative period, identifying ketoacidosis—especially when BGL <14.0 mmol/l—is challenging due to differential diagnoses in this patient group, particularly if blood/capillary ketones are not performed. In the absence of symptoms, it is possible to overlook the presentation in the context of unexplained acidosis during surgery. Furthermore, symptomatic presentations may mimic that of an acute postoperative state or postoperative ileus. There have been reports of unnecessary advanced radiological imaging 1 and negative diagnostic surgical intervention 3 undertaken in the postoperative period when the diagnosis of DKA was initially missed. Hence, the monitoring of capillary ketones at regular intervals to identify significant ketonaemia is vital during the perioperative period. A recent editorial has reviewed the perioperative diagnosis and the management (elective and emergency) approach of patients who are on SGLT2i therapy. 4 A nuanced approach 5 ‘matching the fast’ before and after surgery together with strategies in managing combined prescriptions (e.g. SGLT2i and metformin) for patients with poor glycaemic control and those presenting for complex cases would improve perioperative outcome.
It is likely that a large number of SGLT2i-associated DKA cases remain unreported, and the data presented are an under-representation. A second limitation was that the detail provided within the TGA case reports was variable and sometimes incomplete and largely dependent on who was generating the report (e.g. doctor, pharmacist, drug company or member of the public).
Pre-approval clinical trials are usually underpowered to detect safety signals, as they focus on efficacy in a relative small healthy cohort for a shorter duration (less than 12 months). 6 As safety endpoints are seldom predetermined in Phase III clinical trials, they are weak in identifying uncommon adverse events (incidence of <1:1000). 6 Databases such as the DAEN, EudraVigilance from the European Medicines Agency and the US Food and Drug Administration Adverse Event Reporting System are valuable resources in evaluating post-marketing adverse events emerging in the real world.
Until the true risk in surgical patients is defined, knowledge and vigilance are important to mitigate risk, especially as these SGLT2i-associated DKA events are largely avoidable, particularly in the setting of elective surgery. Society and hospital-based guidelines on the management of SGLT2i in the perioperative setting are helpful in guiding clinical management. Reporting of these adverse events should be encouraged to clarify the risks and benefits of these medications.
Footnotes
Acknowledgements
The authors would like to thank Dr Richard Hill, Medical Officer of the Signal Investigation Unit, Pharmacovigilance and Special Access Branch of the Australian Government Department of Health Therapeutic Goods Administration, for his assistance in retrieving the reports and critical review of the manuscript. Emily Meyer undertook this project whilst holding a Royal Adelaide Hospital AR Clarkson Scholarship. Part of the data has been presented at the recently concluded Australasian Diabetes Congress in Sydney (August 2019).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.