
Abstract
Paediatric airway management is a challenging area of anaesthesia practice to learn. Techniques and skills required need modification from adult practice and gaining experience through exposure takes considerable time. Preparation to manage airway emergencies can be particularly difficult as these events are rare in paediatric practice. This study aimed to examine what educational approaches health professionals of varying backgrounds find useful when learning or teaching paediatric airway management. This qualitative study involved the conduct of five interdisciplinary focus groups; each group consisted of four to six health professionals from nursing, anaesthetic, simulation and critical care backgrounds. After transcription, focus group content was analysed using a qualitative method to identify common themes expressed within the interviews. Five themes were most prominent. These included the high value of hands-on learning, the challenges created by variability in exposure, the importance of developing basic airway skills, the potential for simulation to cover rare situations, and the problems of current airway models. These themes were evident in comments from both experienced and novice practitioners, clinicians with different subspecialty backgrounds and both medical and nursing staff. Learners and educators have similar priorities in airway education. This includes a strong recognition of the importance of spending time mastering basic airway techniques, a role for simulation in building non-technical skills and noted deficiencies in current airway models.
Airway management is a complex area of paediatric clinical practice. It requires development of skills in patient assessment alongside technical skill competency. The paediatric practitioner will care for patients ranging from the premature neonate to the robust teenager with significant changes in patient anatomy and physiology. Bag–mask ventilation, supraglottic airway insertion and endotracheal intubation are examples of practical skills requiring an adjustment in approach compared to adult practice. These differences may be further complicated when managing the difficult paediatric airway where there is uncertainty regarding the best techniques in younger patients.1–6
A comprehensive education approach is needed to develop practitioners proficient in this range of specific paediatric airway skills. Literature relating to education in paediatric airway management often focuses exclusively on the role of a specific technique such as simulation, success rates with a particular device, or the use of a piece of equipment to achieve a specific goal. 7 Absent from such investigations is a broader reflection on what key areas, among the broad range of skills in airway management, most need focus in an airway education programme. There are also multiple stakeholders who may identify different priority areas for learning, or different educational approaches that provide the most value. Novice practitioners in critical care, from either a medical or nursing background, may provide additional unique insights into learner needs. More experienced practitioners, who often have a role in education of trainees, are able to reflect on their own experiences, recall their observations of novices and identify educational tools they find useful.
This focus group–based qualitative study was designed to address current gaps in the literature by reporting on the key questions of: (1) What areas of paediatric airway management do practitioners find most challenging to learn?; and (2) What techniques and approaches are perceived as most effective in helping learners develop their competency? 8
Methods
Ethical considerations
Ethics review and approval was conducted by the Sydney Children’s Hospital Network Human Research Ethics Committee (LNR/15/SCHN/491). All participants were provided with information relating to the study prior to sessions, with further opportunity to ask questions. Signed consent was obtained from all participants after reaffirming that focus group interviews would be recorded via audio recording and contemporaneous note-taking.
Participants
Participants were sourced by advertisement and word of mouth within departments at the participating tertiary paediatric facilities. Participants were drawn from specialties where paediatric airway management is a routine part of the work profile. This included paediatric anaesthesia, paediatric intensive care medicine, paediatric emergency medicine and paediatric airway surgery. One participant who was an experienced anaesthetic and post-anaesthesia care unit (PACU) nurse is also employed in simulation, while some of the medical practitioners also had experience in simulation. Participants could be from a medical or nursing background. They were further characterised as novices if they had less than two years of experience with paediatric airway management or experienced if they had a longer clinical practice. All experienced practitioners are involved in education of trainees as part of their senior role.
Data collection
A focus group methodology was chosen for this qualitative study as an efficient way to explore a range of opinions and ideas on the subject of interest (Table 1). 9 Focus group sessions were designed to include four to six participants to optimise the chance of achieving adequate data saturation. Groups were selected to have a mix of clinical specialties and a range of physicians and nursing practitioners to encourage discussion of varying perspectives and experiences. Where trainees were involved in a focus group, they were kept separate from direct supervisors to remove the potential that junior clinicians might feel inhibited in discussing areas of practice they found challenging, or in reflecting on their experience of different styles of teaching. At each centre (The Children’s Hospital at Westmead, Sydney (CHW) and Royal Children’s Hospital, Melbourne (RCH)) three focus group interviews were conducted. In one session at RCH, an attendee arrived late to the session, and they were interviewed further at the end of the planned session to include their reflections.
Guide questions for focus group sessions.

Guide interview questions were created by the investigating authors. Interview questions aimed to cover the key areas of prior experiences of paediatric airway management and education in this area, key features of successful versus unsuccessful education experiences, and particularly challenging clinical areas to master. Specific attention was paid to the utility of airway models and simulation methodologies as part of airway education on the basis of the experience of the clinician investigators.
Conduct of the interviews was led by the second author (MM) who has prior training in qualitative study methodology. At CHW, author 1 (AW), a specialist paediatric anaesthetist, attended interviews with scope to prompt further discussion of particular items. At RCH, author 3 (SMK), also a specialist paediatric anaesthetist, performed this role. Audio recording was supplemented by contemporaneous note-taking by both attending investigators.
Analysis
There were no pre-defined themes, with categories developed from the content analysis process as described by Malterud.10,11 A process of decontextualisation and recontextualisation was undertaken. Recorded focus groups were transcribed independently by the investigators present at those particular sessions. The entire transcripts were read in context to understand the overall nature of the discussion. Individual investigators then read through the text again identifying preliminary themes with relevant text units manually sorted under headings. For each of these themes further analysis was undertaken to identify any subthemes as part of deeper analysis. At this point authors involved in this stage (AW, MM and SMK) discussed identified themes and subthemes, with further restructuring and reformulation taking place. All themes were reviewed by all co-authors prior to finalising the coding framework. This process resulted in consensus on identified themes. Authors 1 (AW) and 2 (MM) then returned to the initial focus group material to examine the identified themes in their original context, with quotes from the groups chosen for illustration.
Results
Twenty-three individuals participated in focus groups (see Table 2). There were 14 physicians, eight current nursing staff and one simulation practitioner who also had a background as an experienced anaesthetic and PACU nurse. Of the physicians, ten were anaesthetists (seven experienced, three novices), one was an experienced emergency medicine physician, two were novice intensive care physicians and one was an experienced ear, nose and throat (ENT) surgeon. Among nurse participants there were seven currently working in anaesthesia and PACU (five were experienced and two were novices). There was one nurse with a background solely in PACU who was experienced.
Participant backgrounds.
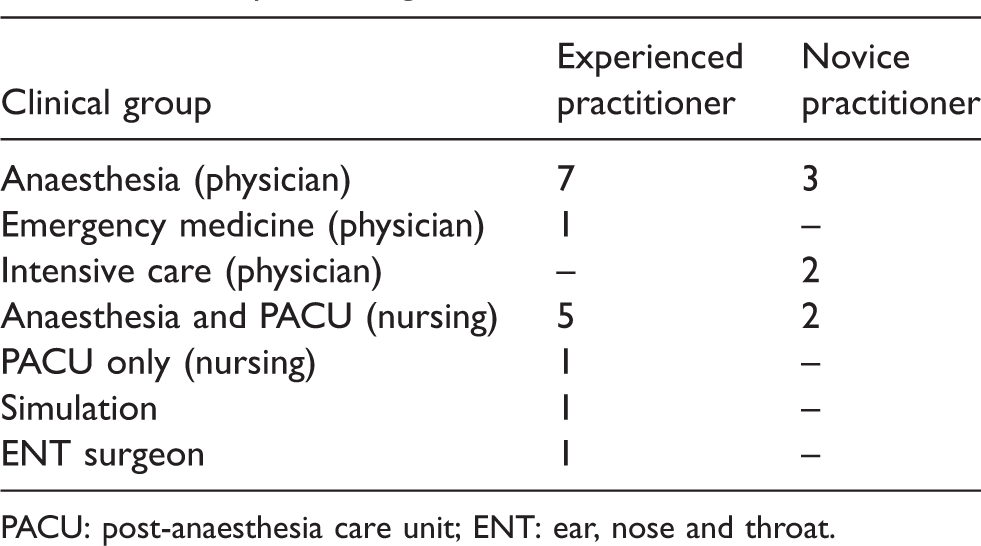
PACU: post-anaesthesia care unit; ENT: ear, nose and throat.
Five key themes emerged. Themes highlighting optimal learning and education practices included: The benefit of guided experiences with scope for learner problem-solving; and that Simulation is valuable for non-technical skills development. Themes highlighting challenges to learning included: Variability for the learner in case exposure and teaching styles; Learning curves apply to basic and advanced technical skills; and that Current airway models are inauthentic.
The benefit of guided experiences with scope for learner problem-solving
Practitioners of all levels highlighted the need to obtain hands-on experience to learn the necessary skills and clinical assessment capabilities. While some participants noted benefits to being ‘thrown into’ managing the airway of a patient, a repeated theme was that opportunities to do so were more effective if learners have guidance through this. Being thrown into a clinical situation without prior preparation was seen as a practice common to medicine but less than ideal. I think some anaesthetists … give us a little a bit more opportunity than others. My first week as a learning anaesthetics nurse he said ‘just put the LMA (laryngeal mask airway) in’ and I was nervous but I did it and it just went in and being thrown in the deep end and not sinking sets the tone for the rest of your career … Because he’s standing right there, he can take over any minute it’s a good thing because they’re not walking out of the room and saying ‘Off you go’ (Group 1, experienced anaesthetics nurse). … all of my most valuable learning experiences are when I’ve been allowed to have what I call a ‘guided struggle’ … it is far more valuable to come up with the solution myself than watching someone else doing it… There is less to be learnt if you feel like a failure and didn’t get the chance to fix it. (Group 1, anaesthetics, novice physician) My most memorable learning experiences are when I figure things out myself so some autonomy is valuable. I try to do this with juniors. (Group 3, anaesthetics, experienced physician)
Simulation is valuable for non-technical skills development
Simulation was felt by all groups to be a valuable educational tool, both as learners and as educators. It was felt to be useful for rehearsing high-risk, low-incidence scenarios with examples offered including difficult airway management, ‘can’t intubate, can’t oxygenate’ (CICO) situations or emergencies in remote areas. Those kind of high-risk, low-frequency scenarios to me those are the sorts of things I see value in running simulation in. (Group 1, experienced anaesthetic nurse and simulation educator) Simulation works really well in getting a group of people working together to manage a scenario … The actual skills side of things maybe not so much, but the teamwork side of things, it’s really helpful. (Group 2, experienced anaesthetist)
Variability for the learner in case exposure and teaching styles
Groups noted that development of airway skills requires time and experience. It is a hands-on process fostered through an apprenticeship model where those training learn with a variety of senior practitioners. As different senior practitioners share varying tips or approaches, synthesising this information is challenging. The patients trainees are exposed to are different from one case to the next with little guarantee of repeating skills from case to case. I do agree with [X] that especially when you’re starting out it’s really difficult assimilating information from a variety of sources and some people are just better teachers than others. There’s no standardised way of teaching things, everybody has their own way … (Group 1, experienced anaesthetic nurse and simulation educator) It’s difficult in our setting because you’ve got a new team almost every day, you’ve got a new patient every hour or two. First of all you have to work out how to teach this particular learner or how this particular learner can learn from you and then on top of that you’ve got to teach them how to manage this particular airway which you may not have a second chance for them to repeat what they do because your next five patients are all different. (Group 1, novice anaesthetist) It can be confusing for beginners having many different techniques demonstrated by different people. (Group 4, anaesthetics, experienced physician)
Learning curves apply to basic and advanced technical skills
In response to the question ‘What is the most challenging part to learn?’, advanced airway skills such as laryngoscopy and intubation were rarely mentioned. More basic skills such as bag–mask ventilation or patient assessment represented the most common responses. This was evident in responses from doctors and nurses, as well as novice and experienced clinicians. Other challenges noted related to development of cognitive skills and decision-making. … the other is the confidence of being able to back off and take control again of the ventilation and not get yourself into a stress cycle … (Group 3, experienced anaesthetist) [In response] What to do if the first plan doesn’t go right or doesn’t go according to plan. Being willing and happy to stop and think about plan B as opposed to struggling with plan A. (Group 3, experienced anaesthetics nurse) Assessing an obstructed airway is quite advanced, like looking at whether a child is making respiratory efforts with their abdomen and whether they are actually moving air … (Group 1, novice anaesthetist) [In response] And there are different gradients of obstruction as well. (Group 1, experienced anaesthetic nurse and simulation educator)
Current airway models are inauthentic
Related to the question on simulation was discussion of current airway manikins. Current paediatric airway manikins that participants had been exposed to were noted to be unrealistic in terms of anatomy and haptic feedback when performing procedures. Issues with manikins were noted when describing simulation as useful for non-technical skill development, but less useful for technical skill acquisition due to flaws in replication of the ‘feel’ of the airway: I think they are useful to understand the anatomy because you are actually looking at a 3D model of whatever but ultimately my experience with manikins is that they are not like the real thing, like intubating manikins is not like intubating real people. (Group 1, anaesthetic novice) … I find the current models are just hopeless pieces of rigid plastic. They don’t give you any feedback that’s consistent with what you find clinically. (Group 5, experienced anaesthetist) I’ve encountered low fidelity and high fidelity models and the low fidelity models traditionally are not meant to be difficult airways or difficult intubations but they unintentionally are and the high fidelity ones are intended to be … but you get used to that one particular model. (Group 2, experienced anaesthetist) … if you are just starting there is plenty to learn from the manikins, but I guess particularly worrying is that sometimes bad habits might be learnt from a manikin and you get good at manipulating an indestructible thing … (Group 4, experienced anaesthetist)
Discussion
These discussions showed striking coherence among both experienced and novice practitioners with different clinical backgrounds. With reference to the original research questions, the most challenging areas identified for learners were basic airway skills, dynamic assessment of the paediatric airway and cognitive decision-making. The most effective educational approaches identified by the focus groups shared the characteristic of supervised autonomy while simulation was perceived as effective in developing non-technical skill.
As a hands-on skill, participants frequently focused on the requirement to gain exposure over time to develop the skills to feel competent in airway management. To create an optimal learning situation, the ideal approach was felt to be initial development of knowledge and rehearsal in a controlled situation prior to exposure to patients. The concept of the ‘guided hands-on experience’ was felt to be most effective, with particular note to the value of being given the opportunity to solve a challenge while knowing support was available.
The traditional apprenticeship model of learning utilising patients for development of primary skills in paediatric airway management is not acceptable in modern practice. 12 A standardised process of knowledge acquisition or reinforcement, rehearsal followed by clinical exposure, may help address the expressed issue of variability in what learners are taught. The heterogeneous nature of cases presented to the learner with varying clinical teams makes hands-on experience difficult to standardise. Initial learning stages taught to an agreed plan would provide some consistency of content and skill learning. Of note, although there has been recent emphasis on the importance of CICO algorithms and the need for training for this scenario, both novice and experienced practitioners stressed the challenge of becoming expert in other areas, particularly knowledge and skills framed as basic.1,13 This accords with concerns expressed by other authors that emphasis on CICO may limit an appropriate focus on the skills required to avoid such situations. 14 Participants noted priority areas of bag–mask ventilation and skills in clinical assessment. These basic areas seem to be rarely discussed in the literature on approaches to airway management education. Nuanced discussion of the ‘best’ basic techniques to pass on to learners is lacking, and the best way to provide this education is not a topic that seems to exercise authors in the area greatly. A previous consensus statement relating to airway management education priorities in emergency medicine neglected all mention of basic airway skills. 15 Accelerating the learning curve in these areas should be a priority of educators, rather than early focus on higher acuity skills, and suggests an importance for holistic, qualitative approaches in evaluating effective clinical education.
Simulation was identified as an expectation of a comprehensive learning programme from participant groups. Its key role was felt to be in rehearsal of rarely confronted but high pressure scenarios and in developing thought processes, plans and teamwork.16,17 This agrees with research showing improvements in operating room communication after team-based simulation as well as improvements in resident confidence in managing neonatal resuscitation.18,19 Although there are reviews suggesting skills development is improved with simulation and that specific paediatric anaesthesia skills programmes are useful, simulation was not felt to be useful for skills development by this cohort.20,21
The perceived issues with skills development may be influenced by limitations of currently available paediatric airway manikins. Current manikins were noted to be inaccurate representations of the paediatric airway, providing unrealistic anatomy and an artificial ‘feel’ during use. This impression from the focus groups accords with previous reports in the literature in terms of anatomical accuracy of paediatric airway models.16,22,23 Some similar issues have been reported in adult airway models. 24 Responses obtained in these focus group sessions suggest this may even extend to encouraging inappropriate techniques when used as a primary learning tool. There is a clear role for more realistic paediatric airway models.
This study is limited by the heterogeneous nature of the respondents. This makes it difficult to assess if there are particular areas that are specific challenges or priorities for specific craft groups. The coherence in responses obtained does, however, suggest that many of the key concerns of learners and educators are in common. This study did not explore the topic of multidisciplinary education in any depth, but rather sought to fill the existing gap related to a lack of holistic understanding of priority needs in paediatric airway management.
Participants in the study volunteered to discuss their experiences relating to paediatric airway education. Self-reporting raises the potential for bias as participants’ responses may be coloured by a desire to influence others’ perceptions of them. Participants may also be more likely to report previous bad experiences which may be more memorable.
While an effort was made to have practitioners at different levels, all participants were in clinical practice in tertiary paediatric facilities. As such the findings may not be applicable to earlier stages in training, and the priorities and experiences of student learners may be different. It is also possible that there may be some transference of skills from prior airway management experience in adult patients, though this did not emerge as a theme in any of the focus groups. Absence of this theme does not exclude the possibility that this sort of prior experience may influence development of learner competency, and further research would be required to specifically explore this possibility.
This cohort also had a larger proportion of experienced practitioners. Apparent agreement in responses from novices compared to experienced practitioners may not have been so evident if more junior practitioners responded to the call for participants. Follow-up studies with a focus specifically on novices would permit a more in-depth exploration of this potential issue. While there were fewer novice practitioners than experienced clinicians, there were no focus groups where the novice practitioners were in the same group as a direct supervisor. Power dynamics are therefore an unlikely source of bias within the discussions.
Conclusion
Practitioners in paediatric airway management from all backgrounds involved in this study highlighted the key challenges of learning skills sometimes considered basic such as bag–mask ventilation and clinical assessment proficiency. The ideal education construct was felt to be knowledge acquisition followed by rehearsal prior to supported hands-on clinical exposure. Simulation was felt to be a valuable part of this, though technical skills acquisition is hampered by inadequate paediatric airway models. A standardised learning programme may help address the issue of variable clinical exposure once practitioners commence work with patients.
Footnotes
Authors’ contributions and authorship
AW: Study design, focus group interviews, data analysis; first draft and manuscript preparation. SMK: Study design, focus group interviews, data analysis, manuscript review. MM: Study design, focus group interviews, data analysis, manuscript review. ML: Study design; review of themes; manuscript review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No external funding was utilised for this study. Travel of investigators to sites for focus groups was sourced from departmental funds.