
Abstract
In a ‘can’t intubate, can’t oxygenate’ scenario, success of emergency front-of-neck access is dependent upon a clinician’s skill, competence and confidence to initiate the procedure. Surgical cricothyroidotomy is an important airway skill, as it can be employed as both the primary method of emergency front-of-neck access or as a rescue approach if a needle technique should fail. We designed a collaborative surgical and anaesthetic training package to address perceived anaesthetic reluctance to perform surgical cricothyroidotomy and undertook a pilot study of the package using a mixed-methods approach. The package consisted of three elements: theory teaching, surgical experience and repeated high-fidelity simulation. Ten anaesthetic trainees were trained using the package. Training comprised face-to-face tuition on the 2015 Difficult Airway Society guidelines, the Vortex cognitive aid, manikin-based surgical cricothyroidotomy instruction and surgical experience gained from an elective surgical tracheostomy. A standardised, high-fidelity in situ ‘can’t intubate, can’t oxygenate’ simulation was used to assess performance at baseline and at two weeks and six months after training. Participants scored their self-efficacy, underwent qualitative semi-structured interviews and had their performance quantitatively assessed to evaluate this training. Six months following training, participants’ performance had improved. They reported significantly increased self-efficacy and demonstrated significantly reduced deliberation time to initiate surgical cricothyroidotomy in the simulated ‘can’t intubate, can’t oxygenate’ emergency. Thematic framework analysis of interview transcripts revealed that reluctance to perform surgical cricothyroidotomy was related to fear and anxiety in regard to performing the procedure. These results support wider adoption of collaborative educational training packages, including hands-on surgical teaching, to improve trainees’ efficacy and confidence with surgical cricothyroidotomy and front-of-neck access in an emergency ‘can’t intubate, can’t oxygenate’ scenario.
Introduction
The ‘can’t intubate, can’t oxygenate’ (CICO) scenario is an anaesthetic emergency that requires emergency front-of-neck access (FONA) to avoid patient death. For FONA, international guidelines recommend surgical cricothyroidotomy (SCT) either as the primary procedure 1 or as a rescue procedure if initial needle or guide-wire cricothyroidotomy fails.2–5 In the UK, the 2011 National Audit Project Four (NAP4) revealed high failure rates for narrow-bore and wide-bore needle FONA techniques, frequently requiring rescue using the surgical technique. 6 Consequently, the Difficult Airway Society (DAS) revised their UK guidelines for unanticipated difficult airway management, advocating SCT as the preferred method of emergency FONA. 1 This guideline was subsequently adopted by head and neck surgeons in the UK on the basis that a simplified consensus approach would reduce operator indecision in an emergency. 7
Although SCT is considered the fastest way to secure the airway, an anaesthetist may be reluctant to perform SCT.7–11 Regular, well-designed airway management training is crucial to acquire and retain the technical skills and confidence to initiate emergency SCT.1,6,11–13 Developing anaesthetic confidence to execute a time-critical, life-saving surgical procedure when clinicians may have had no hands-on surgical experience since medical school is challenging. 11 Greenland et al. have previously suggested that Australian anaesthetists address this deficit by scrubbing to assist with routine, simple surgical procedures—ideally, elective tracheostomies. 11
To improve both the technical ability and confidence of trainee anaesthetists to undertake SCT as part of a CICO emergency, the Departments of Anaesthesia and Maxillofacial Surgery at Aintree University Hospital collaborated to develop a training package combining hands-on surgical teaching with instruction on the DAS 2015 guidelines 1 and the Vortex cognitive aid. 14 The surgical training element provides experience of assisting in an elective tracheostomy (e.g. patient positioning, surface anatomy of the neck, use of a scalpel, feel of neck tissues, bleeding and depth of trachea relative to skin) to develop basic surgical skills to augment ‘standard’ anaesthetic CICO training. Our aim was to evaluate this educational package to determine utility as a precursor to guide potential wider adoption.
Methods
We followed the principles of the UK Medical Research Council (MRC) framework for the development and evaluation of a complex intervention, with an initial pilot phase before an intervention trial.
15
An essential aspect of the pilot phase is to identify which elements of an intervention are useful. Therefore, we took a structured longitudinal approach to evaluate our training intervention using a mixed-methods approach. The study protocol and evaluation have been set out using the Template for Intervention Description and Replication guidance for intervention description and replication
16
:
Self-efficacy scoring (confidence) of managing a CICO emergency.
17
Qualitative assessment of the educational package and participants’ confidence managing a CICO scenario explored using structured interviews and thematic framework analysis.
18
Quantitative measurement of how quickly participants performed SCT in a simulated CICO scenario. Quantitative measurement of how participants managed the CICO emergency with respect to the DAS 2015
1
and Vortex
14
guidance.
Participants
We recruited a cohort of ten anaesthetic specialist trainees (years 5–7) with national training numbers as they rotated to Aintree University Hospital (AUH). Health Education England North West (Mersey) trainees complete their higher and advanced airway competencies at AUH, which is the regional tertiary referral centre for head and neck surgery. The only exclusion criterion was participant refusal. The study was reviewed and approved by the NHS Health Research Authority (16/HRA/4434) and Health Education England Research Governance (North West Office). All participants consented to emergency CICO training and simulation. They also agreed to undergo longitudinal semi-structured interviews for qualitative analysis, and to filming to facilitate quantitative assessment of their management of a simulated CICO scenario. The sample size of ten participants was chosen based on advice for minimal numbers for useability testing 19 and credibility of qualitative data collection and analysis.20,21
Intervention and assessments
The components of the intervention and assessments are described in Figure 1. After baseline semi-structured interviews and assessment of airway management skills, participants began the training package intervention (phase 1). The anaesthetic component was delivered by a consultant anaesthetist with airway expertise (PG) in phase 1, and it was revised in phase 2. This comprised of one-to-one teaching on the DAS 2015 guidelines, 1 the Vortex cognitive aid, 14 the laryngeal handshake, airway ultrasound and SCT training using a low-fidelity manikin.1,14,22,23 Participants were provided with a multimedia bundle consisting of the DAS 2015 guidelines 1 and Vortex, 14 a guide to airway ultrasound, instructional videos demonstrating the performance of SCT and website references of clinicians’ accounts of performing SCT.24–28 The surgical component was delivered in phase 2 by a consultant maxillofacial surgeon (SR). The participant became a directly supervised assistant for an elective tracheostomy, appropriately positioning the patient and marking out the surface anatomy of the neck. Crisis resource management behaviours were not taught as part of the package. To evaluate the utility of the training package, further assessments and semi-structured interviews took place in phases 3 and 4 of the study (Figure 1).
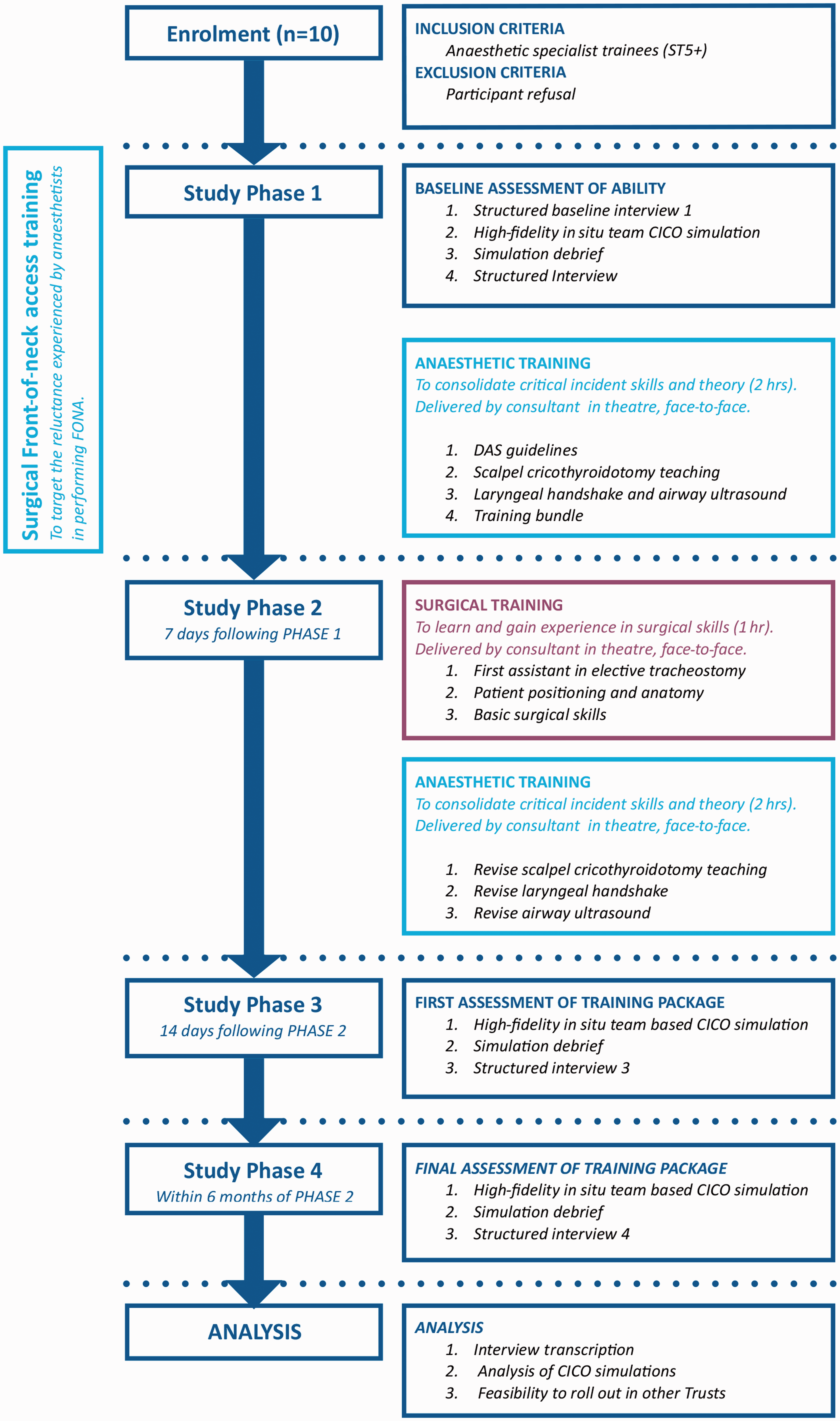
Study design. FONA: front-of-neck access; CICO: can’t intubate, can’t oxygenate; DAS: Difficult Airway Society.
Simulated CICO scenario design
To evaluate the training package, we developed a standardised high-fidelity scenario. This recreated a CICO emergency that arose after induction of anaesthesia in an otherwise healthy patient with a normal airway assessment. The scenario was performed in situ (anaesthetic room) and with clinical staff (operating department practitioner and healthcare assistant), as is standard practice in our hospital, and reproduced identically for simulations A, B and C. The scenario facilitators (HW, RB, WG and SM) used a standardised approved script to ensure identical conditions across each simulation. The same scenario facilitator controlled and filmed the scenarios from outside the anaesthetic room. Full details of the equipment used, standardised simulation and debrief are provided in the online supplementary Appendices 1 and 2. A TruMan Trauma X (TruCorp® Ltd, Belfast, UK) manikin was used for its superior airway attributes, incorporating a novel bleeding neck prosthesis to mimic a patient with an impalpable cricothyroid membrane. 29 This mandated a midline vertical incision according to the revised DAS guidelines. 1 Monitoring was provided remotely with SimMon (Castle + Andersen ApS) displayed on an iPad. In the simulation, participants were permitted to attempt facemask ventilation, laryngeal mask and endotracheal methods of oxygenation, but only FONA yielded positive capnography and resolution of oxygen saturation (both simulated by the faculty member).
Qualitative data
The qualitative aspect of the study was longitudinal by design, with each participant interviewed four times (SS). Interview 1 investigated baseline perceptions. Interview 2 looked at the change in baseline perceptions after managing a simulated CICO scenario. Interview 3 considered the change in perceptions after managing a simulated CICO scenario one week after completing the training package. Finally, interview 4 assessed perceptions towards managing a simulated CICO scenario six months after completing the training package.
At interview, participants were asked questions relating to their reflections on the training package and any perceived effect it had on their self-confidence and competence. Anonymised labels were assigned for participant, interview and quote (e.g. participant P2(1)). At the time of each interview, participants also rated their self-efficacy score for managing the CICO emergency. Each of the 40 interviews was transcribed verbatim. The essential steps of the thematic framework analysis approach were followed to identify key themes. 12 Researchers (JS and JB) independently read all the transcripts to familiarise themselves with the data to identify a thematic framework. Sections of text were indexed to the identified themes in the framework until all of the textual data had been gathered. An illustrative quote from the interview transcript was selected to represent each theme and labelled with interview and representative participant number. Throughout the process of analysis, any differences in the identification of themes and indexing were discussed between JS and JB until a consensus was reached. Involvement of two independent researchers (JS and JB) throughout the qualitative data analysis added rigour to the process.
Quantitative data
Our quantitative analysis was undertaken for exploratory purposes. Our sample size was selected for qualitative analysis only. Therefore, whilst we present exploratory statistical tests, there is a high risk of type II error. Video recordings were made of the three high-fidelity CICO simulations to assess performance of SCT. Our primary outcome was time to complete SCT. The secondary outcome was whether the SCT method employed was in accordance with the DAS 2015 guidelines. 1 We also assessed how the simulated emergency was managed prior to performance of the SCT with reference to the DAS 2015 guidelines 1 and Vortex cognitive aid. 10 In each simulation, we timed three phases of SCT: (a) deliberation time: time from declaration of a CICO scenario to initiation of the SCT; (b) surgical time: time from initiation of SCT to completion; and (c) total time: time from declaration of a CICO scenario to completion of the SCT.
CICO was defined as the declaration of an inability to oxygenate the patient via intubation, supraglottic airway device or bag–mask techniques. Completion of SCT was defined as manikin intubation via a neck incision. Successful insertion was signified by a return of simulated capnography and chest expansion. The latter was announced by the operating department practitioner, and then both were confirmed by the simulation facilitator. Time to completion was measured on video recording. In addition, correct placement was confirmed post scenario when the model was disassembled. Statistical analysis was performed with JASP v0.8.6 (JASP Team 2018, University of Amsterdam, Amsterdam, The Netherlands). Kruskal–Wallis and Wilcoxon signed rank sum tests were used to assess significance; for the small sample size, non-parametric tests were used.
Results
Self-efficacy scores
We found reported self-efficacy for managing a CICO emergency significantly improved at six months upon study completion (medians after simulation A 50%, simulation B 80% and simulation C 87.5%; P<0.001).
Thematic framework analysis results
Thematic framework analysis of semi-structured interviews with study participants is summarised in Figure 2. Theme saturation was achieved by six participants (24 interviews), and full saturation was found by nine participants, confirming adequate sample size. The quote provided for each theme represents a typical participant’s response.
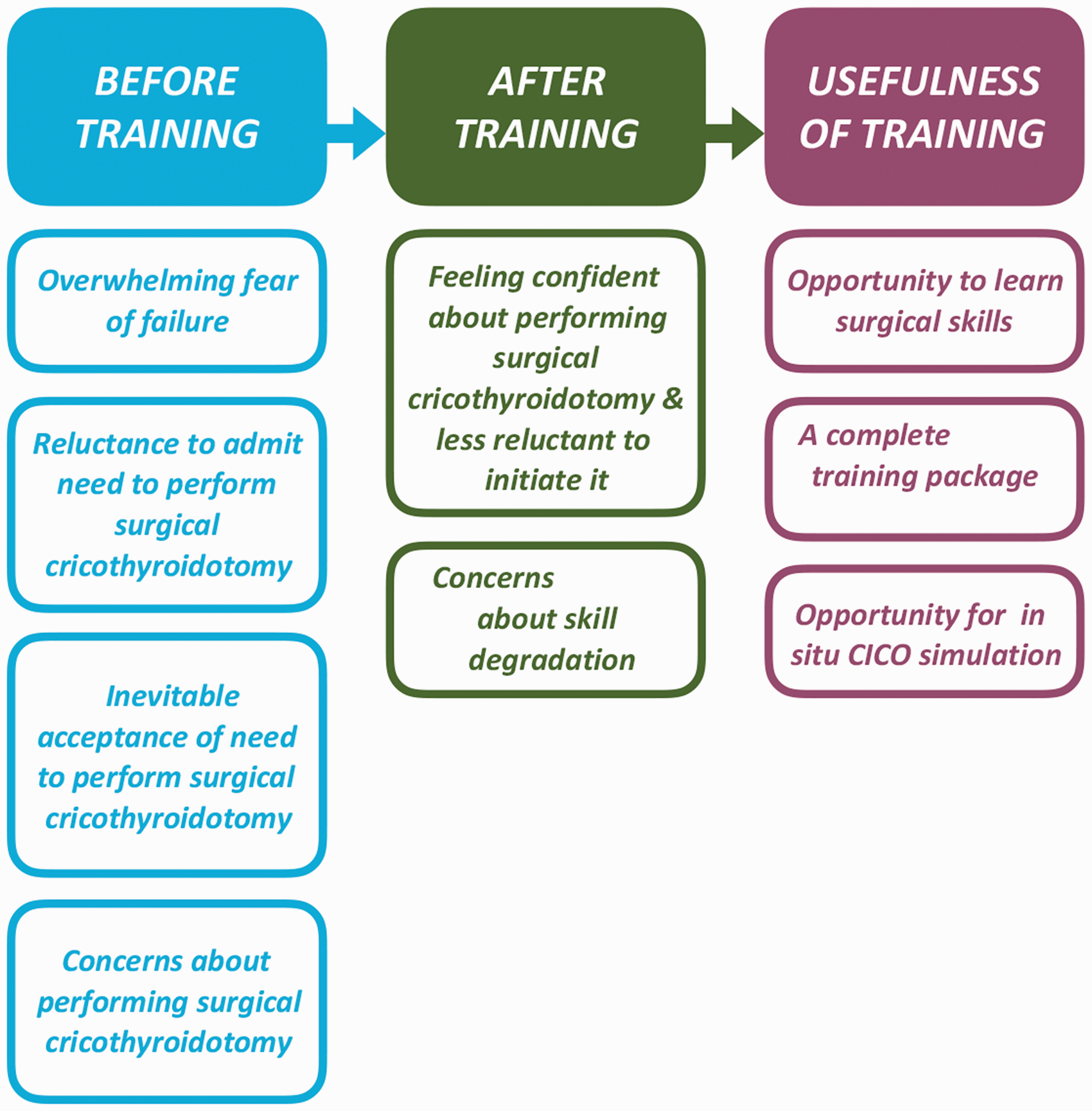
Thematic analysis of the Aintree training package.
Themes identified before completion training (interviews 1–3)
Subtheme 1: Feeling of failure
A key finding was a feeling of failure experienced by anaesthetists compounded by anxiety that their performance had contributed to the CICO scenario: It’s the sort of thing that you hope you would never have to see, but then, also hope that you would be able to manage … I’d be wondering, ‘Am I at this stage because I’m not doing a very good job at the initial steps?’ (Interview 1)
Subtheme 2: Reluctance to admit the need to perform SCT
We noted indecision to perform the SCT promptly due to self-doubt concerning management of the emergency: I think my initial thought would be ‘What else, or what have I missed? Is there anything I can do to avoid this?’ I think that sometimes the problem with the surgical [FONA] is the reluctance to finally pick up the scalpel. (Interview 1) I think my initial feeling would be panic … And I think my initial thoughts would be like, ‘I can’t believe this is happening to me, this isn’t ever really supposed to happen’. We’re trained for it, but … it’s very, very rare. (Interview 1) I don’t think we are programmed to accept failure, especially in something we do every day for how many years. In a way, you are letting yourself down if you can’t intubate that patient. In your mind, you are thinking, ‘Somehow I need be able to get a tube down’. (Interview 2) I think it’s just everybody is desperate to avoid ‘front of neck’, and anyone who says they’re not, is lying. (Interview 3)
Subtheme 3: Inevitable acceptance of the need to perform SCT
Despite low confidence from the lack of experience of performing this surgical procedure, SCT was accepted as an inevitable last resort: I have full confidence in myself, but confidence of my technique, having never done the procedure other than a manikin, would be significantly less. (Interview 1) I think the most difficult part, for me, would be making the decision that I need to go down that algorithm and put a knife to someone’s neck. I think once I’d made that decision, yes, it might be technically difficult, but I have done tracheostomies in ITU. (Interview 1)
Subtheme 4: Concerns about performing cricothyroidotomy
There was high anxiety about correctly performing SCT. The emotions encountered in dealing with an iatrogenic, potentially fatal situation had to be conquered: I would struggle to, I think, overcome the ‘emotions’ side of it …, trying to fight down the utter panic … and the real probability that this patient might die – and it really is my responsibility. (Interview 1) Knowing where to put the knife, especially if you can’t feel the anatomy – that’s probably the most difficult thing, but actually, there’s probably a lot of other difficult things like remembering to call a senior, getting the patient in the right position, staying calm, getting the right equipment, [and] doing it quickly, efficiently. (Interview 1)
Themes identified after training was completed
Subtheme 1: Feeling confident in performing SCT and less reluctant to initiate it
Trainees were satisfied with the development of their technical SCT skills: I’ve got to a stage where I’m really … happy with the technical bits. And I think it’s important to not let that go. Technical skills sort of go after time. (Interview 4) I’d feel less anxious about actually having to do [FONA] in real life, and less, ‘Oh God, is this actually happening to me?’ (Interview 4) I would definitely hesitate less … I think the period of time I’d spend hesitating would be less because … my technical skills in doing it have improved – because we’ve done so many repeated attempts. (Interview 4)
Subtheme 2: Concerns about skill degradation
Recognising the CICO emergency is rare, the repeated assessment simulations highlighted the importance of maintaining skills over time and offered participants the opportunity to develop their skills. You might not ever see [FONA] in your career at all, or you might only see it once. And so, I think, probably, regular training [is important]. (Interview 4)
Themes regarding usefulness of the training package
Subtheme 1: Opportunity to learn surgical skills
The surgical training was highly regarded by trainees. The benefit of ‘getting a feel’ of what it is like to incise a patient’s neck—the anatomical structures, fat, tissue planes and encountering bleeding, whilst performing the elective surgical tracheostomy—was noted. Doing the tracheostomy, or at least the initial incision and dissection, helped a lot: having a feel of the scalpel and the skin and … the tissues … I think helped me with … the technical bit of the procedure … So the actual tracheostomy made a huge difference. Actually, playing the role of the surgeon … Then … having a feel of the scalpel, having a feel of pressures and how you should actually feel when you’re dissecting tissue … and then also [the] feel [of] the trachea and the cartilages. It might give me a mental reminder … if I end up having to do an emergency airway. (Interview 3)
Subtheme 2: A complete training package
Besides the surgical element, the package employed one-to-one SCT manikin training, airway ultrasound and revision of the DAS guidelines
1
and Vortex.
10
Airway ultrasound was highlighted as a potentially useful prospective adjunct if a difficult airway was suspected (if available) but was not used during our high-fidelity simulations. Participants also received links to online instructional SCT videos and first-hand accounts from clinicians involved in real CICO scenarios. The whole package was considered useful: Going in to theatre and actually scrubbing in, and feeling the cricothyroid membrane, and assisting … surgeons in doing the procedure. I think that was really helpful, just to feel [the] anatomy. Doing lots of those would be beneficial. [The] private tutorial in the anaesthetic room, learning all the ways to polish the technique and the proper way to do it, and then actually getting to do it again [in the simulation, to] bed in that knowledge [was useful]. (Interview 4)
Subtheme 3: Opportunity for in situ CICO simulation
Trainees commented that the three high-fidelity simulations used to assess their performance were valuable, especially combined with the one-to-one training: ‘I think it was probably good to go through a ‘sim’ session in the first place, before any training, to identify which bits I struggle with. Going through the ‘sim’ and using the model both in the ‘sim’ scenarios and in the one-to-one teaching with [PG] was probably the most helpful for me’ (Interview 4) ‘I think we’ve had a lot of repetitive practice … It almost just flows now, like a robot.’ (Interview 4)
Quantitative data results
All ten anaesthetic trainees completed the training package, interviews 1–4 and simulations A–C. Video data on one candidate (P7) for simulation B was lost due to technical failure.
Total time for SCT significantly decreased from simulation A (median 225.0 seconds, interquartile range (IQR) 163.8–244.0 seconds) to simulation C (median 151.5 seconds, IQR 129.3–190.0 seconds; P = 0.002) but not at B (median 213.0 seconds, IQR 170.5–246.5 seconds, P = 1.0; Figure 3). This reduction from simulation A to C was due to a significant reduction in the deliberation time: simulation A (median 101.5 seconds, IQR 92.25–177.5 seconds) to simulation C (median 76.0 seconds, IQR 63.25–92.0 seconds; P = 0.027). As shown in Figure 3, the IQR H-spread decreased from simulation A to simulation C, indicative of improved consistency of trainee performance at SCT (total time IQR A: 80.2 seconds; B: 76.0 seconds; C: 60.7 seconds; deliberation time IQR A: 85.25 seconds; B: 58.25 seconds; C: 28.75 seconds; surgical time A: 56.8 seconds; B: 59.0 seconds; C: 44.05 seconds).
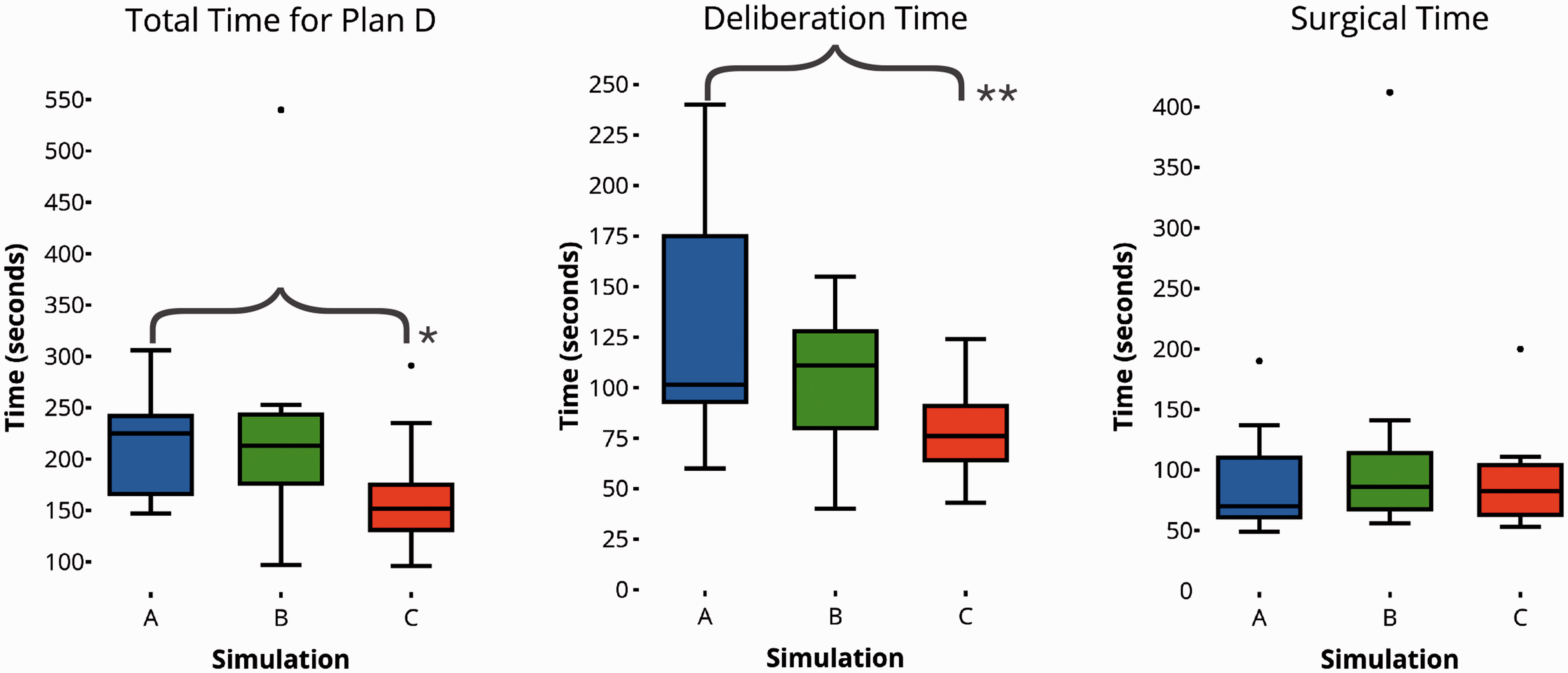
Plan D—quantitative data from simulations A–C. Between A and C, there is a significant reduction in the total time for plan D, which is attributable to a reduction in the deliberation time, not the surgical time. Significance assessed with Wilcoxon rank sum test. *P = 0.002; **P = 0.027.
The length of vertical incisions did not change across the study period (simulation A: 71.0 mm, IQR 60.75–81.5 mm; simulation B: 65.0 mm, IQR 47.5–75 mm; simulation C: 67.5 mm, IQR 63.75–77.0 mm). All were less than the recommended 8–10 cm suggested by the DAS. 2 There was a signal towards concordance with the recommended vertical surgical approach over time (simulation A 60%, simulation B 90% and simulation C 100%; n = 10), but this was not significantly different (P = 0.134). Video analysis of the conduct of managing the CICO emergency revealed that adherence to the stepwise progression set out in the DAS guidelines 1 from A to D did not alter from baseline to six months (A = 60%, B = 70%, C = 60%). Instead, plan B (attempt ventilation via a supraglottic airway device) and plan C (attempt facemask ventilation) were often switched around, possibly reflecting adoption of the Vortex approach. 10
Discussion
We have developed and evaluated a pilot collaborative surgical training package for anaesthetic trainees to prepare for SCT. We found that the delivery of anaesthetic theory and surgical tracheotomy experience was highly valued by trainees. Repeated high-fidelity simulations consolidated this knowledge and experience. These results support wider adoption of collaborative educational packages to improve trainees’ efficacy and confidence with SCT and FONA in an emergency CICO scenario. We recommend that in addition to standard theoretical teaching, CICO training programmes should consider including an element of hands-on surgical teaching, as well as the opportunity for anaesthetists to rehearse their skills in a high-fidelity simulation of the emergency.
Deliberation time, a surrogate for non-technical skill performance, was the rate-limiting step that our training package improved. The reduced total time to perform SCT successfully was due to a significant reduction in the deliberation time, not surgical time. This reduction was evident at six months but not two weeks, suggesting the improvement is attributable to cognitive reprocessing, with the participants learning from reflection and consolidation of their procedural knowledge and understanding. 30 Participants clearly described this aspect, informing us that they had considered where their performance could be improved.
Thematic framework analysis confirmed that before participation in the training package, performing SCT is associated with significant anxiety and reluctance to initiate SCT. After training, there was a statistically significant improvement in the participants’ deliberation time and reported self-efficacy. These findings were corroborated by the thematic analysis, with many participants reporting a reduction in anxiety and deliberation associated with performing SCT.
The quantitative analysis supported the development of improved performance, though this pilot was not designed to analyse results inferentially.
Reluctance to perform SCT is a multifaceted and nuanced phenomenon. We developed the following integrated model to describe the mindset of an anaesthetist contemplating performing SCT (see Figure 4):
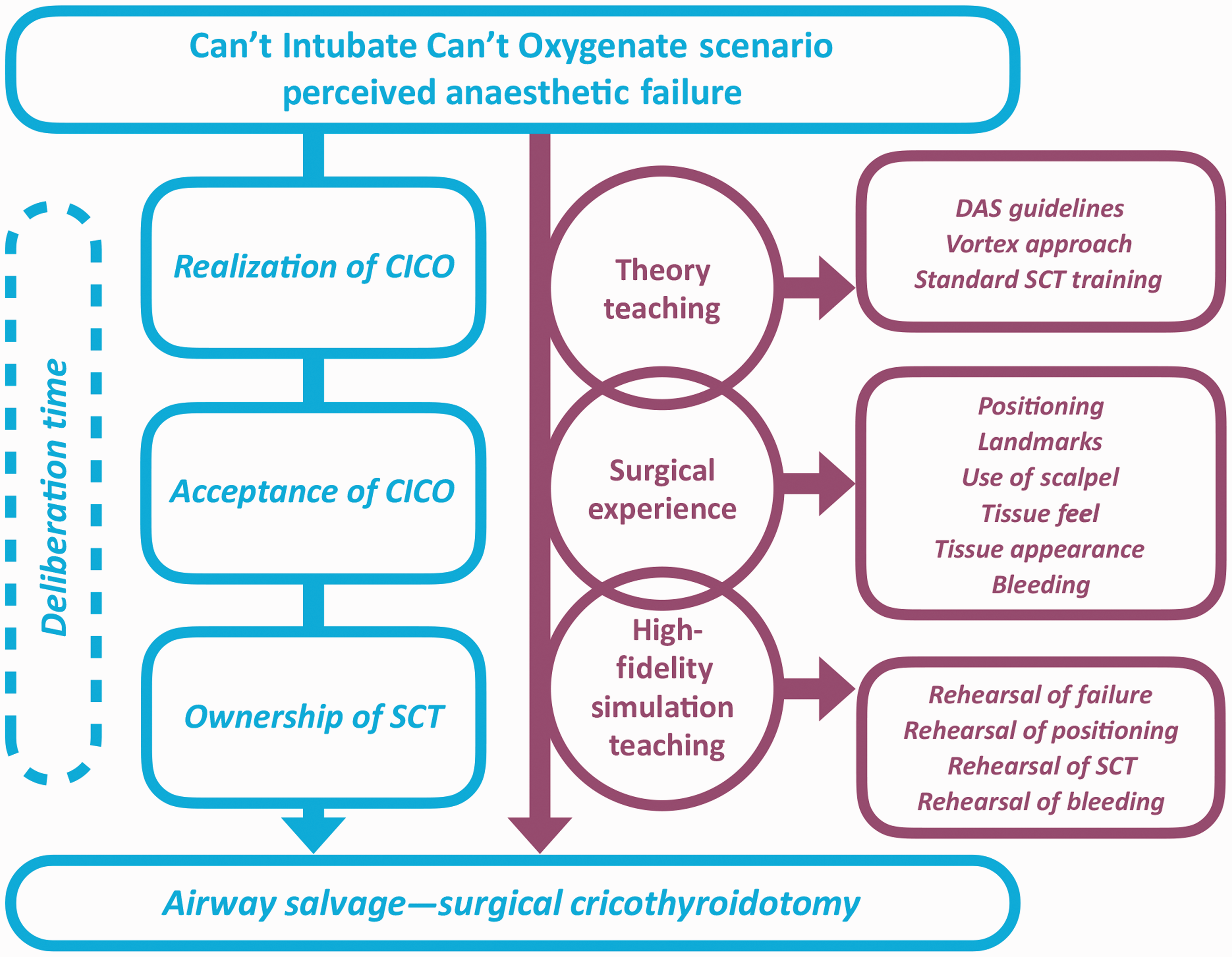
Model of how the training package may reduce reluctance to perform surgical cricothyroidotomy. DAS: Difficult Airway Society; SCT: surgical cricothyroidotomy.
Ownership of SCT—a hard-to-acquire surgical skill set.
Need for SCT perceived as a failure by the anaesthetist.
Acceptance of the perceived anaesthetic failure is a prerequisite to performing SCT.
‘Willingness’ equates to acceptance of failure and ownership of SCT.
The interviews highlighted the importance of practising and rehearsing SCT. Visualisation and rehearsal are effective learning tools known to improve performance in athletes and surgeons.31,32 By anticipating and visualising a CICO scenario and mentally rehearsing failure, participants were able to transcend the perceived non-ownership of a surgical skill to salvage the airway. The importance of mentally preparing, or ‘priming for FONA’ is increasingly well recognised.14,33 In our study, the effect of rehearsal and visualisation was reflected in the increased consistency (reduced IQRs) and speed with which SCT was performed over the six-month study period. We noted evidence of continued mental rehearsal months after the training in interview 4, with participants mentally preparing for FONA when it was a possible outcome.
At six months, participants reported significantly increased self-efficacy dealing with a CICO emergency. Participants valued the private tutorial that emphasised the ‘tips and tricks’ imparted by the one-to-one teaching format, as tacit knowledge was deemed important compared to that gained from the literature. 34 In teaching, emphasis was placed on the Vortex 10 for real-time use to manage a CICO emergency. The Vortex is a specially designed cognitive aid promoting a fluid approach to airway management, alleviating the cognitive overload encountered in a CICO emergency. 35 Serial video analysis of the simulations revealed that plans B and C were often executed out of order and did not improve with training. We believe this represents the participants’ adoption of the Vortex over strict adherence to a DAS 2015 plan A, B, C approach. It supports the logic behind the pragmatic approach of the DAS 2017 ITU guidelines 33 and their adoption of a Vortex method to the implementation of plans B and C. This sentiment was echoed by trainees in the interviews. We advocate that the DAS 2015 guidelines 1 are used in the classroom to teach the theory of CICO management and that the Vortex 10 is taught in the anaesthetic room to support real-time decision-making.
Based on NAP4, approximately 100 CICO events occur in the UK each year. 6 The NAP5 audit estimated that there were 2.7 million general anaesthetics given per year in the UK. 36 If we estimate that the typical anaesthetist administers 750 routine general anaesthetics per year, this equates to a risk of 1/36 per year. If an anaesthetic career lasts 30 years, then anaesthetists will experience on average about only one CICO event in their career. However, the risk of airway complications in settings outside of the operating theatre such as the emergency department or intensive care is likely to be much higher, as NAP4 demonstrated.2,37 It is ambitious to expect an anaesthetist with no prior surgical training to perform a life-saving SCT promptly, confidently and competently in a time-critical CICO emergency. This notion is expounded by Greenland et al. who highlight that whilst anaesthetists may lose situational awareness, a surgeon may be in no better a position to perform SCT. 11 Interview transcripts demonstrated the axiomatic principal of reluctance in SCT performance. Surgical experience was a highly valued aspect of the training package, and experience gained helping perform an elective surgical tracheostomy augmented traditional anaesthetic SCT training. Besides fostering the development of motor and sensory schemata for expertise at SCT, 38 surgical experience was important to improve self-confidence. Candidates especially reported benefit from the feel of live human tissue. In time-critical emergencies, pattern recognition is key, as there is little time for deliberation. 11
Although employed as an assessment tool, the high-fidelity simulations proved to be valuable, as these provided four opportunities for revision of the DAS 2015 guidelines, 1 Vortex 14 and experience of SCT. Specifically, the simulations provided participants with the opportunity to rehearse failing conventional anaesthetic airway management techniques before instituting and practising their SCT technical skills. Over time, the management of CICO became a more familiar and palatable experience for participants to perform SCT. McCrossin et al. previously explored training techniques for percutaneous airway access in a simulated CICO scenario. 39 Our study focused specifically on surgical FONA in standardised high-fidelity in situ scenarios working with multidisciplinary operating department staff. Our holistic methodology qualitatively and quantitatively examines what happens between declaration of CICO and the steps required to put knife to skin. We believe that our study offers insights beyond exploratory trainee confidence measures by highlighting the decision points that educators should target to improve clinician performance.
Limitations
Pilot studies are inherently limited by their sample size but are designed as an essential component to inform further experimental studies. 15 Routine, serial in situ simulations are an accepted way of assessing similar teaching packages, 40 but in our study, these inadvertently served as a training tool, embedding learnt skills into a realistic narrative to provide heuristic improvements. Familiarity may have contributed to the observed confidence increase and reduced deliberation time. However, participants remarked on the usefulness of the simulation in enhancing their learning experience during qualitative interviews. We view repeated high-fidelity simulation as important in the provision of future educational training packages for SCT. This training programme did not address the management of a failed SCT. This is an important issue to address in future work but was beyond the scope of our study. We did not compare the effect of surgical training versus no surgical training on trainee performance in this study. The benefit of the training programme was assessed at a maximum of six months. Of course, it may take 30 years of clinical practice to experience a CICO event, and we cannot comment on the longevity of benefit. The retention of cricothyroidotomy skills are known to be lost after six to nine months. 41 So, we suggest anaesthetists refresh their CICO skills annually (ideally every six months 42 ). The delivery of this training package may be limited by resources in the host institution. However, we have found it feasible to run. In our hospital, all consultants and trainees undertake the training package on an annual basis.
Conclusions and recommendations
Using the MRC definition, our collaborative programme represents a complex intervention in CICO training. 11 Accordingly, we undertook a pilot, mixed-methods study to assess its usefulness in a cohort of anaesthetic trainees. We have demonstrated improved performance, competence and self-confidence in surgical skills, leading to increased willingness to initiate SCT. The thematic analysis identified a reluctance to take on the role of a surgeon. We consider that this can be improved by repeated deliberate practice, including exposure to hands-on surgical training. Not all hospitals offer exposure to elective surgical tracheostomy on a weekly basis, but other operations, not necessarily performed on the neck, may offer similar opportunities to gain transferable skills and diminish the unfamiliarity of SCT. 11 This work suggests that our CICO training package is feasible and warrants further evaluation with national anaesthetic training programmes. Our results describe potential mechanisms through which improvements in managing a CICO may be achieved and explores the complex psychological processes that occur when an anaesthetist encounters a CICO scenario. SCT is indicated as a final method of airway salvage in many international airway algorithms,1–5 even if percutaneous methods have been employed as a first method in CICO. We therefore recommend incorporating an element of hands-on surgical teaching in CICO training programmes. In our opinion, this may represent the future of FONA training internationally, not just in the UK.
Supplemental Material
Supplemental material for A mixed-methods pilot study to evaluate a collaborative anaesthetic and surgical training package for emergency surgical cricothyroidotomy
Supplemental Material for A mixed-methods pilot study to evaluate a collaborative anaesthetic and surgical training package for emergency surgical cricothyroidotomy by Richard J Berwick, William Gauntlett, Sergio A Silverio, Hilary Wallace, Simon A Mercer, Jeremy M Brown, John E Sandars, Ben Morton and Peter Groom in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
Our thanks to Professor Simon Rogers, consultant maxillofacial surgeon, for help and support delivering this collaborative training package. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health. BM thanks the National Institute of Health Research Global Health Research Unit on Lung Health and TB in Africa at LSTM-‘IMPALA’ for helping to make this work possible. IMPALA funds research time for BM at the Liverpool School of Tropical Medicine but did not contribute directly to this project.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RB has received equipment from TruCorp Ltd. BM has accepted a travel bursary from Fisher & Paykel. PG has accepted a travel bursary and speaking fee from Fisher & Paykel. The remaining authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a small project grant from the Difficult Airway Society awarded via the National Institute for Academic Anaesthesia. It was also supported by a grant from the Mersey School of Anaesthesia Charity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.