
Abstract
These abstracts are published as supplied and have not been subject to editorial review or correction.
8
Pressures in 3-way infusion devices: A bench-top study
Nepean Hospital
Introduction
The use of multiple infusions through one cannula is an increasingly common practice in anaesthesia. High pressures in the line often lead to occlusion alarms and pump disconnection. In this study, we aim to determine the pressures generated in common multi-infusion devices, using simple low-cost equipment available and currently in use in the operating theatre environment.
Aims
In this study, we aim to determine the pressures generated in common multi-infusion devices, using simple low-cost equipment available and currently in use in the operating theatre environment.
Methods
We compared three different common and commercially available multi-infusion sets that allowed multiple infusions through one cannula in vitro. One with anti-siphon valves, one without valves, and dual extension sets with side ports connected in series. An invasive blood pressure transducer was used to monitor line pressure. Seven different infusion rates were used to simulate different infusions.
Results
3-way sets with anti-siphon valves have 5.5 times the infusion pressures compared to devices without valves (P < 0.001). The highest pressures obtained across all sets were at the highest flow rate studied (400 ml/hr); this was 243 mmHg in the 3-way set with anti-siphon valves, compared to only 44 mmHg in the 3-way set without valves and 36 mmHg in the dual extension sets. Dual extension sets have the lowest pressures across all flow rates when compared to 3-way sets without valves. (P < 0.001).

Conclusions
Anti-siphon valves generate significantly higher pressures in infusion lines, especially at bolus flow rates, but such pressures are not high enough to trip pump occlusion alarms. There are multi-infusion devices without anti-siphon valves that have lower resistance, but clinicians should be aware of the possibility of siphoning when using them.
11
Audit of Practice in Australian and New Zealand Hyperbaric Units on the Incidence of Central Nervous System Oxygen Toxicity (CNS OT)
1Royal Brisbane And Womens Hospital
2University Of Queensland Faculty of Medicine
3QIMR Berghofer
4Redcliffe Hospital
Introduction
Central nervous system oxygen toxicity (CNS-OT) is an uncommon complication of hyperbaric oxygen treatment (HBOT). CNS-OT usually presents with prodromal symptoms such as sweating, twitching and tunnel vision, followed by a tonic-clonic seizure. It is most commonly brief and resolves spontaneously once the partial pressure of oxygen is reduced. However, patients are at risk of serious harm during a CNS-OT convulsion.
Air breaks are short periods of breathing air instead of oxygen that have been traditionally recommended to reduce the incidence of pulmonary oxygen toxicity Different facilities have developed local protocols to attempt to reduce the risk. The main difference between protocols is in the provision of number and length of air breaks.
Aims
Comparison of the Table 14 (TT14) compression protocols (243kPa) at all Australasian facilities to compare the incidence of CNS-OT events to identify if there is a protocol with a statistically significant better safety profile.
Methods
Retrospective cohort study of all consecutive patients who received treatments at eight hospitals in Australia and New Zealand over five years (January 2010 to January 2015), examining the incidence of CNS-OT events.
Results

Conclusions
HBOT is safe and CNS-OT is relatively rare. The risk of CNS-OT per patient at 243 kPa was 1 in 222 (0.4%; range of 0%−1%) and the overall risk irrespective of treatment table was 0.6% (range 0.31−1.8%). The wide disparity of facility protocols for a 234 kPa table without influence on the incidence of CNS-OT rates should facilitate an approach to consensus.
14
An audit on time to theatre for Neck of Femur (NOF) patients in a tertiary, trauma centre in Western Australia: comparison to accepted national standards
Royal Perth Hospital
Introduction
Patients with neck of femur fractures (NOF) are a known high risk group, with increased peri-operative morbidity and mortality.
The differences in outcomes of surgery at 36 hours versus 48 hours have not been studied in depth and this new timeline has as yet, not been clinically validated.
The general consensus in the literature, is that any undue delay to surgery results in poorer patient outcomes, with hospital costs increasing with increased length of stay.
Aims
The primary outcome was to determine the time taken from admission into ED to arrival in the operating theatre, to determine what percentage of patients had their operative fixation within 36 hours from admission into our institution.
The secondary aim was to identify the reasons for delayed operative fixation, and whether these were due to system failures which could be addressed.
Methods
This was a retrospective audit. The NOF registry database was accessed (a statewide database) and the data reviewed for all NOF patients admitted over a six month time period, from January to June of 2017.
Results
From our data we have identified that approximately 28% of patients were not operated within 36 hours and the most common reason was unavailability of theatre (36.5%), which is not an acceptable reason. The second commonest cause was medically unfit patients, which is an acceptable reason for delaying time to theatre.
Conclusions
We conclude that protocols and specialist input for patients on anticoagulation therapy and access to a dedicated emergency theatre dedicated for NOF will reduce inappropriate delay to hip fracture surgery experienced at our institution.


16
Impact of Visuospatial and Psychomotor Ability on Fibreoptic Bronchoscopy Performance
1South Western Sydney Clinical School, Faculty of Medicine, University of New South Wales, Sydney, Australia
2Department of Anaesthesia, Liverpool Hospital, Sydney, Australia
3Ingham Institute of Applied Medical Research, Sydney, Australia
4Nuffield Department of Anaesthesia, Oxford University Hospital NHS Trust, UK
Introduction
Flexible video fibreoptic bronchoscopy (FOB) is an important skill for anaesthetists. Other procedural skills such as regional anaesthesia have shown a significant positive influence of innate visuospatial and psychomotor abilities on how novices learn. Determining if these cognitive abilities also influence FOB performance allows supervisors to identify trainees most in need of training.
Aims
The primary aim was determining if visuospatial and/or psychomotor ability influences FOB performance, defined by the time taken to complete a bronchoscopy task. The secondary aim was whether the quality of FOB performance is similarly influenced, defined by a composite of global rating scale (GRS) and navigation accuracy scores.
Methods
Visuospatial testing used the Mental Rotations Test-A (MRTA), the Perceptual Reasoning Index (PRI), and the Judgment of Line Orientation test. Psychomotor testing used the Trail Making Part A and B tests, and the Symbol Search test.
Participants were medical students and junior medical officers with no prior exposure to FOB. All participants undertook the five psychometric tests prior to performing FOB on a Dexter manikin. This simulator has modular airways that was re-configured to increase difficulty and prevent learning effects with successive attempts.
Three FOB attempts were permitted: initial, a second attempt after 30 minutes discovery training, then after 1 month. Time taken to perform each attempt was labelled T1, T2, and T3.
Two blinded assessors independently viewed videos taken during each attempt and scored using a GRS. Assessors calibrated their scoring in an iterative pilot phase prior to actual scoring. Each FOB attempt on the Dexter was standardised and marked for completing navigation tasks to locate picture targets within bronchi. The GRS and navigation accuracy scores were normalised as a percentage of maximum possible score, defined as Q1, Q2, and Q3.
Results
There were 180 videos and psychometric test results on 60 participants. There was high assessor inter-rater correlation coefficient using the GRS (0.87 - pilot phase, 0.83 - study phase). Only the MRTA and PRI were significant for time taken and quality endpoints on univariate correlation. Multivariate analysis showed MRTA and PRI were significant, but gross and fine motor experience did not add to modelling. Participants demonstrated a significant improvement in FOB quality from Q1 to Q2, but not at Q3 re-testing.
Conclusions
Only the MRTA and PRI visuospatial tests were significant in predicting the time and quality of FOB performance by novices. FOB quality initially improves, but skills stagnate by 1 month without further training.
17
Experiences with a Mentor Program Model
1North-Western Training Scheme
2Department of Anaesthesia, Perioperative and Pain Medicine, Northern Health, Epping, Australia
3Department of Anaesthesia and Pain Management, Western Health, Footscray, Australia
Introduction
The benefits of mentoring to mentors, mentees, and organisations are well-demonstrated. [1]
In recent years, international anaesthesia training bodies have become aware of the relative lack of mentorship of trainees in comparison to other specialties. [2] Many health services and departments include some form of mentoring program. To date, there is a paucity of evidence in the scientific literature regarding mentoring in Australian anaesthesia trainees.
Aims
We evaluated a mentoring program for first-year anaesthesia registrars within the North-Western Training Scheme, Victoria in comparison to prior mentoring experiences.
Methods
We introduced a mentoring program, “Primary Examination Mentoring Scheme” (PEMS), to first-year anaesthesia trainees from six different health networks—including both metropolitan and regional centres. The program focused on providing support for exam preparation. Mentors were second year anaesthetic trainees nominated by Supervisors of Training. They were provided education and training by the Program Coordinator. Mentees gathered in self-nominated study groups (approximately four per group) and were given the option the opportunity to participate in the program. The Program Coordinator matched two mentors to every mentee group using a pre-program questionnaire. Mentees were also asked to fill in a pre-program evaluation survey. Both mentors and mentees were provided orientation sessions to elucidate their roles. Following introduction by the coordinator and a first meeting between mentees and mentors, subsequent meetings occurred at the discretion of mentors and mentees. Mentors were given regular support by the Program Coordinator. After undertaking the primary exam, mentees were invited to participate in a post-program evaluation survey. Quantitative data was obtained using Likert scales and qualitative data from solicited comments in the survey.
Results
There were 22 participants across two years (2016-2017), from which 17 responded initially in the pre-implementation phase, with 15 post-program evaluation surveys. Of those that initially responded, seven had previously participated in another mentoring program. Survey results showed that for those who had previously participated in mentoring programs had an improved experience—despite meeting mentors less regularly—after the PEMS program. (Figure 1) Regular occurring themes were related to organised leadership by the Program Coordinator, having goals but maintaining flexibility, and the dual (oftentimes conflicting) focus on preparing for exams and focusing on commencement of training.
Conclusions
Mentoring first-year anaesthesia trainees from diverse geographies and hospital cultures carries its unique challenges. We suggest further follow-up to ensure ongoing improvement and ensure sustainability, as long-term data for successful mentor programs is scarce.

Survey responses comparing mean Likert scores (0 = strong disagree, 5 = strong agree) from post-PEMS evaluation with previous mentoring experience(s).
References
18
Clinical Audit: Preoperative Ordering of HbA1C in Upper Gastrointestinal and Endocrine Surgical Patients
1Anaesthesia Resident, Austin Health, Victoria;
2Anaesthetist, Austin Health, Victoria;
Introduction
Diabetes is one of the most important contributors to the overall burden of disease in Australia1. Diabetes and higher HbA1C are independently associated with a higher risk of adverse outcomes after surgery2,3. A clinical audit guideline published by ANZCA recommends all patients undergoing major elective surgery should, if possible, have their HbA1C tested preoperatively4. This recommendation is in line with local policy at Austin Hospital, a tertiary level hospital in Victoria. The International Expert Committee recommends a diagnosis of diabetes be made if the HbA1C level is ≥6.5%5.
Aims
The aim of this audit was to establish the compliance of the Austin Hospital Upper Gastrointestinal and Endocrine Surgery (UGIS) Unit to the Austin Hospital and ANZCA recommendation for preoperative HbA1C testing.
Methods
After research Ethics Committee approval (LNR/17/Austin/556) we performed a retrospective clinical audit to ascertain adherence to these recommendations. All patients undergoing elective major surgery (defined as requiring ≥2 night stay) under the UGIS were audited for the 2016/17 financial year. Austin Health utilises Cerner® electronic medical records that allows comprehensive electronic data capture and access to patient health information in the perioperative setting.
Results
We collected data from 191 consecutive patients. Of these patients, 25 (18%) had diabetes based on HbA1C testing. 113 (59%) had a preoperative HbA1C checked. Of the 78 patients who were not checked, 33 patients had their HbA1C ordered in the immediate postoperative period. HbA1C testing in this group of patients was checked as part of an automated system which operates at Austin Health. This system ensures that all patients aged ≥54 years who have a >24-hour admission and have not had an HbA1C ordered within three months have an automated order for HbA1C created. Of this group of 33 patients, 6 (18%) returned an HbA1C result of ≥6.5%. Breakdown by surgery type in those 78 patients not checked for HbA1C preoperatively is summarised graphically in Figure 1.
Conclusions
In this audit assessing compliance with preoperative HbA1C testing recommendations, 41% of patients did not have HbA1C checked. Further, a small percentage of these patients proceeded to major surgery with undiagnosed diabetes. Further education and more reliable mechanisms for checking HbA1C preoperatively are required. Implementation of an automated system for the ordering of preoperative HbA1C in surgical patients may increase adherence to current recommendations, improve patient outcomes and would likely be applicable to many healthcare services across Australia.

Breakdown by surgery type in 78 patients not checked for HbA1C
References
20
An innovation for audit in real world: 6-month report of Peripheral nerve block audit in private practice
Wakefield Anaesthetic Group
Introduction
Anaesthetists across the world are unable to do audits and are frustrated for many reasons. Many Anaesthetists in private practice rarely have the time and resources along with the imposition of fundamentally and experimentally strong clinical audit is such that it is not easily accommodated in day-to-day medical practice.
I developed an innovative mobile App (RAD App and database). This innovation is the first of its kind in the world of Regional Anaesthesia and enables practitioner to enter data at patient bedside through their smart phones/devices with continuous automated analysis.
Aims
A pilot trial of Regional anaesthesia database audit app (RAD app) in single practitioner private practice and report of 6 months data.
Methods
No Patient identifiable data is collected. Only procedure related data was collected and verbal consent from all eligible patients was obtained. It involved complete peri-operative data entered on smart phone prospectively at the patient bedside. Basic descriptive statistics and national comparative data is built in the database.
All patients who had peripheral nerve blocks were added to the database.
Results
Date range: 2/11/2017 to 2/5/2018
A total of 59 cases and 70 PNBs were recorded
88% of patients had correct site check.
45% of patients had block under GA
7% of the patients had block as sole anaesthetic.
73% of all blocks were done under Ultrasound.
Ropivacaine was used 93% of the blocks in the dose of 2.09 ± 1.14 (mg, mean ± SD).
No failures were reported.
18% of patients had opioid free anaesthesia
81% of patients did not require any analgesics in recovery. 96% of patients had mild pain (VNRS 0-4) in recovery.
No complications were noted
Conclusions
The audit was done with minimal effort. It reflects my private practice. Such data has never been reported in literature.
Some improvement is needed in achieving 100% correct site check, reducing the dose of ropivacaine, improve sterility of Ultrasound probes and achieve better follow-up rates.
Currently there is no existing system to enable busy practitioners to do regular audits and have national database for benchmarking. This innovation will improve audit participation, provide real world data to national database and potential to improve safety and quality of regional anaesthesia practice.


21
Detailed assessment of benefits and risks of retrievable inferior vena cava filters on patients with complicated injuries: the da Vinci multicentre randomised controlled trial
1Department of Intensive Care Medicine, Royal Perth Hospital & School of Population & Global Health, University of Western Australia, Western Australia
2Department of Neurosurgery, Royal Perth Hospital & Sir Charles Gairdner Hospital, Western Australia
3State Trauma Unit, Royal Perth Hospital, Western Australia
4State Trauma Unit, Royal Perth Hospital, Western Australia
5Department of Intensive Care Medicine, Charles Gairdner Hospital, Western Australia
6Critical Care Services, Royal Brisbane and Women’s Hospital & University of Queensland, Queensland
7Critical Care Services, Royal Brisbane and Women’s Hospital & University of Queensland, Queensland
8Centre for Implant Technology & Retrieval Analysis, Department of Medical Engineering & Physics, Royal Perth Hospital, Western Australia
9School of Population & Global Health, University of Western Australia, Western Australia
10School of Medicine and Pharmacology, University of Western Australia, Western Australia
11Department of Radiology, Royal Perth Hospital, Western Australia
12Department of Intensive Care Medicine, Fiona Stanley Hospital, Western Australia
13Western Australian Centre for Thrombosis and Haemostasis, Murdoch University, Western Australia
14Trauma Services, Lancaster General Hospital & University of Pennsylvania, Lancaster, Pennsylvania
Introduction
The most appropriate strategy to prevent symptomatic pulmonary embolism (PE) in major trauma patients with contraindications to anticoagulant thromboembolic prophylaxis is uncertain. Despite a lack of high-grade evidence, inferior vena cava filter (IVCF) has been increasingly used globally as a primary means to prevent symptomatic PE in such patients.
Aims
This study aimed to assess whether early prophylactic inferior vena cava filter (IVCF) use could reduce symptomatic pulmonary embolism (PE) and/or mortality in major trauma patients with contraindications to anticoagulant thromboembolic prophylaxis.
Methods
In this multicentre randomised-controlled-trial, 240 major trauma patients — with an estimated Injury Severity Score (ISS) >15 and contraindications to anticoagulants between June 2015 and December 2017 — were randomly allocated to receive a retrievable IVCF or no IVCF within the first 72 hours of trauma admission. The primary outcome was a composite of 90-day mortality or symptomatic PE; and secondary outcomes were lower limb deep vein thrombosis (DVT), and symptomatic PE for those who did not receive anticoagulant prophylaxis within 7 days after trauma. All patients received screening lower limb Doppler ultrasound to exclude DVT within 2 weeks, and mandatory computed tomography pulmonary angiography to exclude PE when preset objective criteria were met.
Results
The median age and ISS of the patients were 39 years and 27, respectively. Early IVCF did not significantly reduce the primary outcome compared to no IVCF (13.9% vs 14.4% respectively; log rank test: P=0.98). IVCF did not increase the incidence of lower limb DVT compared to no IVCF (11.4% vs 10.1% respectively; P=0.84), and in those who did not receive anticoagulant prophylaxis within 7 days after major trauma, IVCF significantly reduced symptomatic PE compared to no IVCF (N=80; 0% vs 14.7% respectively; P=0.01). This difference remained changed using cumulative incidence competing risk — between mortality and symptomatic PE — analysis (see
Conclusions
Early prophylactic IVCF use within 72 hours after major trauma did not reduce the composite outcome of 90-day mortality or symptomatic PE. For patients who could not receive anticoagulant prophylaxis within 7 days after major trauma, early IVCF significantly reduced symptomatic PE.

22
Predicting perioperative blood loss and transfusion requirement in adult cardiac surgery using multiple electrode aggregometry platelet function test: a cohort study
1Department of Intensive Care Medicine, Royal Perth Hospital & School of Population & Global Health, University of Western Australia, Western Australia
2Department of Anaesthesia & Pain Management, Royal Perth Hospital, Western Australia
Introduction
Platelets play a pivotal role in physiological haemostasis. Many cardiac surgical patients are treated with antiplatelet agents before surgery, and bleeding is common after cardiac surgery.
Aims
This study assessed whether the degree of platelet inhibition within 24 hours before cardiac surgery is associated with perioperative blood loss and allogeneic blood transfusion in elective adult cardiac surgery.
Methods
The degree of inhibition by aspirin, P2Y12-receptor-blocker and glycoprotein IIb/IIIa-blocker on the day before surgery was quantified by three channels using the Multiple Electrode Aggregometry (Multiplate®), after adding arachidonic acid, platelet adenosine-diphosphate (ADP), and thrombin-receptor-activating-peptide (TRAP) as platelet activation agent, respectively. Spearman correlation (r) and area-under-the-receiver-operating-characteristic (AUROC) curve were used to assess the quantitative relationships between platelet inhibition, blood loss and transfusion requirement.
Results
Of the 251 patients included in the study, the total blood loss until subcostal drains removal after surgery was related to the degree of platelet inhibition by aspirin (r=0.161, P=0.015)(see
Conclusions
Platelet inhibition by aspirin before cardiac surgery was weakly related to the amount of postoperative blood loss and transfusion requirement, but these associations were not sufficiently reliable to guide perioperative blood management. Our results do not support routine platelet function testing before elective adult cardiac surgery.

23
A Retrospective Review of Intra-operative Anaesthetic Factors Affecting Mortality After Hip Fracture Surgery
1Department of Anaesthesia, St George Hospital, Sydney, Australia
2Manly Hospital, Sydney, Australia
3Liverpool Hopsital, Sydney, Australia
4South Western Sydney Clinical School, Faculty of Medicine, University of New South Wales. Department of Anaesthesia, Liverpool Hospital, Sydney, Australia
Introduction
Hip fracture surgery is associated with 5.1–13.3% mortality at 30 days123. Anaesthesia interventions to reduce this high mortality has been largely unsuccessful. Recently, the UK Anaesthesia Sprint Audit of Practice identified control of intra-operative blood pressure as a possible factor in mortality.
Aims
To examine if intra-operative blood pressure control has effects on mortality after hip fracture surgery. To examine if other pre- and intra-operative factors influence mortality.
Methods
Retrospective review of all patients undergoing hip fracture surgery in Liverpool Hospital, Sydney, from 01 June 2014 to 30 June 2016. Medical, surgical and anaesthesia records were matched with 30-day and 120-day outcomes data from the Australian and New Zealand Hip Fracture Registry.
Results
1,020 Patients were stratified into 3 groups, based on excursion of intra-operative MAP from pre-surgery baseline: Tight MAP control group (≤12% below pre-surgery), intermediate (13–24% below pre-surgery), and loose (≥25% below pre-surgery). Groups were analysed using the Cochan-Mantel-Haenszel test with continuity correction to assess if MAP control was associated with 30- and 120-day mortality (4). There was no significant difference in mortality between these groups (p = 0.46).
Age at surgery, pre-surgery eGFR, pre-surgery cognitive status, post-surgery cognitive status, ASA score, pre-surgery orthogeriatric assessment, whether surgery was performed within 48 hours of admission, Nottingham Hip Fracture Score, and Charlson scores were statistically significant for association with 30-day mortality. In addition to these, at 120-days, pre-admission walking ability, the type of hip fracture, pre-surgery serum albumin, and MAC-hr were also statistically significant for association with mortality
However, on multivariate analysis only pre-surgery cognitive status, pre-surgery eGFR, and pre-surgery orthogeriatrics assessment were significant for 30-day mortality (p = 0.025). In addition to these variables, pre-surgery albumin and post-surgery cognitive status were significant for 120-day mortality (p = 0.04).
Conclusions
Intra-operative blood pressure control was not associated with mortality after hip fracture surgery. Of other factors identified as being associated with mortality, only two are under clinicians’ influence: timely orthogeriatrics input in patient management, and possibly measures to improve post-surgical cognitive status.
References
24
Hospital Readmissions for a Second Operative Hip Fracture in Older Patients
1Maroondah Hospital, Eastern Health and Faculty of Medicine, Nursing and Health Sciences, Monash University
2Maroondah Hospital, Eastern Health
Introduction
Hospital performance is often measured by the number of readmissions following a specific surgery. Readmissions following hip fracture surgery are not uncommon, reported up to 32.0% at a year, and mostly attributed to medical complications1.
Many older people presenting with a hip fracture have osteoporosis, which increases their risk of a secondary fracture2. As such, a proportion of the quoted readmissions would be due to another hip fracture after initial hospitalization, but these rates of readmissions are rarely reported.
Aims
This study aims to estimate the hospital readmission rate for a second operative hip fracture in older patients within a year of initial surgery and to determine the period until readmission.
Methods
This is a retrospective exploratory study conducted at a metropolitan hospital for admissions between 2011-July and 2015-July. Patients included were 65 years and older, their admission diagnosis was hip fracture and they underwent surgical repair.
After institutional ethics approval, the hospital database identified 1221 patients who met the inclusion criteria, of whom, 20 patients were subsequently readmitted for another operative hip fracture (periprosthetic or contralateral).
The following data for these 20 patients were extracted and analyzed: age, gender, date of discharge from initial hospitalization, readmission date and diagnosis. Based on the collected data, the days between admissions for operative hip fractures (DOHF) were calculated, which is defined as: the period from the initial hospital discharge to readmission.
Results
Most patients (75%) were female, with an average age of 82 years (range 66-92). Among them, 5 patients had periprosthetic fractures (PPF), 14 suffered from contralateral hip fractures, and one patient experienced both and was readmitted twice.
The results indicated that, over the 4-year study period, about 1.7% of older patients were readmitted for a second hip fracture surgery, either suffering from contralateral hip fracture (1.2%) or PPF (0.5%) with a median DOHF of 187 (IQR 57-405). Of concern, over three quarters (76%) of these hip fractures happened within a year after hospital discharge (Figure 1), representing an overall one-year readmission rate at 1.3%.
In our study, all of the 6 PPF’s were readmitted in the first postoperative year with a median DOHF of 88 (IQR 22-209), accounting for 0.5% of the readmission rate.
Conclusions
In conclusion, at least 1.3% of older patients would return to the original hospital for a second hip fracture surgery during the first postoperative year. Among them, 0.5% sustained PPF, which is a well-recognized serious and complex injury after surgical treatment.
However, these findings may be significantly underestimated, since such data are only available for readmissions to the original hospital where the initial surgery was performed, and also errors and omissions can occur with hospital databases.
While this study is limited by the sample size, study period and retrospective analysis, further studies are warranted to assess such re-admissions on hospital performance and the impact on the wider community, in particular, clinical and health economic implications on medical practice and community services.

When do the hospital readmissions occur for a second operative hip fracture?
References
25
Nervous Survey: Prevalence of Persistent Peripheral Neuropathy in Adult Patients Who Received Perioperative Nerve Blocks
1Clinical School at Eastern Health, Deakin University
2Maroondah Hospital, Eastern Health and Faculty of Medicine, Nursing and Health Sciences, Monash University
Background
Peripheral nerve blocks (PNB) are widely performed with excellent postoperative analgesia. However, some perioperative peripheral nerve injuries (PPNI) are attributed to regional blocks, with permanent injury accounting for 0.04% blocks1.
While the etiology of PPNI is complex and often multifactorial, direct nerve damage from invasive procedures is generally considered the main culprit. As such, it is extremely difficult to distinguish block-related PPNI from the surgery as both invasive procedures performed at the same nerve/plexus distribution area. To further complicate this issue, the clinical manifestation of nerve damage is usually delayed; as a result, PPNI is often under reported since a majority of these patients have already been discharged.
Regardless of the causes, persistent postsurgical peripheral neuropathy (PPSN), defined as the presence of a new or worsened sensorimotor deficit 6 months post-surgery2, remains a medical challenge with potential for long term disability. Hence, it is particularly important for early diagnosis and intervention before becoming permanent.
Aims
This study aims to establish a baseline prevalence of PPSN in patients who received perioperative PNB up to 6 months after surgery.
Methods
At our hospital, audit forms were filled in after a regional block by the attending anaesthetist. These forms constituted our database.
After local ethics approval, a telephone interview was conducted at postoperative 6-month or later, in which patients were asked if they experienced clinically relevant PPNI symptoms after discharge.
Results
Of the 173 eligible patients from 2017-Q1, data from 116 patients (20 breast surgery, 15 upper-limb and 81 lower-limb) were included and analysed (dropout reasons see
Our results indicated that after hospital discharge, while 21% patients never had any PPNI symptoms, 67 patients (57%) experienced pain with or without paraesthesia/weakness, and 25 (21%) suffered from paraesthesia/weakness without pain.
Despite significant improvement over the time, PPNI symptoms sustained in 42 patients (9 breast, 3 upper-limb and 30 lower-limb) beyond 6 months after surgery, accounting for a prevalence of PPSN 36% of our cohort.
Discussion
This survey is limited by sample size, retrospective data and lack of objective medical evaluation for those PPSN symptoms, in particular, the latter may well produce a Hawthorne effect that could lead to an overestimated prevalence3.
Indeed, our results are unexpected, with a much higher incidence of PPSN (36%) than the existing evidence. However, this study indicated an unsatisfying result of surgical intervention in terms of postdischarge PPNI control, thus, further studies are necessary with a view to improve PPSN management strategies after discharge.
References
26
Whose Care Can We Optimise? Incidence of Preoperative Anaemia in Elective General Surgical Patients Who Required Perioperative Blood Transfusion
Royal Brisbane & Women’s Hospital & The University of Queensland, Brisbane, Australia
Introduction
The adverse effects of allogenic blood transfusion (ABT) are becoming increasingly apparent. The link between preoperative anaemia and the need for perioperative ABT has been established. Preoperative anaemia has been associated with increased morbidity (increased infections, cardiovascular complications, length of hospital stay and need for intensive care admission) and both short- and long-term mortality. Preoperative optimisation of haemoglobin (Hb) can lead to improved outcomes. Patient Blood Management (PBM) is an evidence-based approach to patient care and its first principle refers to preoperative optimisation of Hb.
Aims
The aim of this study is to evaluate the proportion of elective general surgery patients at a quaternary hospital that could potentially benefit from a PBM approach to care.
Methods
All patients who required perioperative ABT with elective general surgical procedures at the Royal Brisbane Hospital between January 1st and June 30th 2016 were identified. Patient charts were retrospectively analysed to obtain patients’ preoperative Hb.
Results
Twenty elective general surgical patients required perioperative ABT during this timeframe of the study. Table 1. Nine (45%) were male and eleven (55%) were female. The mean age was 65 years (range 46-84 years). Fifty percent (n = 10) of patients were anaemic prior to surgery according to the World Health Organisation definitions of anaemia (Hb < 120g/L in women, Hb < 130g/L in men). Men were more likely to be anaemic than women (66% vs. 36%, respectively). The median and mean amounts by which patients were anaemic were both 25g/L (range 8 to 59g/L). Severe anaemia (Hb < 80g/L) was present in one patient with a Hb of 71g/L. The total number of patients (men and women) who had an Hb of < 130g/L the day prior to surgery was 13 (65%), with three women having an Hb 120-129g/L. Whilst the burden of perioperative ABT was borne generally by the colorectal and hepatobiliary subspecialty teams of general surgery, hepatobiliary patients were not found to be preoperatively anaemic in this study compared to colorectal patients.
Conclusions
Despite strong evidence for worse patient outcomes with preoperative anaemia and the need for perioperative ABT, there remains a large number of patients–especially ‘colorectal’ patients–whose care could be improved through practices such as PBM. Adopting the whole spectrum of PBM practice is imperative for all Australian hospital and patients, and anaesthetists are well-positioned to take the lead for the perioperative aspect of this.
Figure 1: The incidence of preoperative anaemia (Hb <130g/L in men, Hb <120g/L in women) broken down by surgical procedure subgroup with the percentage of patients per procedure group who were anaemic.
Rates of preoperative anaemia broken down by gender.

The incidence of preoperative anaemia (Hb <130g/L in men, Hb <120g/L in women) broken down by surgical procedure subgroup with the percentage of patients per procedure group who were anaemic.
30
Anaesthetic Management in Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in a Tertiary Care Institution in Southeast Asia: A Retrospective Review
1National University of Singapore, Singapore
2National University Health System, Singapore
3Singapore General Hospital, Singapore
Introduction
Cytoreductive surgery (CRS) combined with hyperthermic intraperitoneal chemotherapy (HIPEC) has become a cornerstone of treatment of peritoneal-surface malignancies. It is a complex procedure necessitating special anaesthetic considerations and techniques. This retrospective review conveys our centre’s experience in anaesthetic care.
Aims
Given the scarcity of local data involving HIPEC, we aim to describe the clinical background of patients undergoing CRS/HIPEC from 2015 to 2017 in a tertiary care institution in Singapore. Key variables analysed include comorbidities, demographics, and nature and extent of disease. We also aim to comprehensively analyse and evaluate aspects of anaesthetic management and clinical course of these patients during this review period. This would give us greater insights into the optimal anaesthetic principles for managing HIPEC surgery with the aim of improving clinical outcomes for this group of patients.
Methods
After Centralised Institutional Review Board (CIRB) approval, the relevant electronic patient records were retrospectively reviewed for patient characteristics, anaesthesthetic management, postoperative disposition and complications. Descriptive statistics are presented as median (range), and univariable linear regression was used to identify factors independently affecting intra-operative anaesthetic management and postoperative progress.
Results
Between 2015 and 2017, a total of 113 consecutive patients underwent 118 CRS/HIPEC interventions. 67.8% of patients were female. The median age was 67 years old. The most common primary tumour sites were colorectal, appendix and ovary. There were 5 patients who underwent repeat CRS/HIPEC within 1-2 years for primary tumour recurrence. Median anaesthesia time was 455 (range 202-857) minutes. 8 patients were given adjuvant thoracic epidural anaesthesia (TEA), requiring reduced intra-operative opioid use. Post-operatively, major complications occurred in 8 patients which led to mortality in 3 patients.
Increased length of hospital stay was associated with longer intra-operative time and anaesthetic duration. Respiratory and neurological co-morbidities were also shown to lead to increased length of hospital stay. The rate and severity of surgical complications was also shown to have a positive correlation with total anaesthetic duration and intra-operative time, and was also significantly associated with an increased dose of morphine per weight and blood-products given intra-operatively.
Conclusions
CRS with HIPEC is a challenging procedure involving multifaceted aspects of anaesthetic care. It is associated with major hemodynamic and physiological derangements intra-operatively. This review has shown that several factors such as primary disease, anaesthesia management, and amount of blood transfusions have a significant effect on patients’ outcome.
Keywords
Anaesthesia, Hyperthemic Intraperitoneal Chemotherapy, Postoperative outcome
33
Hashtag Analysis of Social Media (#ASM)
Department of Anaesthesia and Acute Pain Medicine, St. Vincent’s Hospital Melbourne
Introduction
Social media is increasingly used in academic and scientific circles. One of the most popular platforms is Twitter, which is characterised by brief messages up to 280 characters and the use of ‘hashtags’ to categorise content. Each message is termed a ‘tweet’ and may contain multiple hashtags, which help users find relevant tweets.
The Australian and New Zealand College of Anaesthetists (ANZCA) has been encouraging fellows and other stakeholders to engage via Twitter. This was particularly evident at the 2018 Annual Scientific Meeting (ASM) in Sydney from 7-11 May. A dedicated hashtag was used for this event, #ASM18SYD, and a guide was created to help delegates use Twitter1.
Many benefits have been linked with social media for conferences, including networking with other conference delegates, discussing ideas related to the conference, and sharing content with those unable to attend a session (both delegates and non-delegates). Given the time and resources being used to engage with social media and promote its use, it is of interest and value to analyse data related to its use and impact.
Aims
To characterise patterns of Twitter use, engagement and reach associated with the ANZCA 2018 ASM.
Methods
Twitter activity involving the hashtag #ASM18SYD was analysed using the commercial analytics platform ExportTweet2. This analysis included all tweets from 2 May 2018 21:08:21 UTC to 13 May 2018 10:29:49 UTC.
Results
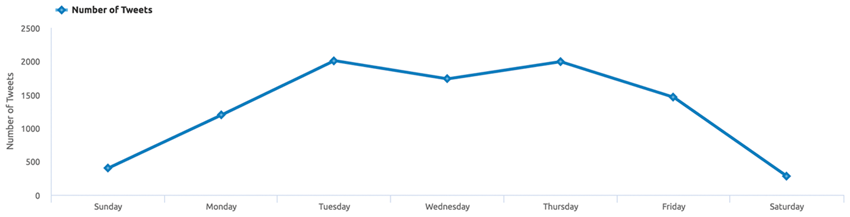
A total of 9,074 tweets were made by 1,495 users (average 6.07 tweets per user). While not all tweets were made by conference attendees, this is equivalent to 62.2% of all ASM delegates.
There were 2,571 (28.33%) original tweets, 6,268 (69.08%) retweets and 235 (2.59%) replies. 21.59 million impressions were made (average 2,380 per tweet and 14,440 per user) and 3.92 million accounts were reached (average 431 per tweet).
English was the primary language in 98.9% of tweets. Devices used to tweet were: iPhone (70.7%), Android (9.8%), web client (9.2%), iPad (7.7%), other (2.6%).
The daily pattern of tweets is shown in Figure 1.
Conclusions
The #ASM18SYD hashtag achieved extensive engagement and reach. This suggests that Twitter is an effective platform for conferences to engage attendees, promote discussion and disseminate content.
References
35
The hidden secret of High Reliability Organisations: practical application to anaesthetic care
1University of Calgary, Calgary, Canada
2Alberta Health Services, Calgary, Canada
Introduction
High reliability organisations (HROs) are those demonstrating “continuously the capacity to provide expected levels and quantity of services, without off-setting failures of critical processes”.1 For the past 20 years, HROs have been an exemplar for healthcare organisations, with suggestions that adopting similar practices could help make healthcare safer.2 However, healthcare organisations continue to struggle to be as safe as HROs. One reason is that providing healthcare is not equivalent to airline transportation or nuclear power generation. We believe a second reason, the secret to HROs’ success, lies in the initial HRO studies.
Aims
Our aims were to prove our hypotheses that:
• individuals’ ability to function at a high level in HROs was related to the organisation’s structural standardisation, upon which reliable performance of activities (process) is dependent; and by whom and why the initial HRO studies were undertaken influenced their findings and subsequent publications.
Methods
We reviewed the 1987-88 and selected recent HRO publications.
Findings
One seminal publication was a study conducted on the USS Carl Vinson, an American aircraft carrier. The paper contained the key phrase, the “Navy itself is of course the underlying structural determinant”.1 Standardisation of structure was recognised as vital but otherwise minimally described. The studies were conducted by a group of political, computer, social and organizational scientists and psychologists at Berkeley University, interested in organizational and individuals’ performance, i.e., process. The most recent HRO publications continue to emphasise HRO-like processes and not structure.3
We think that, in contrast to these HROs, healthcare cannot achieve similar high performance, partly because little of the structure of care (including our patients, the focus of activities) is standardised, leading to variable process of care. To counter this problem, the Calgary Department of Anesthesia is standardising as much equipment as possible, including the emergency bag-valve-mask location in Operating Rooms. We are also working to standardise anaesthetic medications and their drug cart layout on a province-wide basis, as part of development/implementation of a new provincial, computerised healthcare record. Our goal with this project is not to standardise process of care but structure of care, recognising that structure drives process.4,5 For example, standardised structure helps reduce cognitive load, thus facilitating decision-making.6
Conclusions
Healthcare will never match HROs’ outcomes, partly because our patients have highly variable, complex care needs. However, we think standardising equipment will contribute to our healthcare organisations having higher performance reliability in the provision of anaesthetic care.
References
36
The Health Economic Impact of Postoperative Complications Following Liver Resection
1Department of Anaesthesia, Austin Health, Victoria
2Department of Finance, Austin Health, Victoria
3The Florey Institute of Neuroscience and Mental Health, Victoria
4Clinical Information Unit, Austin Health, Victoria
5University of Melbourne, Department of Surgery, Austin Health, Victoria
Introduction
Liver resection carries a high economic cost, and despite improvements in perioperative care postoperative morbidity remains high. The impact of postoperative complications on the cost of liver resection is poorly quantified, and there remains little data demonstrating where these costs occur.
Aim
To identify the relationship between the extent of liver resection, the incidence and severity of complications, and the ensuing costs. Additionally, we sought to examine the sources of cost differentials between complicated and uncomplicated patients.
Methods
Complications for 317 consecutive patients undergoing liver resection at the same institution were recorded using the Clavien-Dindo classification. Patients were stratified based on the grade of their worst complication to assess the impact of morbidity on resource use of specific cost centres. Cluster analysis was performed to identify homogenous groups based on resource use.
Results
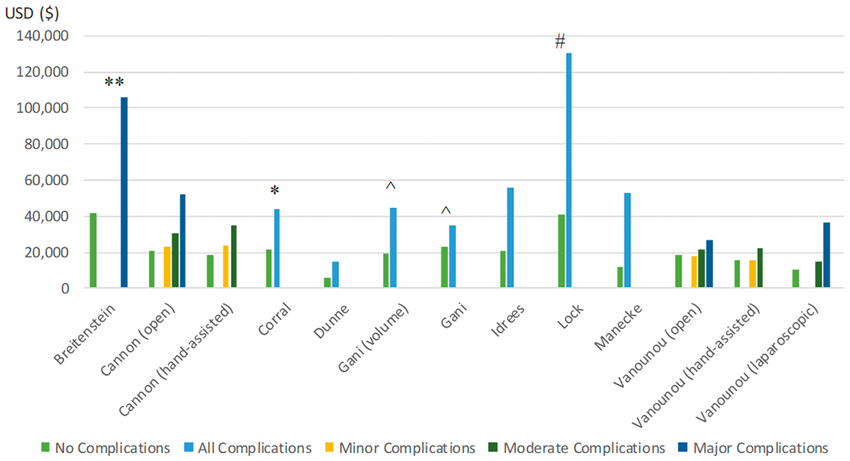
Morbidity dramatically increased hospital cost ($31,259 vs $16,884, p < 0.001). Major resection cost more than double minor resection and carried greater morbidity (82% vs 59%, p < 0.001). Similarly, patients having open resection cost more than those having laparoscopic surgery ($29,731 vs $16,559, p < 0.001) and experienced higher rates of morbidity (72% vs 41.5%, p < 0.001). Morbidity increased costs across all cost centres, but predominantly in the ward, ICU, and medical consult cost centres. Minor complications were shown to significantly increase costs, despite often being clinically menial.
Conclusion
Liver resection continues to carry high rates of morbidity, and these carry a substantial economic burden. Hospital cost and length of stay increase with greater severity and number of complications. Minor complications present an important target for cost reduction strategies.
Figure 1: hospital costs (2018 USD) by cost centre and severity of complications.
hospital costs (2018 USD) by cost centre

37
The health economic implications of postoperative complications following liver resection surgery: a systematic review
1Department of Anaesthesia, Austin Health, Victoria
2Department of Finance, Austin Health, Victoria
3The Florey Institute of Neuroscience and Mental Health, Victoria
4University of Melbourne, Department of Surgery, Austin Health, Victoria
Introduction
Limited data exists concerning the health economics of liver resection, with even less information on the costs emerging from complications, despite this remaining an important target from a health economic perspective.
Aims
We aimed to describe the financial burden of complications following liver resection.
Methods
We searched articles using the MEDLINE, EMBASE, Cochrane and EconLit databases. We included studies reporting on hospital cost or charge of in-hospital complications during the index liver resection admission. All indications for liver resection were considered. All techniques were considered. Data was collected using a data extraction table and a narrative synthesis was performed
Results
We identified 12 eligible articles. There was considerable heterogeneity in study designs, patient populations and outcome definitions. We found weak evidence of increased costs associated with major liver resection compared to minor resections. We found robust evidence supporting the increasing economic burden arising from complications after liver resection. Acceptable evidence for increased cost due to the presence and grade of complication was found. Strong evidence concerning the association of length of stay with costs was demonstrated.
Conclusions
The presence and grade of complications increase hospital cost across diverse settings. The costing methodology should be transparent and complication grading systems should be consistent in future studies.
Cost of complications for liver resection surgery (data presented as mean unless otherwise stated).
38
Mechanism of cellular uptake of the excitotoxin quinolinic acid in primary human neurons
1Intensive Care Senior Resident Medical Officer, Royal Prince Alfred Hospital, NSW
2Centre for Healthy Brain Ageing, University of NSW
3Neurodegenerative Diseases Research Centre, Macquarie University NSW
4Drug Delivery, Disposition and Dynamics, Monash University, VIC
Introduction
The Kynurenine pathway (KP) metabolises and is involved in the pathogenesis of neurodegenerative diseases. The KP metabolite quinolinic acid (QUIN) contributes to neuroinflammation in Alzheimer’s disease. In neuroinflammatory states, activated microglia and macrophages produce excess QUIN that accumulate within the brain parenchyma and dystrophic neurons. QUIN also modulates glutamate uptake into neurons, through the excitatory amino acid transporters (EAATs). Deregulation of the KP in neuroinflammatory diseases leads to QUIN overproduction. QUIN is up-taken into neurons where it accumulates leading to cell death. Despite this, the mechanism(s) of how QUIN is transported into neurons remains unknown.
Aims
1. Quantify the cellular uptake of exogenous QUIN in human primary neurons. 2. Significantly attenuate QUIN uptake. 3. Co-localise QUIN with a molecular transporter and demonstrate increased transporter protein expression when exposed to QUIN
Methods
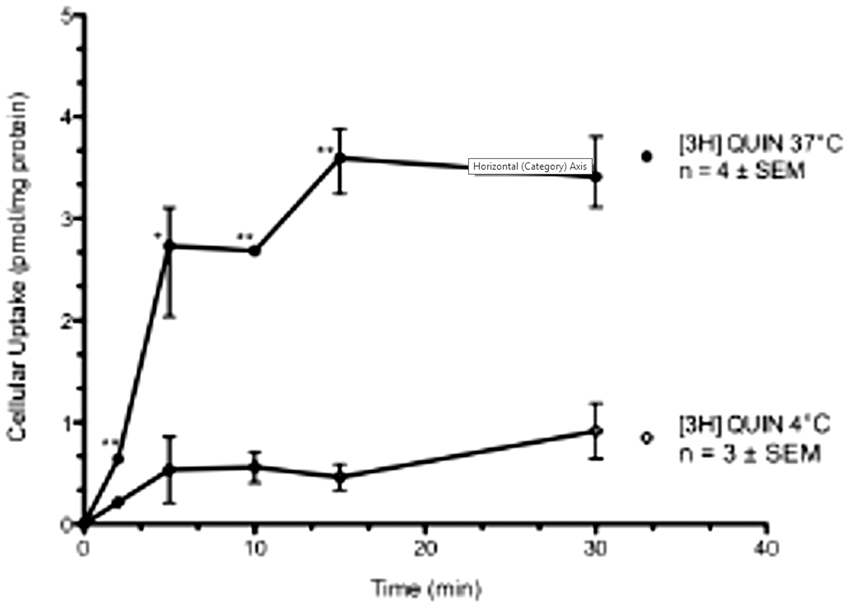
Using human neuronal cultures the pharmacokinetics of QUIN was quantified using radiolabelled [3H]QUIN uptake assays and measured with a scintillation counter with concentration and time-dependent endpoints. Using these results [3H]QUIN uptake was assessed in the presence of transport inhibitors. Significance from control was determined by Student’s t-test. Immunocytochemistry and confocal microscopy was used to qualitatively co-localise QUIN with a molecular transporter and analyse increased receptor protein expression. Our positive control was the NMDA-receptor which QUIN is a known agonist. Immunostaining with MAP2 demonstrated pure neuronal cultures.
Results
We found that QUIN increases expression of EAAT protein and co-localises with the receptor. We also found a significant temperature-dependent high affinity transporter leading to neuronal uptake of [3H]QUIN with a Km of 42.2 μM, and a Vmax of 9.492 pmol/2min/mg protein (n = 4), comparable with the uptake of glutamate through EAAT. Furthermore, QUIN uptake into primary neurons was shown to involve EAAT3, as uptake was significantly attenuated with the EAAT inhibitor L-trans-Pyrrolidine-2,4-dicarboxylic acid.
Conclusions
This study is the first to characterise a mechanism for QUIN uptake into primary human neurons and the involvement of EAAT. Our pharmacological data suggests that QUIN is transported into neurons via an active, high-affinity and saturatable receptor. Our kinetics are similar to the neuronal glutamate receptor, EAAT3 shown by other groups. We co-localised QUIN with the EAAT transporter and the fact that high levels of exogenous QUIN increased EAAT3 protein expression further supports our pharmacological data that EAAT3 is responsible for QUIN transport. We significantly antagonised QUIN uptake, which may prevent cell death and be relevant for the development of targeted noval therapies for neuroinflammatory diseases.
39
Addressing The Need For Regional Anaesthesia Training
Department of Anaesthesia, St George Hospital, Sydney, Australia. Faculty of Health Sciences, Australian Catholic University, Melbourne, Australia
Introduction
Advances in anaesthetic practice have seen an emergence of novel techniques and new training competency requirements by the Australia and New Zealand College of Anaesthetists (ANZCA)1.
It can be challenging for ANZCA trainees to achieve these competencies during their relatively short training period. Regional anaesthesia skills training is not uniform across training hospitals. Trainees’ volume of practice (VOP) is largely dependent on the surgical case-load, surgeons’ preferences and the resources available in their training hospitals, in addition to their supervisors’ skills.
Aims
To assess if current regional anaesthesia skills training is adequate in meeting the ANZCA training requirements.
To make recommendations for developing a centralized simulation education program to address any training needs identified.
Methods
An anonymous online questionnaire was sent to current anaesthetic trainees at various levels of training and different training hospitals via email, SMS and social media.
Results
Of the 52 trainees who completed the questionnaire, 58% had received at least one formal regional anaesthesia training session. Of these, 97% felt that this had improved their skills.
77% of trainees believed that they are not receiving adequate regional anaesthesia training and that their skills do not meet the ANZCA competency requirements.
83% of trainees believed that they do not have enough VOP in regional anaesthesia. 84% of these attributed this to lack of regional anaesthesia proceduralists able to teach trainees, with 62% attributing this to time pressure in clinical settings.
94% of participants believed that they would benefit from dedicated regional anaesthesia training, with 58% of trainees choosing advanced training as the most appropriate time for this.
98% of participants would attend regional anaesthesia skills workshops and 94% were interested in accessing online educational material.
83% of participants found video demonstrations to be good for teaching clinical skills followed by mobile phone applications (50%) and online e-modules (45%).
In the 54% of participants who’d received skills training on cadavers, 82% found this to be a good teaching method and of the 56% of participants who’d had skills training on phantom models, 76% scored this as a good teaching method.
All participants believed that multi-modal teaching would enhance their learning.
Conclusions
We have identified the need for improving regional anaesthesia training amongst ANZCA trainees.
We have made recommendations for implementing a coordinated systemic approach to developing a cost-effective multi-modal simulation program to address the learning objectives and training requirements of the new ANZCA curriculum1.
We have discussed the benefits of implementing such a program and provided recommendations for addressing any potential difficulties.
References
41
An audit of ROTEM guided management of bleeding in cardiac surgical patients at a major tertiary teaching hospital using a case control study
1Department of Anaesthesia, Royal Adelaide Hospital
2Department of Cardiothoracic Surgery, Royal Adelaide Hospital
3Med VI University of Adelaide
4Department of Anaesthesia, Royal Adelaide Hospital
5Department of Anaesthesia, Royal Adelaide Hospital, Senior Clinical Lecturer, The University of Adelaide
Introduction
Bleeding complications after cardiac surgery are common and are associated with morbidity and mortality.1 Point of care whole blood viscoelastic testing (e.g. Rotational Thromboelastometry, ROTEM) is rapid and allows timely decisions for targeted intervention2. Management of coagulopathy guided by ROTEM based algorithms have been shown to reduce the use of blood products for patients with postoperative bleeding2.
As ROTEM is relatively new in our institution we decided to assess whether clinicians are prescribing blood products appropriately in response to ROTEM testing. We audited cardiac surgical patients returning to theatre for surgical exploration for excessive postoperative bleeding over a three-month period.
Aims
To identify areas for quality improvement, this project analysed the current use of ROTEM in cardiac surgery patients in a major tertiary teaching hospital, by comparing the management of patients who had ROTEM tests and returned to theatre for bleeding with those who did not return to theatre.
Methods
Following ethics approval, the Australian and New Zealand Society of Cardiac and Thoracic Surgeons (ANZSCTS) database was used to identify all patients who returned to theatre for bleeding and had a ROTEM between 1st January 2018 and 31st March 2018.
Control cases were identified from the database and matched using the Papworth bleeding risk score.3
Other databases used in this study included: hospital laboratory reporting systems and automated patient record keeping systems. The following data were collected to identify controls: age, BMI, type of surgery, urgency of surgery, aortic valve disease.
The following outcome measures will be collected for comparison:
ROTEM variables– a blinded investigator will interpret results and provide treatment recommendation
1. Red blood cell and non-red blood cell transfusion rates and times
2. Postoperative drain output (4 hours)
3. Surgically determined site of bleeding
4. Society of Thoracic Surgery risk score (STS score)4
5. Tranexamic acid dose (total) and mode of administration
6. Preoperative antiplatelet use and days of cessation
7. Lowest temperature and temperature on admission in CTICU
8. Decrease in haemoglobin (% and absolute)
9. Acute kidney injury (AKI) via KDIGO classification
10. Mortality at 30 days
All data collected were de-identified and stored securely.
Results
Data will be presented primarily as summary statistics (means with standard deviation or medians with range depending on data distribution). Regression models will then be performed, one for each defined outcome from the list above versus the predictor: whether the patient returned to theatre to control bleeding or not. The Papworth bleeding risk score will be included as a confounder.5
References
42
Preoperative fasting: assessing compliance with guidelines and patient understanding at a tertiary referral centre
1The Royal Brisbane and Women’s Hospital, Queensland
2The Prince Charles Hospital, Queensland
3University of Queensland
Introduction
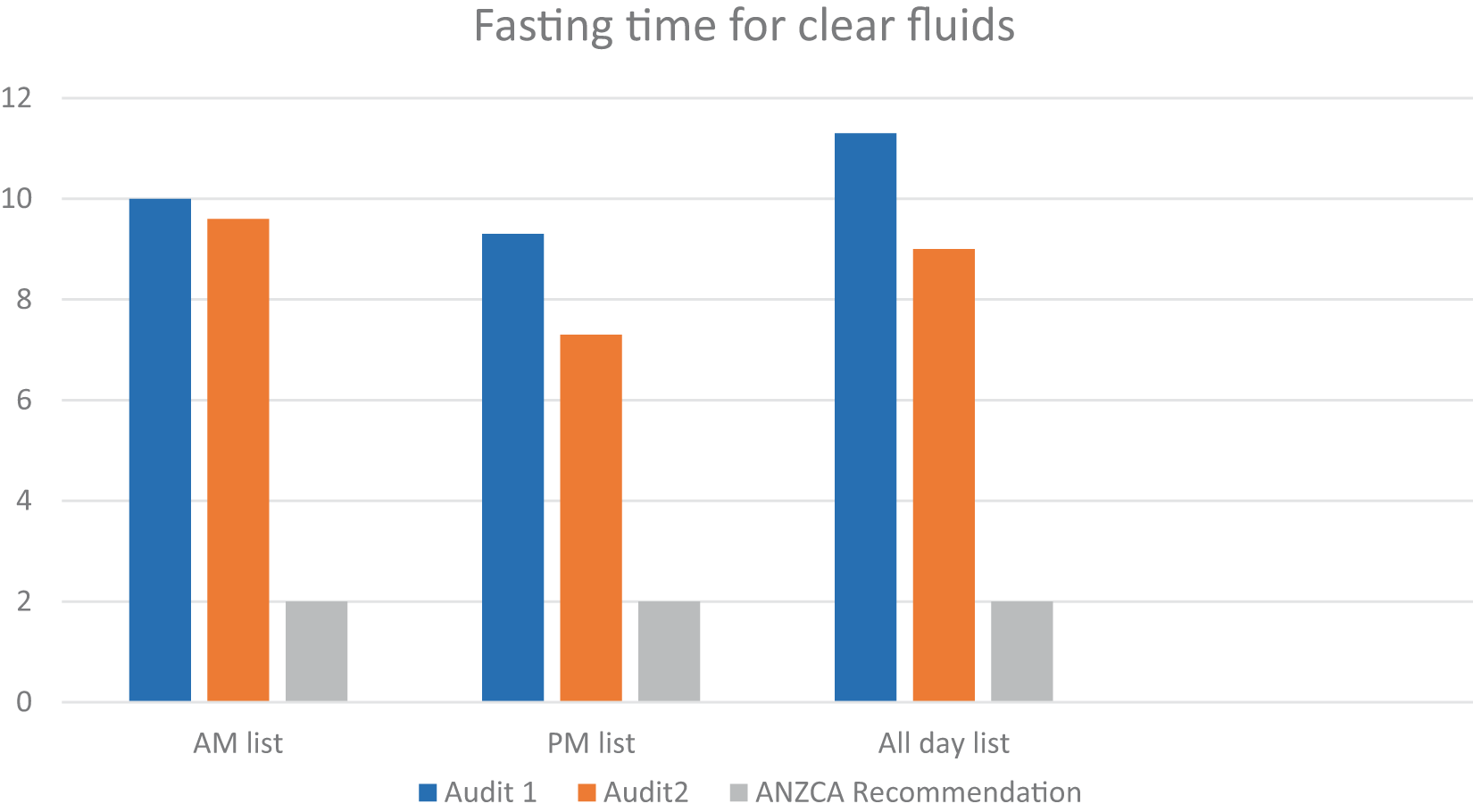
ANZCA guidelines recommend a period of fasting for 6 hours for limited solid food and clear fluids up to 2 hours prior to anaesthesia1 for elective surgical procedures. Pre-operative fasting results in a state of thirst, hunger and often objective dehydration. Preoperative drinks containing carbohydrates may improve the post-operative course by reducing postoperative nausea and vomiting2, prepare the patient for surgical stress3,4and improve patient satisfaction4,5.
Aims
This prospective audit aimed to evaluate pre-operative fasting times among patients undergoing elective surgery, patient understanding of fasting instructions and impact of fasting on patient well-being.
Methods
With exemption from the institutional ethics committee, the initial audit conducted in September-October 2017 surveyed 145 elective surgical patients admitted through the day surgical unit at the Prince Charles Hospital (TPCH) on the day of surgery using a patient questionnaire about the duration of fasting, fasting instructions subjective symptoms. The results were compared with ANZCA fasting guidelines1. This audit highlighted poor compliance with the fasting recommendations and explicit guideline implementation and staff education involving the anaesthetists, surgical and nursing staff followed. The audit was repeated 3 months after these measures were taken.
Results
The first audit involved 143 patients and the second audit included 145. The initial audit showed fasting times to exceed the ANZCA guidelines especially for clear fluids, with mean duration of 11hours (h) 5minutes (m) (range: 3h5m-18h27m). With the repeat audit, this reduced to 9h18m (range:3h-18h1m). These results were analysed based on the surgical lists, being divided into morning, afternoon and all-day lists. We assessed patient understanding of instructions and their subjective feelings of thirst, hunger, tiredness and dehydration. 100% of the patients in the second audit understood the need to fast as opposed to 83% in the first audit.
Conclusions
Pre-operative fasting aims to optimise patient safety by reducing the risk of aspiration of gastric contents and pulmonary injury. Prolonged fasting however has several adverse effects. This audit process was the first step in the minimisation of prolonged fasting through establishing effective communication between treating teams. A better patient understanding of the need for preoperative fasting was noted with the re-audit. Although there was a reduction in the fasting time for clear fluids, there is clearly scope for further improvement. There is a need for further staff education, encouraging patients to drink or even provide a drink to patients awaiting surgery up to 2 hours pre-operatively.
Graph 1 Comparison of results: Mean fasting time for clear fluids
Bibliography
43
Preoperative fasting: assessing compliance with guidelines and patient understanding at a tertiary referral centre
1Eastern Health, Victoria, David Cui, Eastern Health, Victoria, Alice Jiang, Eastern Health, Victoria, Richard Hiscock, Epworth Eastern & Mercy Hospital for Women, Victoria
2Eastern Health, The Royal Victorian Eye and Ear Hospital & Monash University, Victoria
Introduction
Perioperative analgesia in fractured neck of femur (#NOF) patients is challenging as patients tend to be elderly with more medical co-morbidities. Both increased opioid use and poor pain control are associated with increased rate of delirium, length of stay, and other complications1,2. Australian guidelines suggest performing initial analgesia with paracetamol, nerve block and conservative doses of opioid as needed (PRN)3. However, despite optimal use of paracetamol and nerve blocks, some patients may still ultimately require large doses of opioid for adequate analgesia. Alternatives including opioid sparing strategies would be important to consider in this situation.
Aims
To determine the pre-operative analgesia requirements of patients with surgically managed #NOF in order to identify the frequency of patients requiring higher doses of opioid that might benefit from early consideration of opioid sparing strategies.
Methods
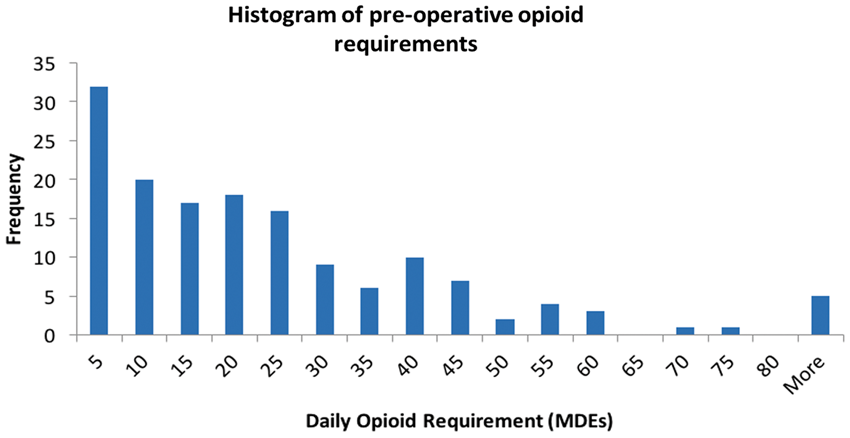
A sample of 151 consecutive patients with surgically managed #NOF was obtained. All analgesia (including nerve blocks) administered between arrival in the emergency department and the time of surgery was noted. Selected pain scores were also obtained from triage documents and observation charts. The pre-operative daily oral morphine dose equivalents (MDEs) were calculated using accepted conversion ratios4 (Table 1) and time to surgery.
Results
The distribution of MDEs (Figure 1) had a large variance (s.d. = 22.5mg). 40 patients (26.5%) required MDEs of >30mg (equivalent to 5mg Endone 6-hourly) and 18 patients (11.9%) required MDEs >45mg. 133 (88.1%) patients received a nerve block. Only 4 patients did not receive a nerve block if they had pain at triage. Only 3 patients did not receive regular paracetamol if the daily MDEs were >30mg. NSAIDs and Tramadol were not regularly used. Tapentadol was used in both sustained and immediate release forms. All other oral opioid used was immediate release.
Conclusions
Even with optimal use of paracetamol and nerve block, doses more than 5mg Endone 6-hourly (or equivalent) are common in this population. Given that elderly patients are more sensitive to opioids, careful consideration of the clinical situation is required when patients exceed their initial, conservative PRN opioid dose ceiling. If further opioids are indicated, sublingual buprenorphine and immediate release tapentadol are reported to have more favourable side-effect profiles5,6. More frequent dosing of shorter acting opioids may be another solution. However, early implementation of opioid sparing strategies such as continuous nerve blocks, and ketamine may be superior. Further research is required to determine this.
Conversion Ratios Used to Calculate MDEs.

Histogram of pre-operative opioid requirements in daily MDEs
References
44
Post-Operative Multimodal Analgesia is Associated with Reduced Opioid Prescriptions After Anterior Cruciate Ligament Reconstruction Surgery
1Tripler Army Medical Center, Honolulu, HI, USA
2Uniformed Services University, Bethesda, MD, USA
Introduction
Anterior cruciate ligament reconstruction (ALCR) is associated with severe post-operative pain and subsequent opioid use. To reduce risk of prolonged opioid use after ACLR, evidence provides strong rationale for optimizing the postoperative analgesia pathway. The present study compared a standard post-operative analgesia pathway to an enhanced pathway in which gabapentin and celecoxib were added to a combined short-acting opioid with acetaminophen.
Aims
The study aim was to determine whether the enhanced pathway was associated with reduced opioid prescription doses and refills in the first 90 days following same-day ACLR surgery.
Methods
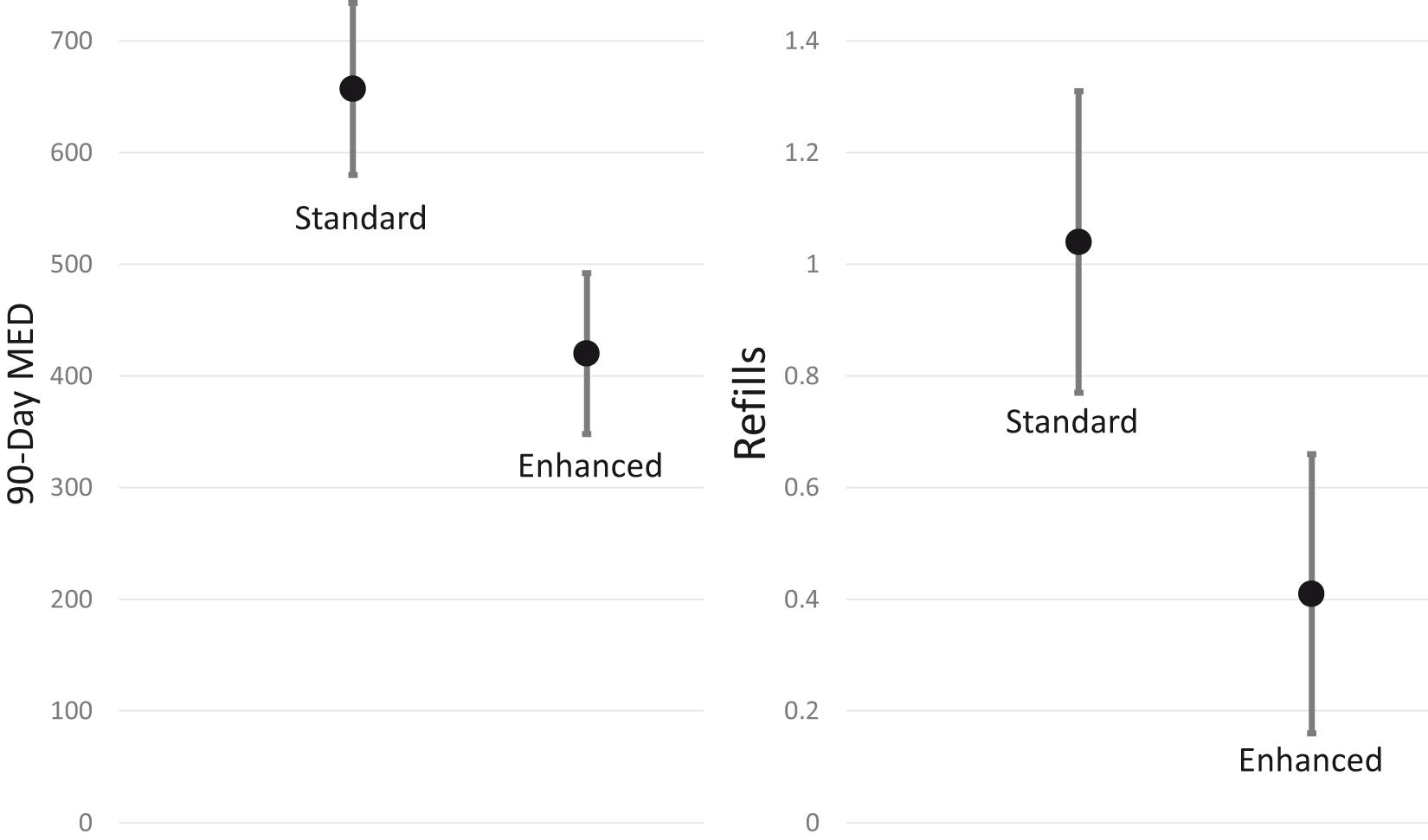
Retrospective data of all primary ALCR cases in a facility (N=108) were divided into a Standard (n = 55) and Enhanced (n = 48) analgesic groups. Bivariate tests assessed group differences in demographic and clinical factors. Generalized linear models (GLMs) examined the effect of group on post-operative morphine-equivalence dose (MED) prescribing as well as number of post-operative opioid refills through 90 days post-operatively, while controlling for relevant covariates. Significance level was adjusted for two outcomes at p < 0.025.
Results
The Enhanced group (94%) had a higher percentage of military service members than the Standard group (71%, p < 0.01). Surgical variables were similar except for increased surgical time in the Enhanced group (p < 0.05). GLMs controlled for military status and surgical time. 90-day post-operative MED prescribed [420 MED (95%CI 348, 492) VS. 657 MED (95%CI 580, 734), p < 0.001] and number of post-operative opioid refills [0.41 (95%CI 0.16, 0.66) VS. 1.04 (95%CI 0.78, 1.31) p < 0.001] were significantly lower in the Enhanced vs. Standard group respectively.
Conclusions
Increased utilization of post-operative gabapentin and celecoxib in addition to a short-acting opioid with acetaminophen was significantly associated with reduced total post-operative opioid prescribing and opioid refills in the first 90 days after same-day ACLR surgery.
Post-Operative Analgesia Group Differences Across Patient Characteristics

Note: Continuous variables were not normally distributed, and group differences were assessed with Mann-Whitney U tests. Categorical variable differences were assessed with Fisher exact tests. SMD=Standardized Mean Difference.
90-Day Opioid Prescribing MED and Refills
47
Anaesthetic and peripartum care and outcomes in super obese women
1The Royal Brisbane and Women’s Hospital, Queensland
2The University of Queensland
Introduction
Obesity is a global epidemic. Published population data from Australia and New Zealand demonstrated that women with a pre-pregnancy body mass index (BMI) greater than 50 kg/m2 or weight > 140 kg have poor maternal and foetal outcomes1. Obesity has been shown to contribute to anaesthesia-related maternal deaths in the United Kingdom2.
Aims
This retrospective audit aimed to assess maternal and neonatal outcomes and anaesthesia management of pregnant women with severe obesity at the Royal Brisbane and Women’s Hospital (RBWH). We compared these with published data obtained for Australia and New Zealand1.
Methods
Ethics exemption was obtained. Women were included if they delivered between January 2013 and December 2017 or had a booking weight > 140kg or BMI greater than 50 kg/m2. Data regarding maternal and fetal outcomes and anaesthetic management was collected by chart review.
Results
We identified 127 women with a median (IQR, range) booking weight of 144 (140-156, 66-212) kg and BMI of 51.9 (49.1-55.6, 42.2-73.9) kg/m2. Table 1 summarises the maternal outcomes, anaesthesia techniques and neonatal outcomes. Five (11.8%) women received pre-natal thromboprophylaxis, while 98 (77%) women received post-natal thromboprophylaxis. Post-delivery, 48 (38%) women required supplemental oxygen for a mean time of 1.5 days, 84 (66%) women used epidural analgesia, while 4 (3.1%) women used intravenous patient-controlled analgesia. Twelve women (9.4%) had diagnosed obstructive sleep apnoea. Fifteen women (12%) did not have an antenatal anaesthesia management plan,
Conclusions
Women with severe maternal obesity have higher rates of maternal and neonatal adverse outcomes. Our data shows a high rate of caesarean section and use of general anaesthesia compared with the general population but similar to population-based data of obese women from Australia and New Zealand [3]. The rate of neonatal intensive care admission was high and could be related to the very high rate of gestational diabetes in this group.
Use of labour epidural analgesia by very obese women was similar to our overall departmental rate of 34%. Regional anaesthesia was the preferred initial anaesthesia technique and the conversion rate to general anaesthesia was 11%. Provision of antenatal anesthesia planning and postnatal thromboprophylaxis can be improved.
Maternal, neonatal and anaesthesia outcomes for 127 severely obese women delivering at the Royal Brisbane and Women’s Hospital, compared with results from Sullivan et al. [2]

BMI: Body mass index; CSE: combined spinal epidural; OT: operating theatre; CS: Caesarean section; BSL: Blood sugar level; NICU: Neonatal intensive care unit; SCN: Special care nursery; ICU: Intensive care unit; HDU: High dependency unit; RBWH: Royal Brisbane & Women’s Hospital; *Labour epidural percentage was calculated using the denominator of all vaginal deliveries and emergency caesarean sections, n=90.
References
48
Obesity hypoventilation syndrome: A hidden diagnosis?
1Senior Staff Specialist, Wollongong Hospital, and Hon Clin Assoc Prof, University of Wollongong, Graduate Medicine
2Critical Care SRMO, Wollongong Hospital, NSW
Introduction
The prevalence of Obesity Hypoventilation Syndrome (OHS) is estimated to be around 0.15%–0.3% in the general adult population and 10–20% in the severely obese. (Chau). Patients with OHS often have other co-morbidities such as left ventricular hypertrophy, obstructive sleep apnoea (OSA), and pulmonary hypertension and have significant increased risks for perioperative morbidity and mortality (Kaw, Chau). OHS patients are 3–10 times more likely to experience complications such as postoperative respiratory and cardiac failure, prolonged intubation, and transfer to ICU when compared to patients with OSA alone (Kaw). Anecdotally, however, when these patients present to anaesthetists, the existing diagnosis of OHS is often not made clear and therefore not acknowledged in anaesthesia planning.
Aims
The study design was a retrospective record review of patients with known, previously diagnosed OHS who had surgical procedures at Wollongong Hospital from 2006–2017. Data from Concord Hospital in Sydney may also be available by the time of presentation. Patients were identified by two methods: hospital coders supplied a list of all patients coded with OHS and anaesthesia / surgery, and the respiratory department provided a list of known OHS patients under their care at Wollongong Hospital. Electronic and paper anaesthesia records were reviewed and qualitative data extracted focusing on initial assessment (airway, co-morbidities and pre-operative investigations), intraoperative management (airway type, ventilation settings, monitoring, analgesia, paralysing agents and extubation plan) and post-operative course (disposition, clinical issues and ongoing management). The proportion of patients with OHS in whom this information was given to the anaesthetist was recorded.
Results
A total of 25 patients were identified: 3 with a coded diagnosis of OHS and 22 patients with a diagnosis from the respiratory department. 44% of these patients had at least 1 previous anaesthetic record, with most patients having multiple anaesthetic records. None of these patients, with known OHS, had this diagnosis documented as part of their anaesthesia assessment. We are currently analysing the rest of the results and will have these available to present before October.
Conclusion
To follow.
References
49
A Novel Method of Recycling in Wollongong Operating Theatres
Wollongong Hospital, NSW
Wollongong Hospital, and Hon Clin Assoc. Prof, University of Wollongong, Graduate Medicine
Introduction
The health of the environment is a public health issue 1. The Australian and New Zealand College of Anaesthesia (ANZCA) has recognised this and has provided a statement guideline on environmental sustainability in anaesthesia and pain medicine practice, thus helping to drive a more environmentally sustainable practise1. It is well known the contribution of anaesthetic gases to CO2 emissions with annual worldwide use having the potential effect as one million American passenger cars on global warming2. Recycling can reduce the carbon foot print and the amount sent to landfill each year1. Anaesthetic waste contributes 25% to overall waste produced in theatre with a proportion of 60% recyclable3. As anaesthetists have been shown to be willing to improve recycling in theatres and reducing environmental impact4. Good waste management and recycling practises should be introduced into theatres to reduce our carbon footprint and also reduce financial costs associated with waste management.
Method
A descriptive review of current recycling practices in Wollongong operating theatres and aimed to outline the waste separation, flow and management through theatres into appropriate collection bins. An audit was carried out to calculate the volume of recycled glass within collected over a one-week period.
Results
The review showed an efficient multidisciplinary approach to waste management in theatres. With two collection points are used in theatres via the anaesthetic area and scout nurse area. With sorting/separation of waste implemented at opening or use of recyclable items and then removed at the end of every case with the general waste and disposed in appropriate collection bins. This included co-mingle (plastic/glass/metals), cardboard, paper and security (confidential paper recycled after shredding). Over the week audit 15.8 Kg of glass was collected for recycling which costs $0.33/Kg compared to sharps/clinical waste disposal $0.95Kg saving $9.80/week.
Conclusion
The recycling process has used a multidisciplinary approach which has improved waste management within Wollongong Hospital. Leading current calculated savings of $9.80/week of recycled glasses but the secondary effects of removing more waste from landfill and recycling objects which has a reduced carbon emission compared to production from raw material. There is ongoing auditing to calculate the further saving of cardboard, plastic, and paper and security waste.
References
50
A Simple Method For Reversing Heparin After Radio-Frequency Ablation
The University of Queensland; Visiting Senior Specialist, Royal Brisbane and Women’s Hospital
Introduction
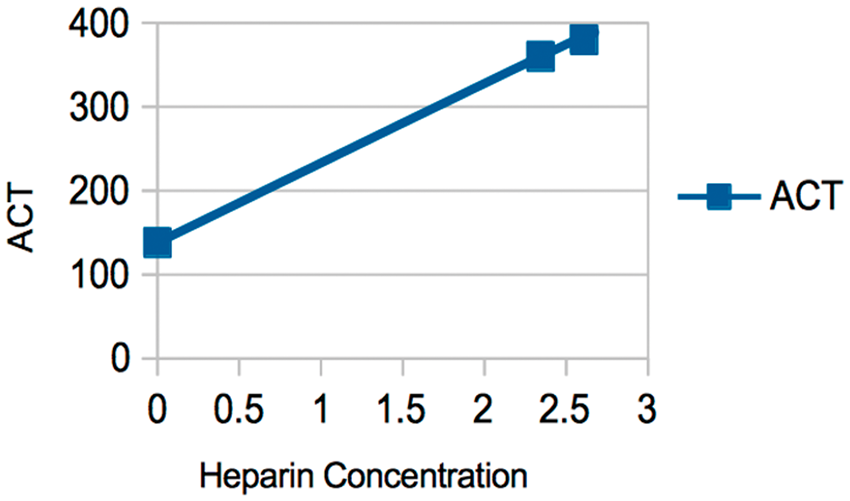
Catheter Ablation for Atrial Fibrillation (CA-AF) has become standard of care for many patients. These procedures require heparinisation to an ACT of between 300 and 400 in order to ensure a very low risk of complications. The variable response to heparin is well documented and can make the calculation of the correct dose of Protamine for reversal problematic, especially if oral anticoagulants are continued.
Aim
The aim of this study was to find a simple method for determining the correct dose of Protamine to give for reversal of heparin to a level approximating their pre-heparin ACT measurement.
Methods
Data was collected prospectively from patients undergoing CA-AF and used to determine estimated blood volume and the amount of protamine to be given.
The pre-heparin and post-heparin ACTs were measured and the slope of the heparin dose-response curve was calculated according to the following formula:Slop=(ACTAH−ACTBH)/([H]AH−[H]BH)where ACTAH is the ACT after the initial heparin dose, ACTBH is the initial ACT before heparin is given, [H]AH is the heparin concentration ten minutes after the initial heparin dose was given, and [H]BH is the heparin concentration before heparin is given (zero).
[H]AH can be calculated from the dose of heparin given and the estimated blood volume using Nadler’s formula1.
Rearranging this gives: [H]BP = (ACTBP−ACTBH)/Slope
where ACTBP is the ACT before protamine is given. Knowing the estimated heparin concentration enables the amount of active heparin producing that ACT to be calculated. A dose of protamine was given using 1 mg of protamine for every 1 mg (100 IU’s) of heparin.
Results
There was no significant difference between the values for pre-heparin ACT and post-protamine ACT. The difference of the means was -6.58, SEM of 1.14, SD of 23.18t value of −5.79 with 416 degrees of freedom (P < 0.001)
Conclusion
A simple method for guiding protamine reversal of heparin used in CA-AF has been developed and shown to be useful in practice. A cross-platform application has been written to facilitate this and is available on Windows, OSX and iPhone.
References
56
Intraoperative systolic blood pressure in traumatic brain injured patients?
1Anaesthetic Registrar, Royal Brisbane and Women’s Hospital, Queensland
2Anaesthetic Provisional Fellow, Royal Brisbane and Women’s Hospital
3Staff Specialist Anaesthetist, Royal Brisbane and Women’s Hospital
Introduction
The World Health Organization predicts that traumatic brain injury (TBI) will be one of the leading causes of mortality and disability worldwide by the year 2020.i There are two injuries in TBI, the primary insult which occurs at time of trauma, and the secondary injury which involves a cascade of mediators resulting in increased intracranial pressure and decreased cerebral perfusion. Intraoperative interventions to improve cerebral perfusion are intended to decrease secondary brain injury.ii Literature now supports a higher level of SBP that may vary by age.iii Perioperative management should be a continuation of the resuscitation process already instituted.ii Different systolic blood pressure targets for different age groups are advised in the most recent TBI Guidelines for the Management of Severe Traumatic Brain Injury (4th edition).
Aims
The aim is to examine the intraoperative systolic blood pressures (SBP) in traumatic brain injured patients and examine adherence to updated guidelines from the Brain Trauma Foundation in 2016.
Methods
Ethics exemption was granted by the Royal Brisbane and Women’s Hospital (RBWH) Human Research Ethics Committee. A retrospective search of emergency neurosurgical procedures for patients with TBI was completed for 2017, (59 patients). Demographics collected were age, sex, GCS, length of procedure (minutes) and length of time the SBP was at or above guideline target (% of procedure duration) SBP. Data was entered into SBP targets for the three age groups: SBP>110 mmHg for 15-49years and >70years; and a SBP>100 mmHg for ages 50-69years.
Results
The most common age group to have a TBI requiring neurosurgical procedure was >70years (47.5%), 50-69 years (27.1%) and 15–49 (25.4%). Of the population who had neurosurgical procedures, 72% were men. The 15-49 year age bracket had the highest adherence to the SBP guidelines (53% had their SBP maintained at >110 mmHg for 90–100% of the operation).
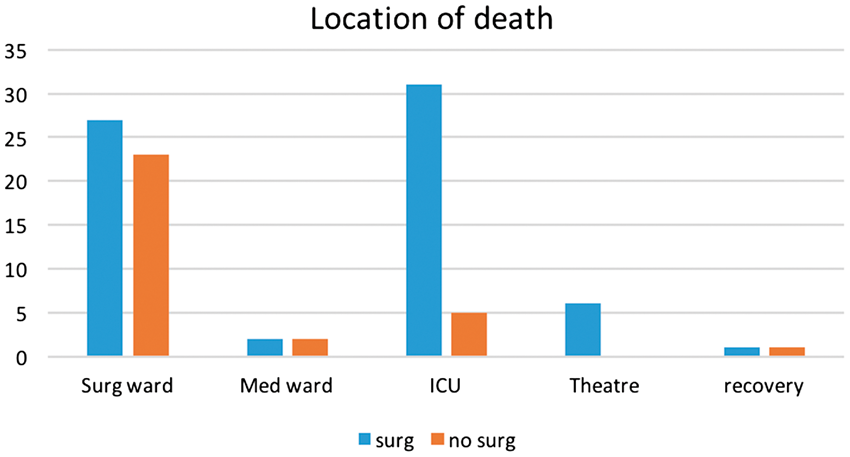
Conclusions
This is a retrospective audit of intraoperative SBP management in patients with TBI undergoing neurosurgical procedures at the RBWH in 2017. It suggests that adherence to specific age group SBP targets, as per the guidelines, can be improved. Departmental education regarding the new guidelines and age group specific targets may improve adherence rates.
References
57
An Audit of Postoperative Nausea and Vomiting Prophylaxis in Patients Undergoing Surgery at a South-East Queensland Hospital
Mater Hospital, Queensland
Introduction
Postoperative nausea and vomiting (PONV) is a common adverse effect of general anaesthesia which can lead to patient dissatisfaction, prolonged post-anaesthesia care unit (PACU) stay, unanticipated delayed discharge and overall health care costs.1 The incidence of PONV is approximately 30% and can be as high as 80% in high risk patients. The Australian and New Zealand Collage of Anaesthetists (ANZCA) endorses the Society of Ambulatory Anaesthesiology (SAA) guidelines for the management of PONV.
Aims
This retrospective cohort analysis evaluates the compliance of patient risk stratification and the administration of PONV prophylactic agents against the current recommended SAA guidelines at Mater Hospital. In addition to overall compliance, we aim to collect data on the incidence of PONV in the Post-Anaesthesia Care Unit (PACU).
Methods
All patients who underwent elective surgery with general anaesthesia over a one-week period in early February were identified by a historical review of Operating Room Management Information System (ORMIS) data. Once patients were identified, a review of patient records via Mater Hospital’s electronic database Verdi allowed the review of clinical records, anaesthetic records and drug charts to obtain the data required. In particular, we focused on PONV risk stratification, antiemetic interventions used, and the incidence of PONV in PACU.
Results
Data showed that although all patients received a pre-surgical anaesthetic evaluation, this only included specific information on PONV if it was a pertinent feature of the patient’s anaesthetic history. Factors significant to a patient’s individual risk of PONV, either protective or predictive, were all evaluated throughout the screen but are not grouped to provide ease of determination of a patient’s specific risk.
The use of single agent intra-operative anti-emetic was frequent as opposed to double or triple agent therapy. There was no correlation overall between number of risk factors identified and number of anti-emetic agents utilised.
Conclusions
While post-operative nausea and vomiting remains well treated and prevented there is consistently room for improvement. Patients with multiple risk factors for PONV are often given a single anti-emetic agent with poor outcomes. An addition of a PONV category to a pre-anaesthetic evaluation (with a simple protective vs predictive factor list) would stratify risks and bring to the forefront of the anaesthetists mind the requirement to increase the number and potency of available anti-emetic drugs.
58
PERIOPERATIVE END-OF-LIFE CARE AND RISK ASSESSMENT. A MULTI CENTRE SURGICAL MORTALITY AUDIT
1Eastern Health VMO Anaesthetist, Monash University
2Austin Health Intensivist, Monash University
3Eastern Health HMO
BACKGROUND
High risk patients rarely have opportunities for End of Life (EOL) discussions prior to theatre. Little is known about the quality of death and comfort care in surgical patients dying in Australian Hospitals. New legislation for advance care planning means that end of life and NFR discussions are an essential part of routine anaesthesia practice. We performed a retrospective audit of surgical mortality to obtain better understanding of the nature and type of pre-operative functional assessment and EOL care in perioperative patients.
CONCLUSIONS

59
Does triggering an Autonomic Sensory Meridian Response reduce pre-operative anxiety?
1The University of Sydney, Sydney Adventist Hospital Clinical School, NSW
2The University of Sydney, Sydney Medical School, NSW
3Westmead Hospital, Sydney, NSW, The University of Sydney, School of Public Health, NSW
Introduction
Pre-operative anxiety is common and associated with perioperative hypertension, arrhythmias and nausea and vomiting. Various techniques have been investigated to reduce this anxiety such as listening to music, and premedication. The Autonomic Sensory Meridian Response (ASMR) is a relatively new and abstract relaxation technique that has been reported to reduce anxiety and depression. It has not been investigated in the peri-operative setting.
Aim
To assess the effect of an audio-visual stimulus designed to trigger an ASMR on pre-operative anxiety.
Methods
This randomised, prospective, double blind, placebo-controlled trial enlisted 50 elective surgical participants. Ethics approval and informed consent preceded randomization. The study intervention was a 6-minute video presenting standard pre-operative information in an ASMR format; the placebo video presented the same information in a conversational tone. Subjects completed the study using an iPad which presented the preoperative questionnaires, the allocated video and the post intervention questionnaires in a seamless platform using Research Electronic Data Capture (REDCap) tool. Demographic data included age, sex, ethnicity, date of birth and previous ASMR experience were recorded. The primary outcome was a change in anxiety after the intervention, quantified by heart rate, arterial blood pressure respiratory rate, and 3 validated anxiety grading tools; Visual Analogue Anxiety Scale (VAAS), the State-Trait Anxiety Inventory (STAI), and the Amsterdam Preoperative Anxiety and Information Scale (APAIS).
The secondary outcome was a change in anxiety after the effect of the intervention in patients with a high trait anxiety.
Results
The demographic characteristics were similar in both groups. Pre-intervention, there was no difference in the physiological and behavioural variables between groups. Systolic arterial pressure was lower post intervention in the ASMR group, a finding which was maintained after multivariate analysis. (Table 1).
There was a reduction in the VAAS and APAIS scores in the control group following the intervention as well as a fall in the APAIS score in the ASMR group. The STAI-S did not change in either group.
There was no correlation between higher pre-intervention trait anxiety and the effect size.
Conclusions
We found a small fall in systolic arterial pressure and APAIS after the ASMR triggering video. VAAS and APAIS fell in the control group. We did not confirm an anxiety reducing effect of our ASMR triggering video.
Change in physiological and behavioural variables after exposure to a pre-operative video in either an Autonomic Sensory Meridian Response triggering or conversational format. [mean (95% confidence interval)]

61
An Audit of Perioperative Surgical Antibiotic Prophylaxis Administration in Patients Undergoing General Surgery at a Tertiary Hospital
Department of Anaesthesia, Royal Brisbane and Women’s Hospital, Queensland
Introduction
Surgical antibiotic prophylaxis has been demonstrated to reduce the risk of perioperative surgical site infections. The current edition of Therapeutic Guidelines suggests that surgical antibiotic prophylaxis is administered inappropriately in a large proportion of surgical procedures (between 30 to 90%). Appropriate antibiotic prophylaxis includes the choice of drug, dose of drug and timing of drug in order to optimise both (1) the tissue antibiotic concentrations, and (2) the spectrum of antimicrobial coverage at target surgical tissues.
Aims
This retrospective audit evaluates the administration of surgical antibiotic prophylaxis, within the Department of Surgery and Perioperative Services at the Royal Brisbane and Women’s Hospital. We compared hospital practice to the Australian Therapeutic Guidelines to establish the rate of complying with the current gold standard. In addition we assessed (1) the reasons for antibiotic prophylaxis not complying with guidelines, (2) factors that affect complying with surgical antibiotic prophylaxis guidelines, and (3) incidence of post-operative infective complications.
Methods
All patients having general surgery from 1st February 2017 to 14th February 2017 were identified from the operating theatre electronic database. Patient records were reviewed to obtain all relevant information, including the specific details of the antibiotic prophylaxis administered and post-operative infectious complications.
Results
A total of 115 general surgery cases were identified in this two week audit period. Of the 115 cases, 57 (49.6%) adhered to current guidelines. There were an additional 20 cases that did not follow the current guidelines, but antimicrobial cover was acceptable for the surgical cases performed. These 20 cases included (1) patients who were on an appropriate antibiotic pre-operatively, and (2) cases in which there was an appropriate substitution of an alternative antibiotic. Overall there were 77 cases that had an appropriate antimicrobial coverage during the surgical case (67.0%).
There were 10 reasons identified for not complying with current guidelines and providing appropriate antimicrobial prophylaxis (outlined in Table 1).
Post-operative infective complications occurred in 10 surgical cases (8.7%).
Conclusions
There was poor compliance with surgical antibiotic prophylaxis guidelines in our audit population. This resulted in 37 cases (32.2%) not having appropriate antimicrobial coverage during surgery. The main reason for poor compliance was late timing of antibiotic administration (11.3%).
Of the 10 cases of post-operative infections, 6 cases of post-operative infection had an appropriate antimicrobial coverage during surgery (60.0%), and 6 cases of post-operative infection had a pre-existing pre-operative infection (60.0%). Of the 6 cases of post-operative infections that also had a pre-existing pre-operative infection, only 2 cases received pre-operative antibiotics.
– Compliance with surgical antibiotic prophylaxis guidelines and appropriate antimicrobial prophylaxis in the audited general surgical cases.

62
Endotracheal intubation versus supraglottic airway device insertion in cardiac arrest: A systematic review and meta-analysis
1School of Medicine, University of Queensland, QLD; Sunshine Coast University Hospital QLD
2School of Medicine, University of Notre Dame, NSW, Australia; Wagga Wagga Base Hospital, NSW
3School of Medicine, University of Queensland, QLD
4School of Medicine, University of New South Wales, NSW; Royal Prince Alfred Hospital, NSW
Introduction
Failure to ventilate via a bag valve mask is not an uncommon situation during out of hospital cardiac arrest (OHCA). Available advanced airway management strategies include endotracheal intubation (ETI) and supraglottic airway (SGA) device insertion.
Aims
The primary aim of this study was to compare survival to discharge in OHCA in patients managed with ETI versus SGA during the prehospital period. Secondary aims were to compare incidence of ROSC, survival to hospital admission and neurological outcome.
Methods
Five databases were systematically searched to May 2018. Studies comparing the use of ETI versus SGA in the prehospital setting for OHCA were included. All studies were assessed on methodological quality using the Cochrane Collaboration’s tool for risk of bias tool. A quantitative analysis was performed using RevMan 5.3 software (The Nordic Cochrane Centre, Copenhagen, Denmark), using the odds ratio (OR) with 95% confidence interval (CI) for dichotomous outcomes, and the weighted mean difference (WMD) with 95% CI for continuous outcomes. The Mantel-Haenszel (M-H) random effects model was used. Heterogeneity was assess using the I2 statistic, with an I2>50% indicating significant heterogeneity. P value of < 0.05 provided evidence of significant OR and WMD. Sensitivity analyses were performed for care provider, manual or automated chest compressions or cause of arrest.
Results
Twenty-six studies with 443,164 patients were found in our systematic search. Overall, there was a significant increase in the rate of ROSC with ETT compared to SGA (OR= 1.52; 95%CI= 1.35 to 1.71; I2=88%; p < 0.0001). The significant benefit of ETT compared to SGA persisted, with significant increased in survival to hospital admission (OR= 1.45; 95%CI= 1.17 to 1.78; I2=90%; p=0.0006) and survival to hospital discharge (OR= 1.35; 95%CI= 1.05 to 1.73; I2=97%; p=0.02). Despite the increase in overall survival, there was no significant difference in the rate of neurologically intact discharge (OR= 1.22; 95%CI= 0.97 to 1.54; I2=92%; p=0.10). There were no changes in significance on sensitivity analysis for care provider, manual or automated chest compressions or cause of arrest.
Conclusions
In the largest meta-analysis ever performed, we showed significant increase in the likelihood of achieving ROSC, survival to admission and survival to discharge when patients received an ETT as opposed to a SGA in cardiac arrest. However, there was no increase in survival neurologically intact. This is in keeping with the fact that airway management is only one aspect of cardiopulmonary resuscitation.
63
e safety of buprenorphine compared to morphine in acute pain: A systematic review and meta-analysis
1School of Medicine, University of Queensland, QLD; Sunshine Coast University Hospital QLD
2School of Medicine, University of Notre Dame, NSW, Australia; Wagga Wagga Base Hospital, NSW
3School of Medicine, University of Queensland, QLD
4Sunshine Coast University Hospital QLD
5School of Medicine, University of New South Wales, NSW; Royal Prince Alfred Hospital, NSW
Introduction
Buprenorphine is a potent analgesic agent with no ceiling effect in the setting of acute pain. Current guidelines indicate that buprenorphine may be safer than alternative opioids with a ceiling effect on respiratory depression and sedation. However, the data referenced in most guidelines are derived from lab-based studies in healthy young research participants.
Aims
The primary aim is to determine the safety profile of buprenorphine in comparison to morphine in the hospital setting. The secondary outcome is to assess the relative analgesic efficacy of buprenorphine compared to morphine.
Methods
Five databases were systematically searched until May 2018. Only studies investigating buprenorphine compared to morphine for acute pain in the hospital setting were eligible for inclusion. Studies including patients on chronic buprenorphine therapy were excluded. All studies were assessed on methodological quality using the Cochrane Collaboration’s tool for risk of bias tool. A quantitative analysis was performed using RevMan 5.3 software (The Nordic Cochrane Centre, Copenhagen, Denmark), using the odds ratio (OR) with 95% confidence interval (CI) for dichotomous outcomes, and the weighted mean difference (WMD) with 95% CI for continuous outcomes. The Mantel-Haenszel (M-H) random effects model was used. Heterogeneity was assess using the I2 statistic, with an I2>50% indicating significant heterogeneity. P value of < 0.05 provided evidence of significant OR and WMD. A p value of < 0.10 was used to demonstrate heterogeneity of intervention effects.
Results
In total, twenty-eight randomised controlled trials that included 2,210 patients were eligible for inclusion in this meta-analysis. There was no difference in the incidence of adverse events with the exception of less pruritus (OR= 0.31; 95%CI= 0.12 to 0.84; I2= 6%; p=0.02) compared to morphine. Incidence of respiratory depression (OR= 2.07; 95%CI= 0.78 to 5.51; I2= 30%; p=0.14) and sedation (OR= 1.44; 95%CI= 0.76 to 2.74; I2= 23%; p=0.26) were not significantly different to morphine. Buprenorphine provided equivalent analgesia to morphine, with no difference in visual analogue scores (WMD= -0.29; 95%CI= -0.62 to 0.03; I2=99%; p=0.07)
Conclusions
The present study supports the current guidelines in regard to buprenorphines analgesic efficacy. Our findings also recommend that buprenorphine be used with caution, equal to any other opioid.