
Abstract

Perioperative medicine involves a range of medical specialists, including anaesthetists, physicians and surgeons, and is expanding in response to the increasing need to prevent and manage postoperative complications. 1
There have been few attempts to quantify the future burden of postoperative complications. However, data from the extensively validated American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database and risk prediction tool 2 , 3 and data on Australian population projections 4 provide an opportunity to estimate the future changes in Australia.
For example, using colonic resection (Hartmann’s procedure), a procedure with a relatively high prevalence and complication rate, and a known response to optimal postoperative treatment, NSQIP 30-day predictions of the probability of readmission, serious postoperative complications, length of stay and death were calculated. The hypothetical patient was male, with hypertension and an American Society of Anesthesiologists (ASA) score of 2, and in the age brackets 65–74 years, 75–84 years and ≥85 years. These calculations show a substantial impact of age on complications, especially for death (see Figure 1). The predicted increases in the Australian population numbers in these age brackets between 2017 and 2047 are 150%, 220% and 300% for the three age groups, respectively. 4 As a result of both the increased population numbers, and the shift towards older age, it can therefore be expected that the burden of these postoperative events will increase substantially. Figures for other surgery types can be calculated, and also show large age-related effects.
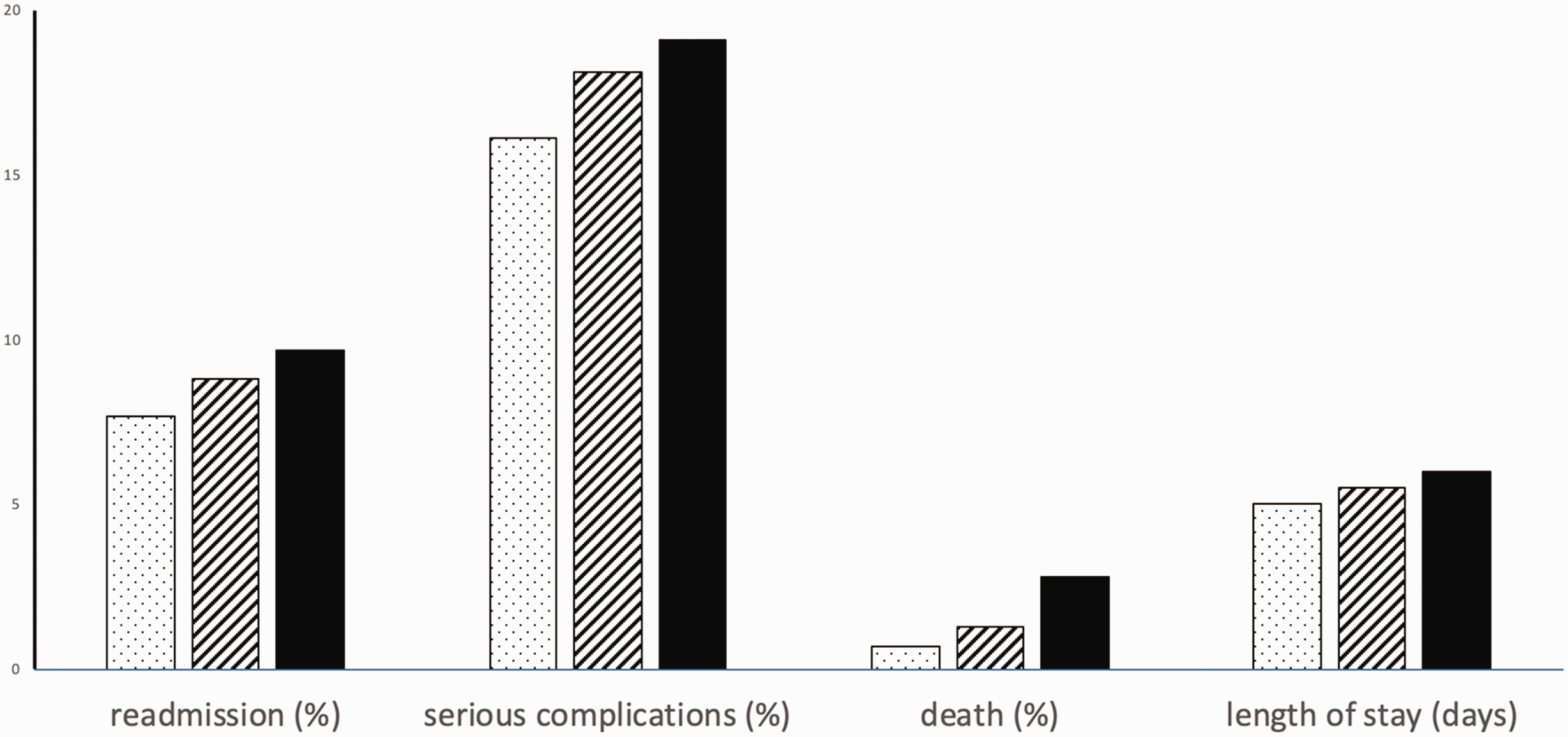
Postoperative events after Hartmann’s procedure predicted by the National Surgical Quality Improvement Program (NSQIP) risk prediction algorithm 3 for theoretical patients with hypertension and an American Society of Anesthesiologists score of 2, and in the age brackets of 65–74 years (dotted bars), 75–84 years (striped bars) and >85 years (solid bars).
These estimations include numerous assumptions, such as that surgery types will remain unchanged, that perioperative outcomes will remain unchanged and that surgeries are provided with equal frequency across age brackets. Importantly, it assumes the health of the population (the incidence of other co-morbidities) remains unchanged, which is optimistic and suggests the figures are an underestimate. For example, for the patient >85 years who now has an ASA of 3 and diabetes, readmission rates change from 9.7% to 15.6% and mortality changes from 2.8% to 9.3%. However, these figures at least draw attention to the need to consider this issue in future planning of workforce, training and hospital capacity in perioperative medicine.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.