
Abstract

Equipment deficiencies are recognised as a major contributor to airway morbidity and mortality, and previous audits conducted in Australia, 1 New Zealand 2 and the United Kingdom 3 have demonstrated poor availability or organisation of difficult airway equipment. The immediate availability and organisation of difficult airway equipment is essential for all critical care units. Equipment should be organised in a logical fashion, and standardised to enable shared learning and facilitate teamwork and processes between sites and operators.
Following ethics approval (Top End Health Services HREC 2018-3095, the Central Australian HREC CA-18-3196), we audited difficult airway trolleys (DATs) in the Northern Territory (NT) against standards set by the Australian and New Zealand College of Anaesthetists 4 and the Difficult Airway Society (DAS). 5 Seven out of the eight hospitals offering anaesthesia, emergency department (ED), or intensive care unit (ICU) services in the NT were surveyed regarding their DATs. The trolleys were scored according to the presence or absence of essential and non-essential equipment and storage conditions. The scores were converted into percentages and analysed using descriptive statistics.
Of the 15 trolleys examined, seven were in theatre suites, six in EDs and two in ICUs. Theatre trolleys were the best equipped, with median scores of 88.9% and 37.5% for essential and non-essential equipment, respectively. ICU trolleys had the best organisation, with a median score of 100% for storage conditions.
The median score for essential equipment was 77.8%, with a low score of 61.1% and a high score of 94.4%. Each trolley scored 100% for the items multiple endotracheal tubes, bougies and scalpels. No trolley had an oesophageal detection device. Non-essential equipment had a median score of 42.9%, with a low of 14.3% and a high of 57.1%. Every department had ready access to a videolaryngoscope. Combitubes® (ETC, Kendall-Sheridan Catheter Corp., Argyle, NY, USA), double-lumen endotracheal tubes and light wands were not available on any trolley. Figure 1 shows the availability of equipment.
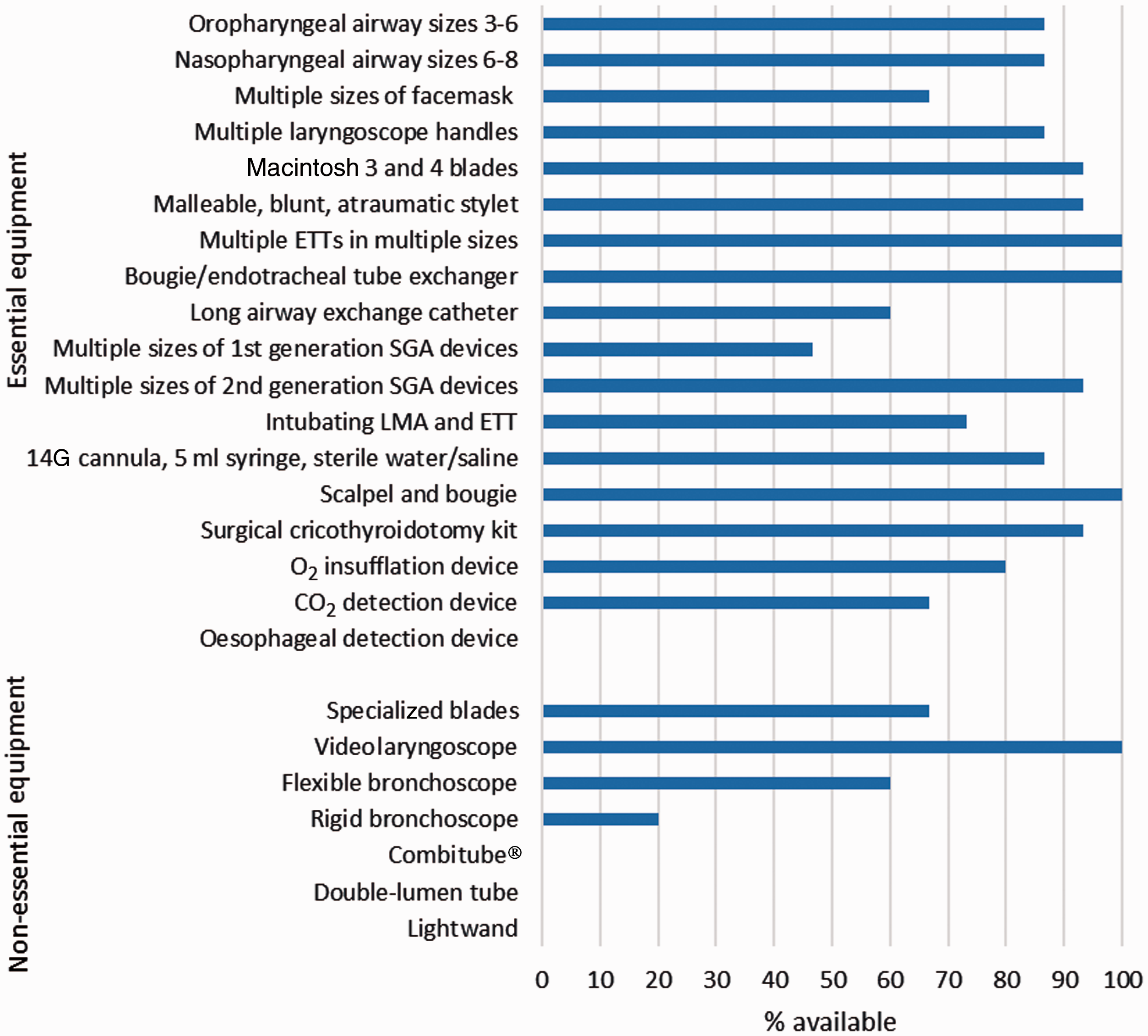
Availability of equipment on difficult airway trolleys.ETT: endotracheal tube; SGA: supraglottic airway; LMA laryngeal mask airway. Combitube® (ETC, Kendall-Sheridan Catheter Corp., Argyle, NY, USA).
The median score for storage conditions of difficult airway equipment was 87.5% with a low of 12.5% and a high of 100%. Of the 15 trolleys, seven scored 100% for storage. The criteria with the highest individual scores at 86.7% each included dedicated container, reviewed ± replenished in the last three months and equipment within expiry dates. Cognitive aids were on 53.3% of trolleys.
During this audit the chief investigator was frequently asked by site investigators if intubating laryngeal mask airways (iLMAs) should still be included on DATs. Investigators were concerned iLMAs have a low first-pass success rate and may distract clinicians from definitive front-of-neck access in an airway emergency, wasting valuable time. Given the 2015 update to the DAS guidelines advising against blind intubation down iLMAs, airway interest groups may want to consider the ongoing inclusion of iLMAs in DAT guidelines.
The audit identified good compliance when compared to other similar audits. 6 The strengths of the audit include its simplicity and objectivity leading to easy reproducibility, and the collection tool can be converted to a standardised checklist for ongoing quality assurance. A limitation of this audit is that it relied on recruited doctors at sites outside of Darwin, with an inherent potential for reporting bias. The tick-box nature of this audit may also have missed items included on the trolley but not on the list. The availability, organisation and standardisation of equipment and cognitive aids are central to clinician and team performance in an airway emergency. This audit highlights an opportunity to improve DATs across the NT. The findings have been presented to the Top End Health Service, and DAT guidelines have been updated and distributed to stakeholders in the NT for review and implementation.
Footnotes
Acknowledgements
The authors would like to thank investigators Dr Phillipa Tallis, Katherine Hospital; Dr Josh Mark, Gove District Hospital; Dr Zoran Stojkovski, Alice Springs Hospital; Dr Serne Kemp, Tennant Creek Hospital; Dr Peter Harbison, Darwin Private Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.