
Abstract
The first 4000 reports to the webAIRS anaesthesia incident reporting database were used to evaluate pulmonary aspiration in patients undergoing procedures under general anaesthesia or sedation. Demographic data, predisposing factors, outcome and potential preventative measures were evaluated. In these reports, 121 cases of aspiration were identified. Aspirated substances included gastric contents, bile type fluids, blood and solids; 60 (49.6%) patients were admitted to the intensive care unit/high dependency unit, and 43 (35.5%) required mechanical ventilation. Aspiration was associated with significant harm in >50% of reports, and eight (6.6%) patients died. Factors associated with a risk ratio of aspiration >1.5 and outside the 95% confidence interval for no event included: age >80 years, emergency procedure, procedure undertaken in freestanding day unit or gastroenterology department, procedure undertaken between 1800 and 2200 hours and endoscopy procedures. Only 11 (9%) cases appeared to be inadequately fasted, and 77 (64%) were definitely fasted. In the remaining 33 (27%), fasting was not mentioned. In 18 (14.9%) cases, aspiration occurred in the presence of cricoid pressure. Potential measures to prevent aspiration included using a cuffed endotracheal tube rather than a laryngeal mask airway in cases at high risk of aspiration and being made more aware of potential risk factors by improvements in team communication. Aspiration continues to be an important complication of anaesthesia, and one that can be difficult to predict and to prevent.
Introduction
Incident reporting has an established place in quality assurance programmes in many industries (e.g. aviation, nuclear power) and has been embraced by anaesthesiology as a useful method to evaluate clinical practice. The Anaesthesia Incident Monitoring Study (AIMS) was initiated in 1988 and subsequently evaluated >7000 reports, resulting in a series of reports, crisis management algorithms and review papers. 1 The webAIRS system was developed later as a new web-based, de-identified system, used for collecting and evaluating clinical incidents in anaesthesia from Australian and New Zealand hospitals and other healthcare facilities. 2
Aspiration of various substances (gastric contents, blood and other foreign bodies) continues to be an important complication of anaesthesia and was cited by the 4th National Audit Project (NAP4) of the Royal College of Anaesthetists as the major cause of airway-related deaths in the UK.3,4 Aspiration data from Australia and New Zealand were reported from AIMS data using a different methodology, but these data are now almost 20 years old. 5 The aim of the present study was to analyse the incidents coded as aspiration during anaesthesia in the first 4000 cases reported to webAIRS.
Methods
The methods used in this study, the categorisation of the first 4000 incidents and the relevant ethics approvals have been described in detail previously.2,6
The first 4000 reports from the database were accessed using Structured Query Language (SQL) to extract reports associated with aspiration. The SQL query used the term ‘respiratory/airway’ as the main category and the term ‘aspiration’ as the subcategory in the codified data. This was combined with a narrative search using an SQL query which included the term ‘aspiration’. The initial reports targeted for inclusion in this analysis were created by M.C., and then M.K. and M.C. validated the aspiration events into definite, possible and improbable events. Possible reports were re-evaluated and allocated to be included or excluded from the final analysis. Some reports in the aspiration group appeared to be exact duplicates and were excluded, whilst others with almost identical narratives that were entered around the same date were combined into a single report, as it was assumed that two separate people had entered the same case.
The database was then re-evaluated and coded for a second time by both M.C. and M.K. Some reports had been coded by the reporter as ‘no patient involved’. These were excluded from further analysis. The remaining incidents were classified into (1) aspiration and (2) no aspiration. Reports were coded as ‘aspiration’ if the reporter indicated that aspiration had occurred, and additionally when chest X-ray imaging indicated new changes consistent with pulmonary aspiration, even if the reporter had not explicitly indicated that aspiration had occurred. M.C. and M.K. undertook a detailed individual review of every report in the aspiration group but not in the no aspiration group. M.M. and A.M. undertook additional reviews of selected reports and commented on certain matters related to this process, but the final coding of these reports was by agreement between M.C. and M.K. All elective cases were assumed to have been fasted unless there was an explicit comment to the contrary from the reporter. Inadequate anaesthesia was only coded if specifically indicated by the reporter. The respiratory outcome was coded as aspiration pneumonia if this had been noted by the reporter or if new X-ray changes consistent with pneumonia were noted. Potential preventability was determined by the reviewing authors (M.K. and M.C.), taking into account the assessment of the reviewer. Reviewers also evaluated the narratives for potential risk factors which were not stated by the reporter for preventability, outcome and other noteworthy features.
As described previously, 6 we calculated the proportion of incidents in each of the two groups—aspiration and no aspiration—pertaining to selected characteristics potentially relevant to the risk of aspiration (e.g. age band, American Society of Anesthesiologists (ASA) category, location of procedure, etc.). We then calculated the risk ratio (RR) for each of these characteristics as the proportion with that characteristic among the aspiration incidents divided by the proportion among the no aspiration incidents, with 95% confidence intervals (CIs) calculated using Wald continuity correction. In methodology consistent with previous publications evaluating webAIRS data, if the 95% CIs did not overlap and the RR was >1.5 or <0.67, we deemed the factor as potentially associated with more or fewer aspirations reports, respectively. 6 All analyses were performed using R 3.5.0 7 in RStudio 1.1.447. 8 The data.table 1.11.8 9 package was used for calculations, and packages used for generating tables and figures were ggplot2 3.0.0, 10 huxtable 4.0.0.9000, 11 flextable 0.4.4, 12 tableone 0.9.3 13 and officer 0.3.0. 14
Results
From the 4000 reports in the webAIRS database, 71 reports were omitted, as there was no patient involved or the incidents affected multiple patients or involved potential hazards to patients. Of the remaining 3929 reports, we identified evidence of pulmonary aspiration in 121 patients. Aspirated substances included gastric contents, bile type fluids, blood and solids (Figure 1). In patients reported as having aspirated, chest X-ray changes were noted in 54 (44.6%) reports. The majority of patients who aspirated were managed in the postoperative care unit or general ward, but 60 (49.6%) patients were admitted to the intensive care unit (ICU)/high dependency unit (HDU), with 43 (35.5%) patients requiring a period of postoperative ventilation. Aspiration events were associated with significant harm in >50% of the reports (Tables 1 and 2).
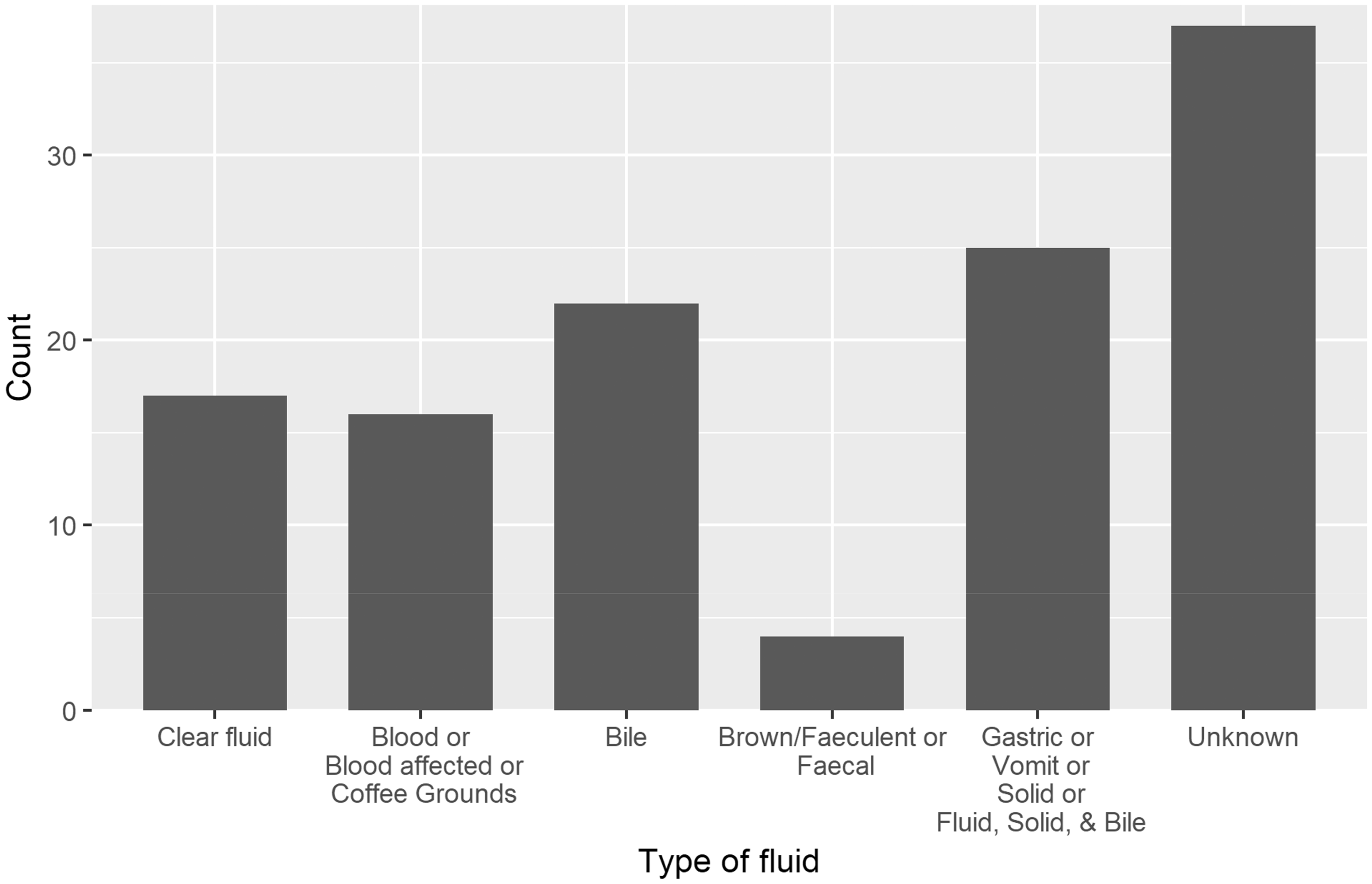
Type of material aspirated, as described in the narrative.
Immediate and final outcome from aspiration event.
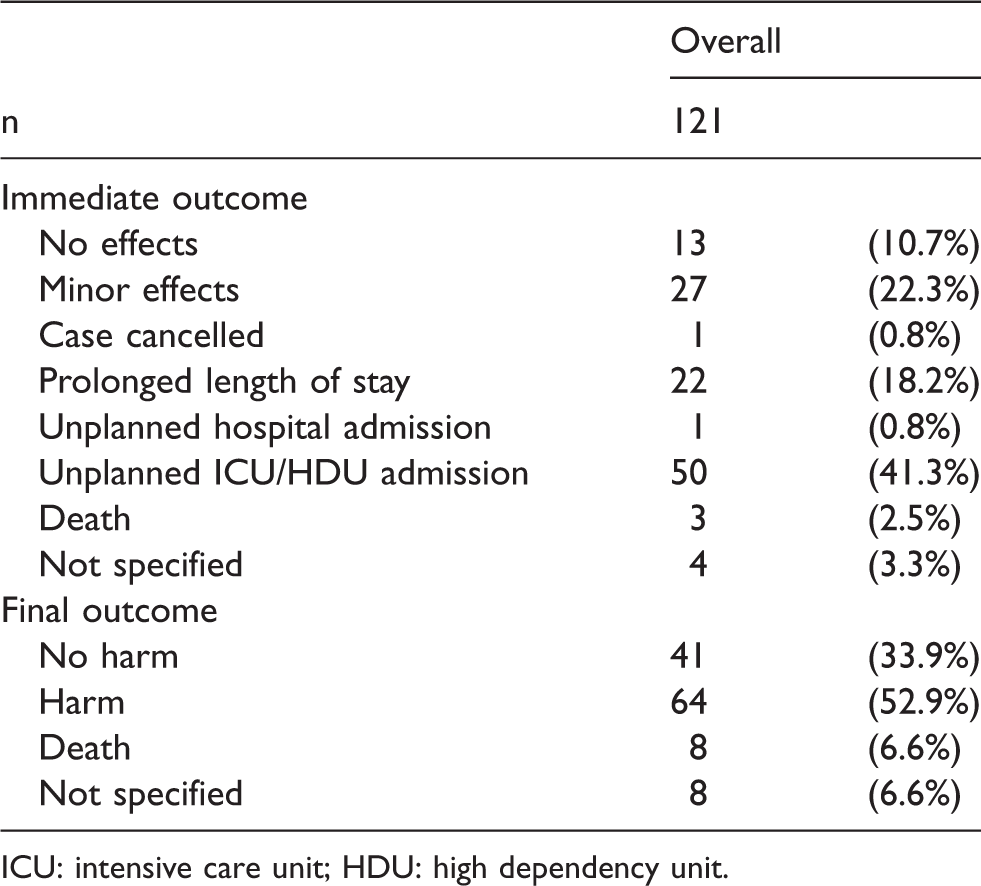
ICU: intensive care unit; HDU: high dependency unit.
Patient outcome: Proportion associated with aspiration and no aspiration, and risk ratio for aspiration versus no aspiration.
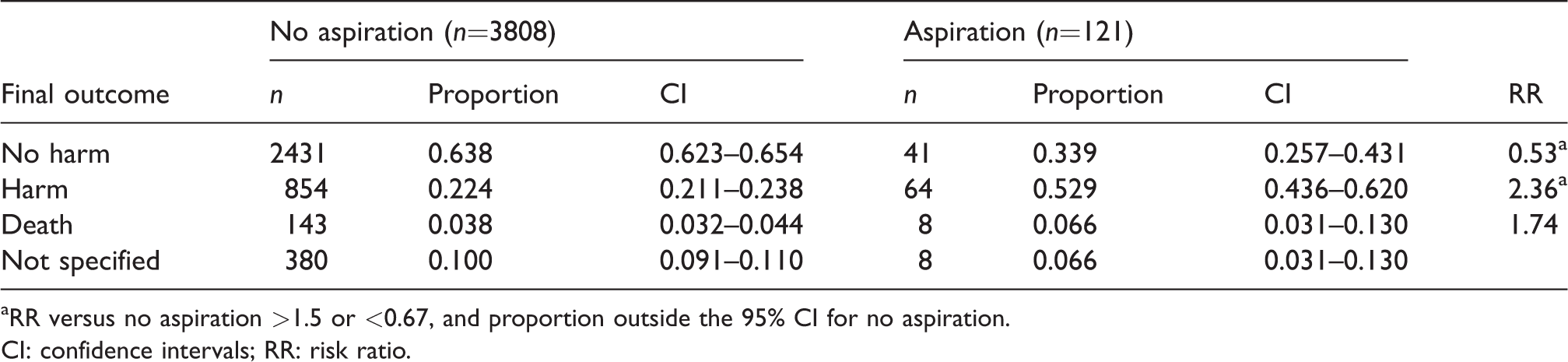
aRR versus no aspiration >1.5 or <0.67, and proportion outside the 95% CI for no aspiration.
CI: confidence intervals; RR: risk ratio.
Sex of patients involved in the reports: Proportion associated with aspiration and no aspiration, and risk ratio for aspiration versus no aspiration.

CI: 95% confidence intervals; RR: risk ratio; F: female; M: male.
The numbers of reports and RRs for aspiration versus no aspiration categorised by sex, age, body mass index (BMI), ASA, grade of anaesthetist, location of incident, time of day, urgency of surgery and surgical specialty are shown in Tables 3–11. Factors associated with an RR of aspiration >1.5 and outside the 95% CI for no event included: age >80 years, emergency procedure, procedure undertaken in freestanding day unit or gastroenterology department, procedure undertaken between 1800 and 2200 hours, and endoscopy procedures. Obstetric and gynaecology procedures were associated with an RR of <0.67 and outside the 95% CI for no event.
Age of patients involved in the reports: Proportion associated with aspiration and no aspiration, and risk ratio for aspiration versus no aspiration.
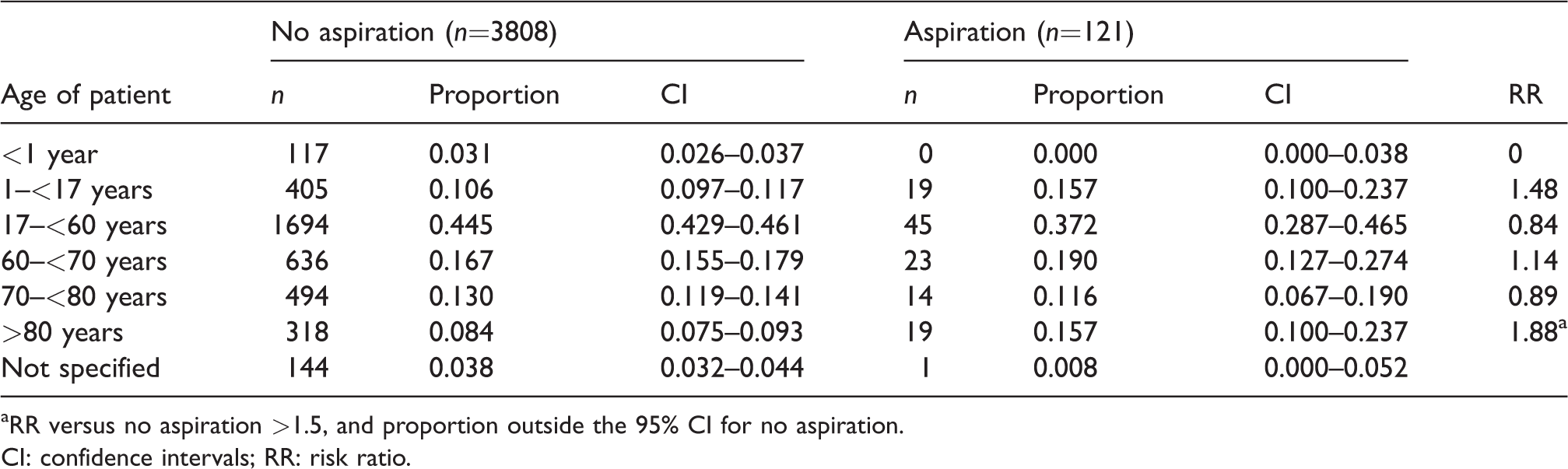
aRR versus no aspiration >1.5, and proportion outside the 95% CI for no aspiration.CI: confidence intervals; RR: risk ratio.
Body mass index of patients involved in the reports: Proportion associated with aspiration and no aspiration, and risk ratio for aspiration versus no aspiration.
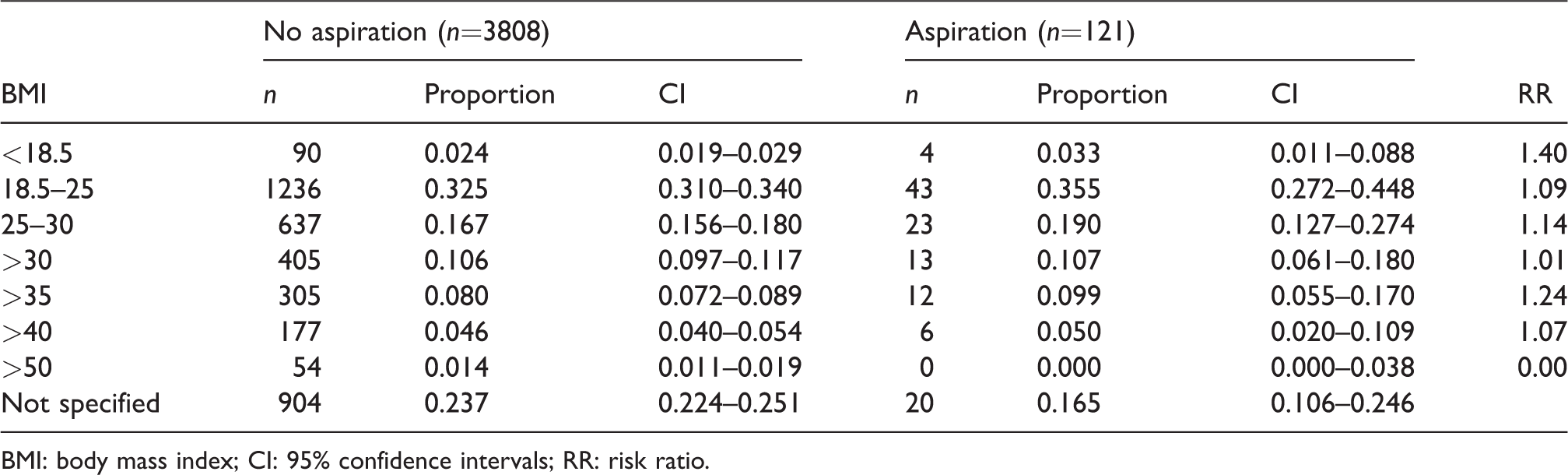
BMI: body mass index; CI: 95% confidence intervals; RR: risk ratio.
American Society of Anesthesiologists physical status of the patients involved in the reports: Proportion associated with aspiration and no aspiration, and risk ratio for aspiration versus no aspiration.
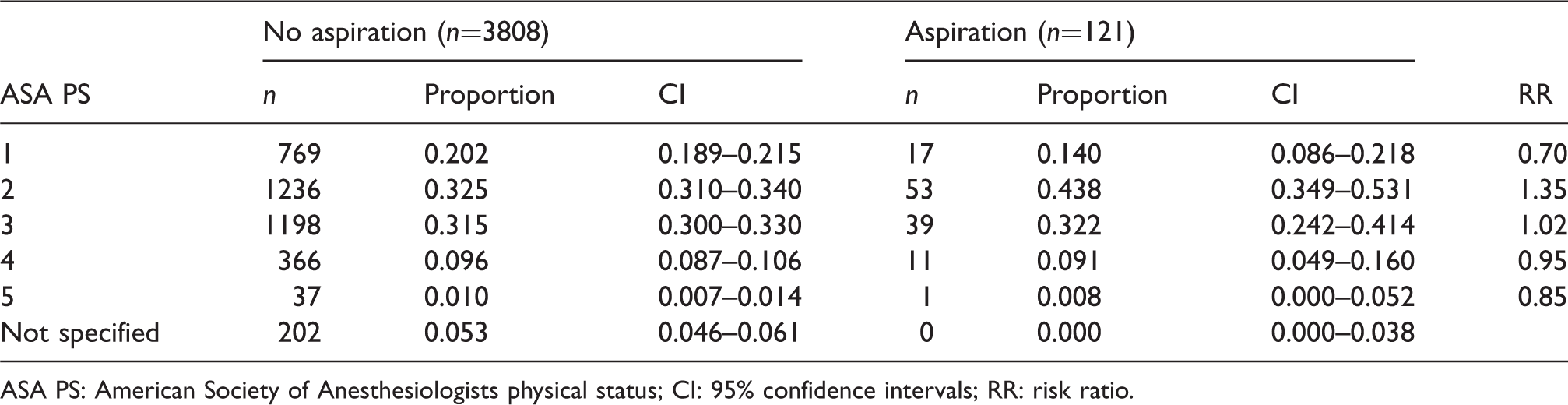
ASA PS: American Society of Anesthesiologists physical status; CI: 95% confidence intervals; RR: risk ratio.
Urgency of case reported: Proportion associated with aspiration and no aspiration, and risk ratio for aspiration versus no aspiration.
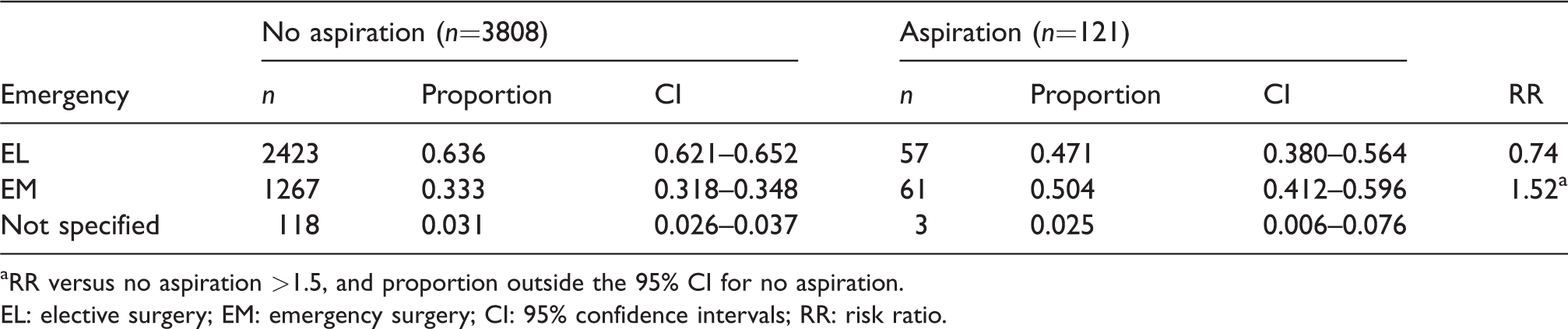
aRR versus no aspiration >1.5, and proportion outside the 95% CI for no aspiration.
EL: elective surgery; EM: emergency surgery; CI: 95% confidence intervals; RR: risk ratio.
Grade of anaesthetist involved in the reports: Proportion associated with aspiration and no aspiration, and risk ratio for aspiration versus no aspiration.
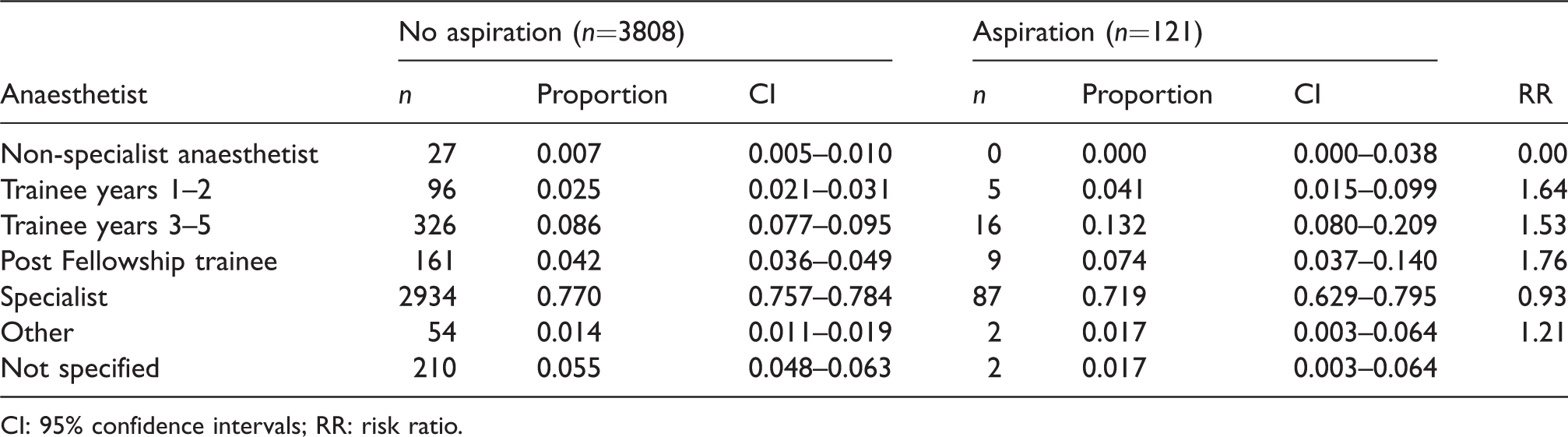
CI: 95% confidence intervals; RR: risk ratio.
Location of incident: Proportion associated with aspiration and no aspiration, and risk ratio for aspiration versus no aspiration.
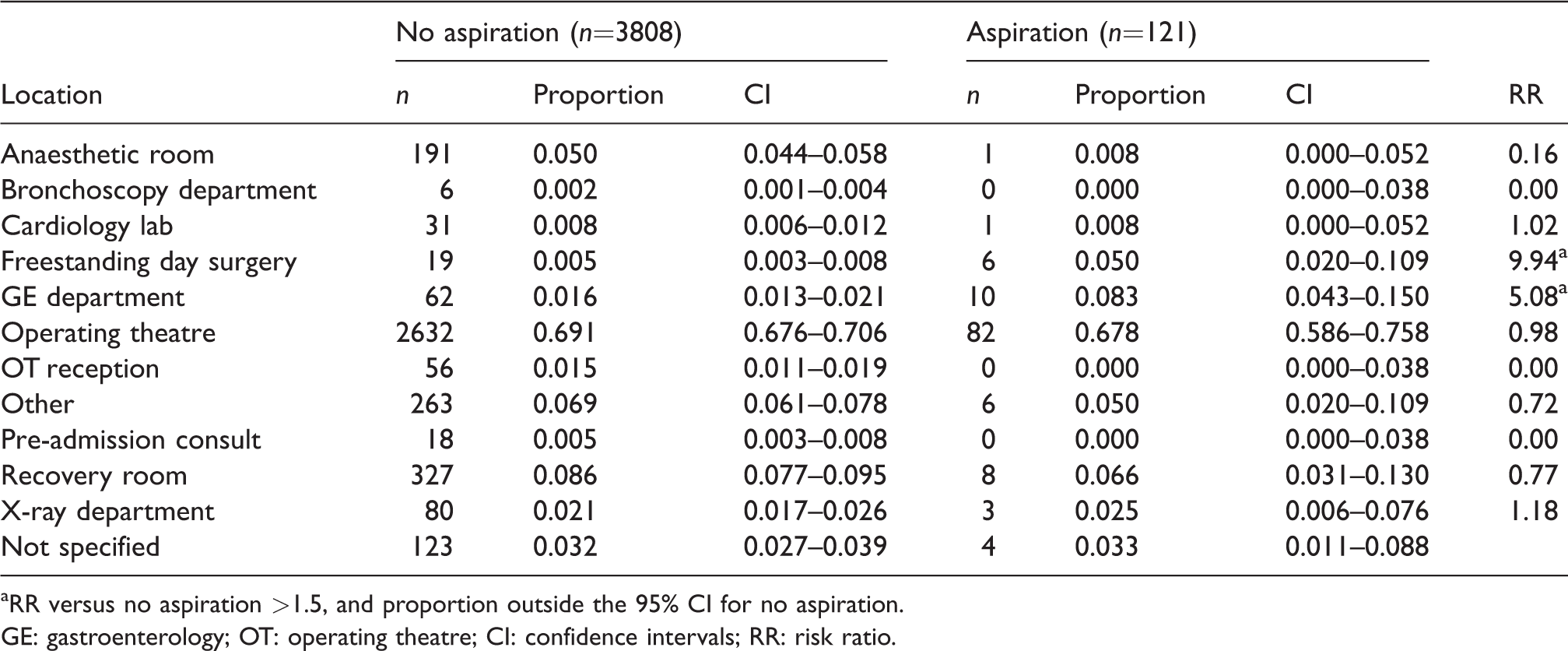
aRR versus no aspiration >1.5, and proportion outside the 95% CI for no aspiration.
GE: gastroenterology; OT: operating theatre; CI: confidence intervals; RR: risk ratio.
Time of procedure: Proportion associated with aspiration and no aspiration, and risk ratio for aspiration versus no aspiration.
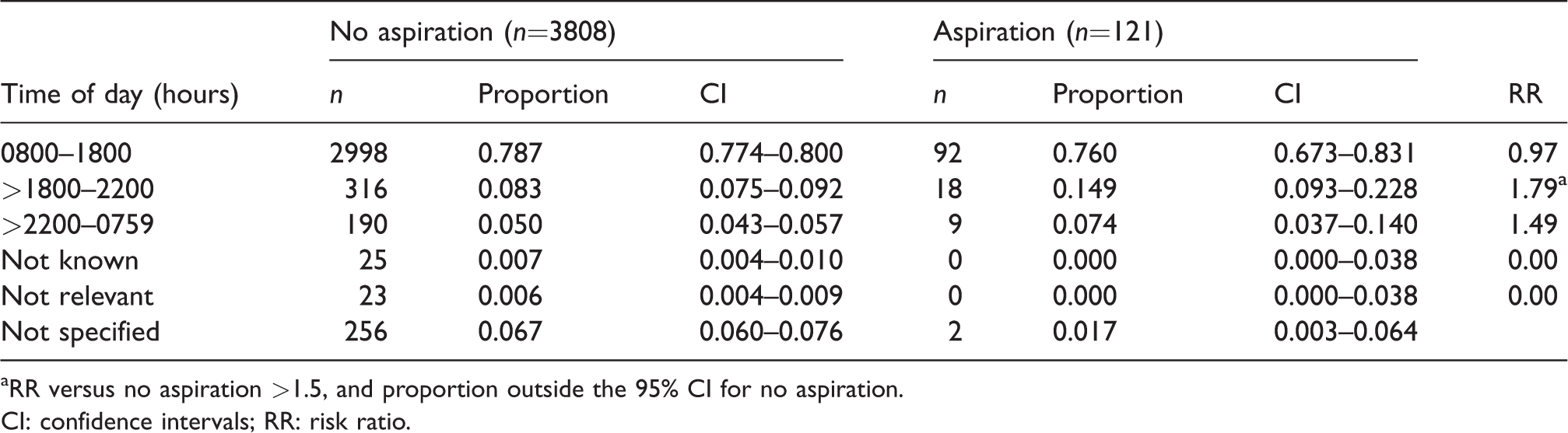
aRR versus no aspiration >1.5, and proportion outside the 95% CI for no aspiration.CI: confidence intervals; RR: risk ratio.
Surgical specialty of case reported: Proportion associated with aspiration and no aspiration, and risk ratio for aspiration versus no aspiration.
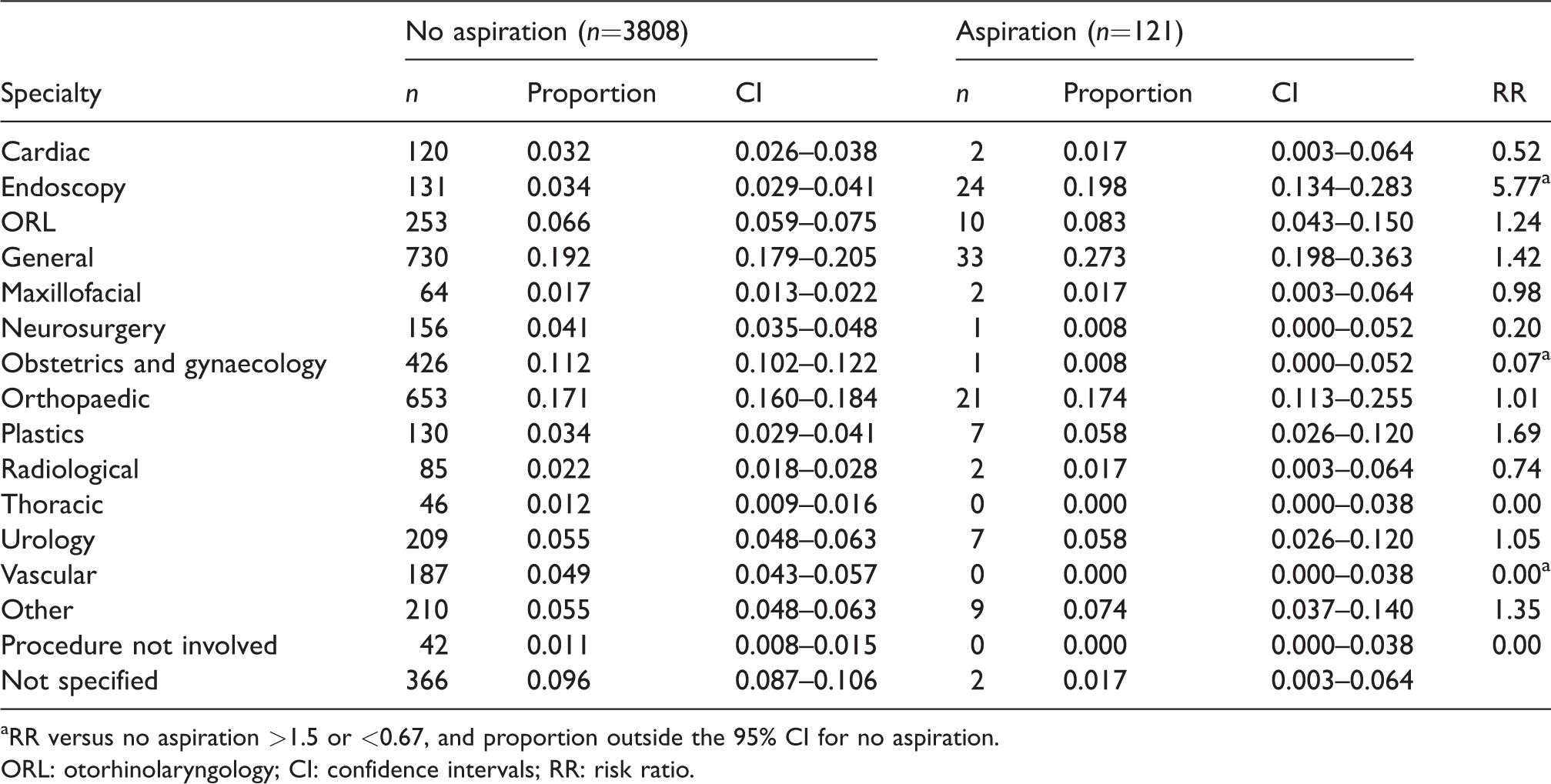
aRR versus no aspiration >1.5 or <0.67, and proportion outside the 95% CI for no aspiration.
ORL: otorhinolaryngology; CI: confidence intervals; RR: risk ratio.
Factors recorded by reporter as contributing to the aspiration event.
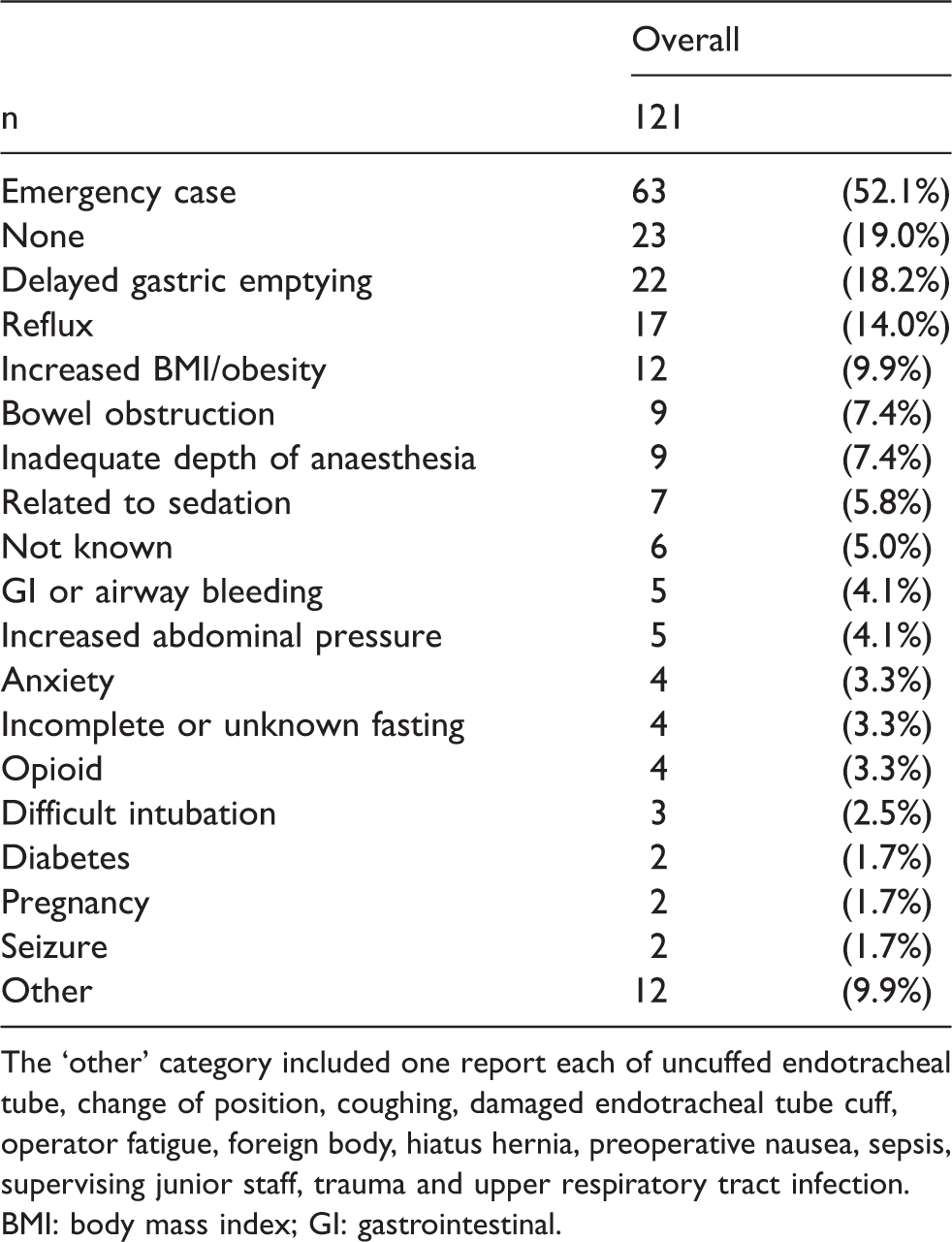
The ‘other’ category included one report each of uncuffed endotracheal tube, change of position, coughing, damaged endotracheal tube cuff, operator fatigue, foreign body, hiatus hernia, preoperative nausea, sepsis, supervising junior staff, trauma and upper respiratory tract infection.BMI: body mass index; GI: gastrointestinal.
The most common contributory factors recorded by the incident reporters were emergency surgery, delayed gastric emptying, increased BMI, inadequate depth of anaesthesia and bowel obstruction (Table 12). In addition, reviewers identified a documented history of reflux in one in seven reports and a clinical risk of regurgitation and aspiration in almost two in three reports. Only 11 (9%) cases appeared to be inadequately fasted, and 77 (64%) were definitely fasted. In the remaining 33 (27%) cases, fasting was not mentioned. Four reports suggested a possible breach in elective fasting guidelines, but this breach was confirmed postoperatively in only one report. In 14 cases, it appeared there was inadequate communication regarding surgical plan, patient comorbidity or fasting status.
Preventability of aspiration event: Proportion associated with aspiration and no aspiration, and risk ratio for aspiration versus no aspiration.

CI: 95% confidence intervals; RR: risk ratio; Y: yes; N: no.
Reporting anaesthetists indicated that the incident was potentially preventable in 55 (45.4%) cases (Table 13), whereas the reviewers considered that only 21 (17.4%) were likely to be preventable, with an additional 18 (14.9%) considered possibly preventable. The strategy most commonly identified to reduce risk involved a clinical decision to intubate the trachea rather than use a supraglottic airway, or to undertake a rapid sequence induction (RSI). However, aspiration occurred in 18 (15%) cases where an RSI with cricoid pressure had been undertaken.
No reviewer or respondent cited improvements in pharmacological prophylaxis or better adherence to fasting guidelines as potentially important factors to reduce aspiration risk or sequelae. Reviewers questioned the clinical decision to use a laryngeal mask airway (LMA) in one patient with bowel obstruction.
Risk factors associated with lower gastrointestinal (GI) endoscopy in the webAIRS data included moving the patient and subjecting the abdomen to external pressure to facilitate endoscope passage. Many of these cases were sedated with combinations of propofol, midazolam and fentanyl, and although difficult to quantify from the narratives, the majority of the cases appeared to have deep sedation and, as such, possibly had more impaired protective reflexes than if carried out at lighter levels of sedation.
Discussion
The present study clearly reinforces the message that the pulmonary aspiration of gastric contents, blood or solid material continues to be an important cause of anaesthesia-related morbidity and mortality, with associated increased costs of health-care utilisation. More than 50% of patients who aspirated had chest X-ray changes or clinical evidence of significant aspiration, which is similar to the rate reported by Olsson 15 (47%) in a study of >185,000 procedures. Approximately half of those who aspirated required HDU admission, and many needed mechanical ventilation. Interestingly, harm was associated with a higher proportion of aspiration reports than the combined reports of all other types of incident reported to the webAIRS database (see Table 2). Death followed the aspiration event in eight cases, despite admission to the ICU and periods of ventilation in most of these cases. Many of the patients who died were elderly and suffering from various, often serious, comorbidities. Whilst aspiration may not have been the main mechanism for death, it was clear that the aspiration event contributed importantly to these deaths. These observations are consistent with the finding of the NAP4 study which identified aspiration as one of the most important causes of anaesthesia-related death,3,4 and with those of the ASA Closed Claims Study in which claims for patients who have aspirated had twice the risk of death than those whose claims were associated with other complications. 16
Our data suggest that risk may be greater in emergency procedures and procedures undertaken between 1800 and 2200 hours. The RR was also increased (to 1.49) for cases undertaken between 2200 and 0759 hours, but with 95% CIs that overlapped those for cases in which aspiration did not occur. However, the number of cases in this category was small, and it seems reasonable to infer that all cases undertaken out of hours may be at increased risk of aspiration. This is consistent with an older Swedish study 15 which suggested a sixfold incidence of aspiration in out-of-hours cases. Obviously, a higher proportion of procedures undertaken during these hours are likely to be emergencies than those undertaken during working hours. Other factors, such as the grade of the anaesthetist, might also play a part in the greater risk out of hours. Yet, in our data, the grade of the anaesthetist did not meet our criteria for association with an increased risk. Moreover, changes in clinical work practice have led to a reduction in out-of-hours surgery and with unsupervised (or distantly supervised) junior trainees managing at-risk cases.
The increased RR for patients >80 years of age is also consistent with the ASA Closed Claims Study, in which older patients were over-represented in claims associated with aspiration. 16
The RR was increased in endoscopy procedures and in procedures undertaken in freestanding day units or gastroenterology departments, which may reflect the same group of patients. Many patients undergoing these procedures are highly comorbid and potentially have unstable physiology. There is debate in the gastroenterology literature regarding same-day bowel preparation 17 and high residual gastric volumes, 18 and some studies suggest up to 10% of patients may present with ‘at risk’ gastric volumes prior to endoscopy. 18 A recent systematic review indicated upper GI endoscopy was associated with higher morbidity and mortality rates than other procedural sedation techniques. 19 Seven of the eight deaths were reported in patients with significant comorbid disease (e.g. neurological problems, active upper GI bleeding) undergoing upper GI endoscopy. Further research into the reasons for this potentially important observation is warranted. The reduced RR in patients undergoing obstetric and gynaecology procedures is of interest because these procedures (particularly obstetric procedures) have long been held to have an increased risk of aspiration. However, our data do not provide any insight into the reason for this observation. Despite frequent associations between aspiration and increased BMI, this association was not identified by RR analysis in the present study, although the reporting anaesthetists identified an increased BMI as a risk factor in 9.9% of cases.
The literature cites a wide range of rates for aspiration (from 1 in 900 to 1 in 10,000 anaesthetic cases), depending on acuity.20,21 Aspiration may be less common in paediatric patients and may also be associated with less morbidity and mortality in these patients than in the adult population.22,23 Conversely, the rate may be higher in other clinical areas such as emergency medicine, where rates of nearly 1 in 12 cases following emergency intubation have been described. 24 Risk factors commonly cited in the literature include emergency cases, increased BMI, inadequate anaesthesia and a history of reflux. 25 However, the sensitivity and specificity for these factors is low, and there is no recognised/agreed ‘Aspiration Risk Index’. Furthermore, as confirmed by our data, aspiration often occurs in young patients with no identifiable risk factors at all. Gastric ultrasound has been shown to have value in assessing the risk of aspiration in both adult and paediatric patients,26,27 but its widespread use is limited by the need for training and equipment.
The degree of preventability of an event is difficult to assess from incident reporting data. The earlier AIMS study suggested that up to 60% of cases with an aspiration event could have been prevented. 5 However this was based on ideal conditions with physical and pharmacological interventions (e.g. cricoid pressure, fasting, antacids, etc.) that were assumed to be 100% effective. Evaluation of the current data was more pragmatic and recognised only clear and practicable preventable factors. The principal strategy recommended in the literature for the prevention of aspiration is to secure the airway and isolate it from the GI tract. Current practice implies the placement of a cuffed endotracheal tube (ETT), often with an RSI with cricoid pressure. Some recommendations have included the use of endotracheal intubation in all emergency cases, but these are not universally followed, and there is some variation in definitions of what designates an emergency case.
Several cases in the present report had a planned RSI, but difficulty was experienced with tube placement, cricoid pressure was unreliable, or aspiration occurred even with an ETT in place. Similar observations were made in the ASA Closed Claims Study 16 and in the NAP4 study.3,4 In some reports to the webAIRS database, dual-lumen (DL)-LMAs had been chosen in preference to an ETT. The role of DL-LMAs has not been evaluated in high-risk cases, although there is some evidence to suggest that DL-LMAs may fail to protect against aspiration during cardiopulmonary resuscitation. 28
Fasting policies appear to be widely followed, and from our reports, we identified only one confirmed instance of a breach in accepted fasting duration. Antacids, histamine type 2 receptor antagonists and proton pump inhibitors are all recommended to reduce the risk of aspiration.29,30 It is generally suggested that chemoprophylaxis is not warranted for routine low-risk procedures, but should be considered for patients at an increased risk of an aspiration event. However, robust studies assessing the impact of these agents on clinical outcomes (e.g. morbidity/mortality) are lacking, and the majority use surrogate endpoints instead (e.g. pH and volume). Furthermore, these agents only serve to reduce the acidity of gastric contents, and in our reports, a high proportion of patients aspirated bile-stained fluids, blood and particulate matter, which would not be altered by such agents.31,32 Significantly, no reporter or assessor identified the use of pharmacological agents to be a potential factor in preventing or reducing the outcome in the cases reported here. In a recent ultrasound-guided study of 110 patients, whilst one in two non-emergency cases had a preoperative empty stomach, one in 14 had a residual gastric volume of >100 mL, possibly predisposing to an aspiration event. 31
Importantly, several reports commented upon the lack/inadequacy of communication between members of the surgical/anaesthesia team in relation to clarifying aspects of the surgical plan (e.g. potential for airway contamination with irrigating fluids), patient comorbidities (e.g. recent upper GI bleed, ongoing nausea) or fasting status (e.g. intake of fluids <60 minutes before induction of general anaesthesia). The World Health Organization (WHO) Surgical Safety Checklist 33 has now been adopted widely, and team briefings are encouraged before any operative intervention. It may be that issues relating to airway security and/or aspiration risk are specifically addressed at the sign-in to focus attention to this ongoing clinical issue and potentially highlight any corrective strategy.
The benefits and limitations of incident reporting in general, and of the webAIRS system in particular, have been outlined in a previous report. 2 Any statistical inferences are limited by the absence of denominator data and the incompleteness of numerator data, making meaningful comparisons with registry databases (e.g. Olsson 15 ) difficult. The comparisons we have made are therefore purely descriptive. The comparison made between the aspiration and no aspiration groups and outcomes suffers a further limitation: the no aspiration group was taken from the larger webAIRS database rather than from a random sample of all patients undergoing anaesthesia. Thus, there may well be biases associated with the selection of this control group.
In conclusion, aspiration continues to be an important complication of anaesthesia and one that can be difficult to predict and to prevent. More work is needed to improve quantification of the risk of aspiration, potentially through the wider use of ultrasound to evaluate gastric contents. Securing the airway with an ETT in patients at high risk of aspiration still seems to be the principal method for the prevention of aspiration, but may prove difficult and thus may fail in this objective. Therefore, we suggest reinforcing the message that both the risk of aspiration and the potential for difficulty with the airway should be formally evaluated for every case undergoing anaesthesia or sedation as part of the WHO sign-in, and an appropriate plan made, particularly in emergency cases and those undertaken out of hours. A low threshold for requesting the assistance of a second anaesthetist would seem to be appropriate.
Footnotes
Acknowledgements
The continued support of the reporting anaesthetists is recognised, as is the support from webAIRS supporting organisations: The Australian and New Zealand College of Anaesthetists, The Australian Society of Anaesthetists and The New Zealand Society of Anaesthetists. Preliminary data were presented at the ANZCA ASM, Sydney, 2018.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.D.C. was previously Medical Director of the Australian and New Zealand Tripartite Anaesthesia Data Committee. No conflicting interests exist for the remaining authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The webAIRs database is jointly funded by the Australian and New Zealand College of Anaesthetists, the Australian Society of Anaesthetists and the New Zealand Society of Anaesthetists. The present study received no additional funding.