
Abstract
Patients recovering from critical illness are often suffering from remarkable limitations in their everyday life. The purpose of this study was to find factors associated with poor physical functioning and mental health after critical illness. The study was conducted among patients who met the inclusion criteria of our post–intensive care unit follow-up clinic. The patients were invited to the follow-up clinic three months after hospital discharge. The participants filled out a RAND-36 questionnaire, underwent a clinical examination and were stratified to those with good or poor recovery according to physical functioning and emotional wellbeing. Altogether 332 out of 351 follow-up clinic attendees had data available for analysis. In physical functioning 40% of patients achieved a poor outcome. In mental health the percentage was 8%. The patients with poor physical functioning had a longer hospital stay and were more likely to have received vasopressors. Eleven out of 16 (69%) multitrauma patients had poor physical functioning. Patients with poor physical functioning had more memories of pain, achieved worse results in a six-minute walk test and were less likely to be able to move independently. The patients with poor mental health had higher delirium incidence and fewer memories of relatives’ visits and of nurses. The conclusions of this study were that the memories of pain, multitrauma and longer hospital stay were associated with a poor physical functioning outcome. Delirium and a lack of memories of relatives and nurses were associated with a poor mental health outcome.
Keywords
The ideal outcome in critical care is a patient surviving through the acute, life-threatening event and eventually attaining similar—or nearly similar—medical condition and health-related quality of life to before the critical illness. In real life, a significant portion of intensive care unit (ICU) survivors recovering from a critical illness suffer remarkable limitations in their physical capability, in their psychological and cognitive functions and in their social interactions.1–7 This then imposes a significant burden on the patient’s post-ICU health-related quality of life. 8 Due to the significant subjective and societal burden caused by post-ICU–related health impairments, the early and effective recognition of high-risk patients plays an important role in the organisation of post–critical illness rehabilitation. 9
Older age is a recognised risk factor for impaired physical functioning 10 and worsened neuropsychiatric status, 5 but impairments in these functions affect patients in all age groups. Deficits in physical functioning and mental health play a major role in a decreased ability to return to work after a critical illness in working-age patients.11,12 During the recovery process, physiotherapy-led rehabilitation care has been reported to improve exercise capacity after critical illness. 13 The incidence of some specific neuropsychiatric conditions, such as post-traumatic stress disorder and depression, are also more common in the younger ICU-survivor population.4,14 Early recognition and correctly timed therapeutic interventions play a significant role in the treatment of these mental health issues.15,16
The ICU physician- or ICU nurse-led follow-up clinics have been proposed as a way to follow ICU survivors and facilitate the early recognition and treatment of any ICU-related comorbidities. Quantitative and qualitative evidence as to the degree to which post-ICU follow-up clinics are beneficial, however, is limited or controversial.17–19 Scientific evidence as to the correct patient selection for follow-up clinic referral also remains uncertain.
In this retrospective study, we evaluated the patients from our own post-ICU follow-up clinic and attempted to determine which factors are associated with impaired physical functioning and/or impaired mental health at three months after ICU discharge in a selected cohort group of long-staying patients of working age. Our purpose also was to determine the patient groups that might benefit from the follow-up clinic visits in the future.
Materials and methods
The study was performed at our 26-bed, mixed surgical and medical adult ICU of the Oulu University Hospital, which is a tertiary-level academic teaching hospital in northern Finland. Institutional approval for the study was obtained according to the policy set out by the local Ethics Committee (journal number 64/2016) and the Data Protection Ombudsman. The local Ethics Committee accepts all registry-based studies. All variables used were previously collected for clinical purposes according to our standard practice and no intervention other than the recording, classifying, counting and analysing of data took place.
Patients
The study population consisted of ICU survivors who had been examined in the post-ICU clinic during the years 2004–2012. Post-ICU patients from the Northern Ostrobothnia hospital district (population 400,000) can use the services of our follow-up clinic. Our service does not cover patients referred from the four, non-academic–level central hospitals in our tertiary-care area (population of 740,000). There were no interventions related to this study. The patients were treated according to the judgement of each attending physician. Discharged patients aged between 18 and 65 years who recovered to live at home with an ICU length of stay (LOS) of more than four days were invited to attend our follow-up clinic at three months from hospital discharge. The group of patients excluded included: cardiac surgery patients, patients suffering severe psychiatric disorders, patients with alcohol or substance abuse issues and patients who were unable to properly communicate or cooperate. Patient selection was made by the follow-up clinic nurse after reviewing the patient charts.
We focused on selecting working-age patients with a prolonged ICU stay, as this is the patient group expected to most benefit from rehabilitation information and a debriefing conversation. The timing of the follow-up clinic visit occurred at three months after hospital discharge to ensure that the early detection of post–intensive care–related health issues was possible. Prior to the visit, patients received a health-related quality of life (HRQoL) questionnaire (RAND-36 HRQoL; validated Finnish version) to be returned and discussed during the visit.
Study data and main outcome variable
At the follow-up clinic the clinic’s nurse interviewed the patient using a semi-structured questionnaire. This assessment form was a part of the patient’s medical chart and was stored electronically in our hospital’s patient records. The interview covered memories of the ICU period, and current physical, psychological and social issues that the patient might have experienced. Following the interview, a clinical examination was performed (blood pressure, heart rate, electrocardiography, hand-grip test, six-minute walk test (6MWT) and body weight). The data gathered during the clinic visit was subsequently retrieved for our analyses. Patient demographics, comorbidities, severity of illness scores, organ failure scores, reasons for ICU admissions and data regarding ICU stay were retrieved from the electronic patient data management system (PDMS) (Clinisoft, GE Healthcare, Chicago, IL, USA). The measured severity of illness scores included the Acute Physiology and Chronic Health Evaluation (APACHE II), 20 the Simplified Acute Physiology Score (SAPS II) 21 and the Sequential Organ Failure Assessment Score scoring systems. 22 Sepsis was defined according to the American College of Chest Physicians/Society of Critical Care Medicine criteria. 23 Delusions and delirium were assessed daily by a subjective nursing assessment (calm and cooperative, restless but cooperative, restless and uncooperative, disoriented and delusional, agitated, dangerously agitated and uncooperative) and recorded to the PDMS. The delirium diagnosis was considered positive if the patient’s status was: restless and uncooperative, disoriented and delusional, agitated, or dangerously agitated and uncooperative. Achieving the standing position during the ICU treatment was recorded as a milestone of rehabilitation and mobilisation. 24
The scores on all eight subdomains in the RAND-36 HRQoL questionnaire (physical functioning (PF); social functioning; role limitations due to physical functioning; role limitations due to emotional functioning; mental health (MH); vitality; bodily pain; general health perception; and health change) were computed on a scale from 0 to 100 with higher scores representing a better HRQoL. In this study, PF and MH were used to stratify the patients to an impaired or normal outcome in comparison with the general healthy population. HRQoL measurements from healthy controls were obtained from the Finnish RAND-36 manual. The manual describes a validation study in a random sample of 3000 Finns aged 18 to 79 years. The results of the PF and MH dimensions in patients participating in this study were compared with the age- and sex-matched control groups of the validation study. Impaired PF or MH were defined if the patient’s RAND-36 score on PF or MH dimension score was more than two standard deviations (SDs) below their age- and sex-matched reference score from the healthy Finnish population (population mean). This impaired level was selected assuming that approximately 2.5% of the population is below that level in approximately normally distributed data. The other group, a normal score group, had scores above the population mean – 2 SDs.
Statistical analysis
Descriptive statistics were used to analyse the data. Summary statistics for continuous or ordinal variables are expressed as medians with 25th and 75th percentiles, and an analysis between groups was performed using the Mann–Whitney U test. Categorical variables were analysed using Fisher’s exact test. P-values less than 0.05 were considered statistically significant. Analyses were performed using the SPSS software program for Windows (IBM Corp., released 2012, IBM SPSS Statistics for Windows, Version 21.0, Armonk, NY, USA).
Results
There were 788 eligible non–cardiac surgical patients between 2004 and 2012 who met the post-ICU clinic’s age and LOS criteria. After the definitive follow-up, using the clinic’s exclusion criteria, another 320 patients (40.6%) were excluded (Figure 1). An invitation to the post-ICU clinic was sent to 468 patients, of whom 351 patients (75%) attended the clinic. PF and MH could be calculated in 332 patients, the majority being male (63%). The median age was 50 (interquartile range (IQR) 38–57) years of age. The median APACHE II and SAPS II scores on admission were 18 (IQR 13–23) and 38 (IQR 28–49), respectively. The median LOS was 7 (IQR 4.8–11.8) days and median hospital stay was 23 (IQR 15–35) days. One hundred and thirty-one patients (39.5%) could be classified as individuals having impaired physical functioning, and 25 patients (7.5%) as individuals with impaired mental wellbeing, as compared with the sex- and age-matched general population control group, according to the RAND-36 data. The RAND-36 questionnaire was filled out by the patient themself in 21 (84%) cases from the impaired MH group versus 276 (90%) cases from the normal MH group. The corresponding numbers were 114 (87%) cases versus 184 (92%) cases, P = 0.198 in the PH strata.
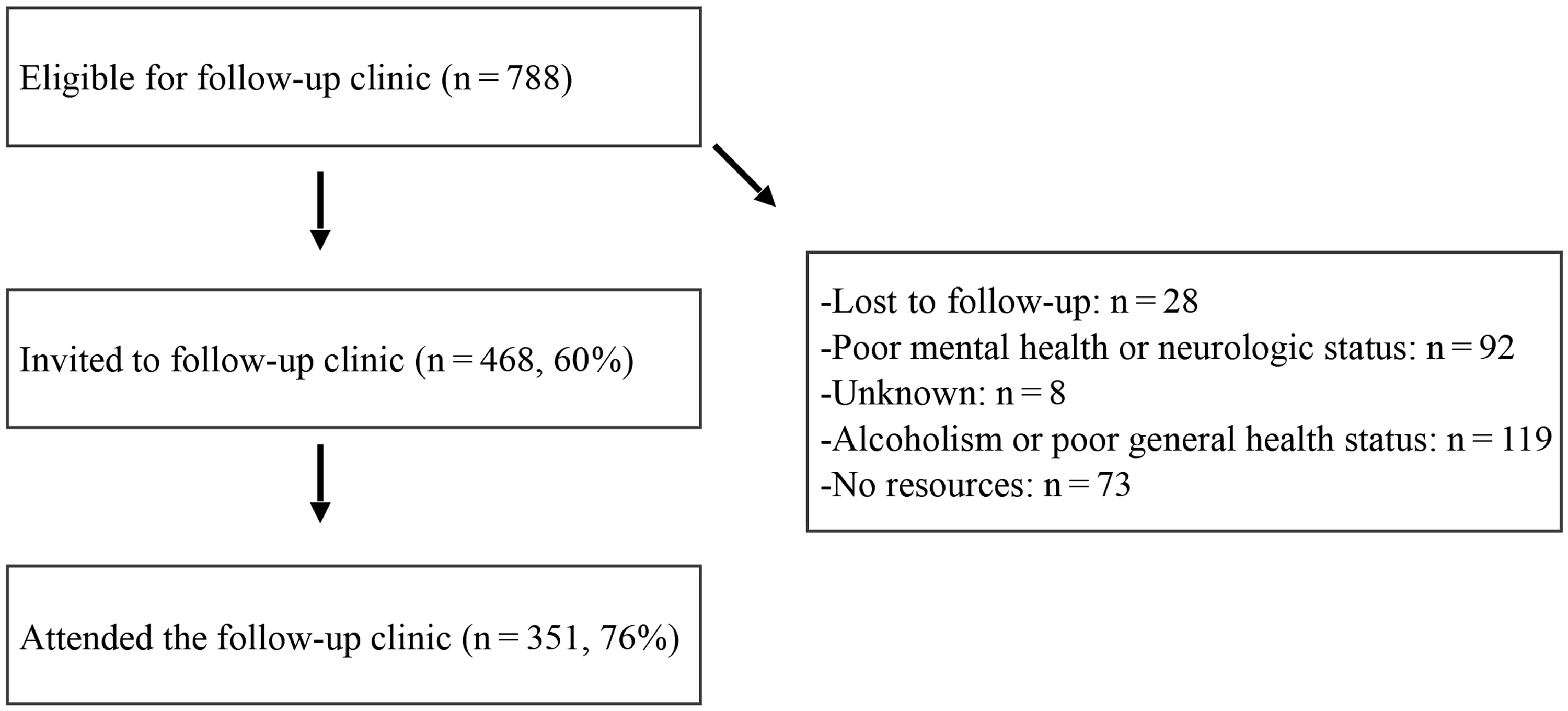
Outline of the follow-up clinic’s patient recruitment and attendance.
Patients with an impaired PF outcome had a longer hospital stay (Table 1). Otherwise, there were no significant differences in the demographics or comorbidities between the impaired and normal outcomes in either of the quality of life dimension groups (PF and MH). Eleven out of 16 (69%) multitrauma patients had impaired PF. During the ICU treatment period (Table 2), patients with an impaired PF were more likely to have received vasopressor infusions (85% versus 73%, P = 0.013). During the follow-up clinic visit (Table 3), 22 patients (7%) had memories of pain. Patients with an impaired PF outcome had more frequent memories of pain related to the ICU treatment (10% versus 4%, P = 0.03), achieved poor results in the 6MWT (393 m versus 500 m, P < 0.001) and in hand-grip tests (left hand 28 kg versus 32 kg, P = 0.004; right hand 29 kg versus 34 kg, P = 0.001) (Table 3). Patients with an impaired PF outcome were also less likely to move independently (69% versus 98%, P < 0.001), and were more likely to be dependent on different assistive devices in their everyday mobility (31% versus 2%, P < 0.001). There was no significant difference in achieving a standing position during the ICU stay between the impaired and normal PF outcome group (21% versus 29%, P = 0.076).
Patient demographics and clinical data categorised to those that reached the population mean and those that did not.
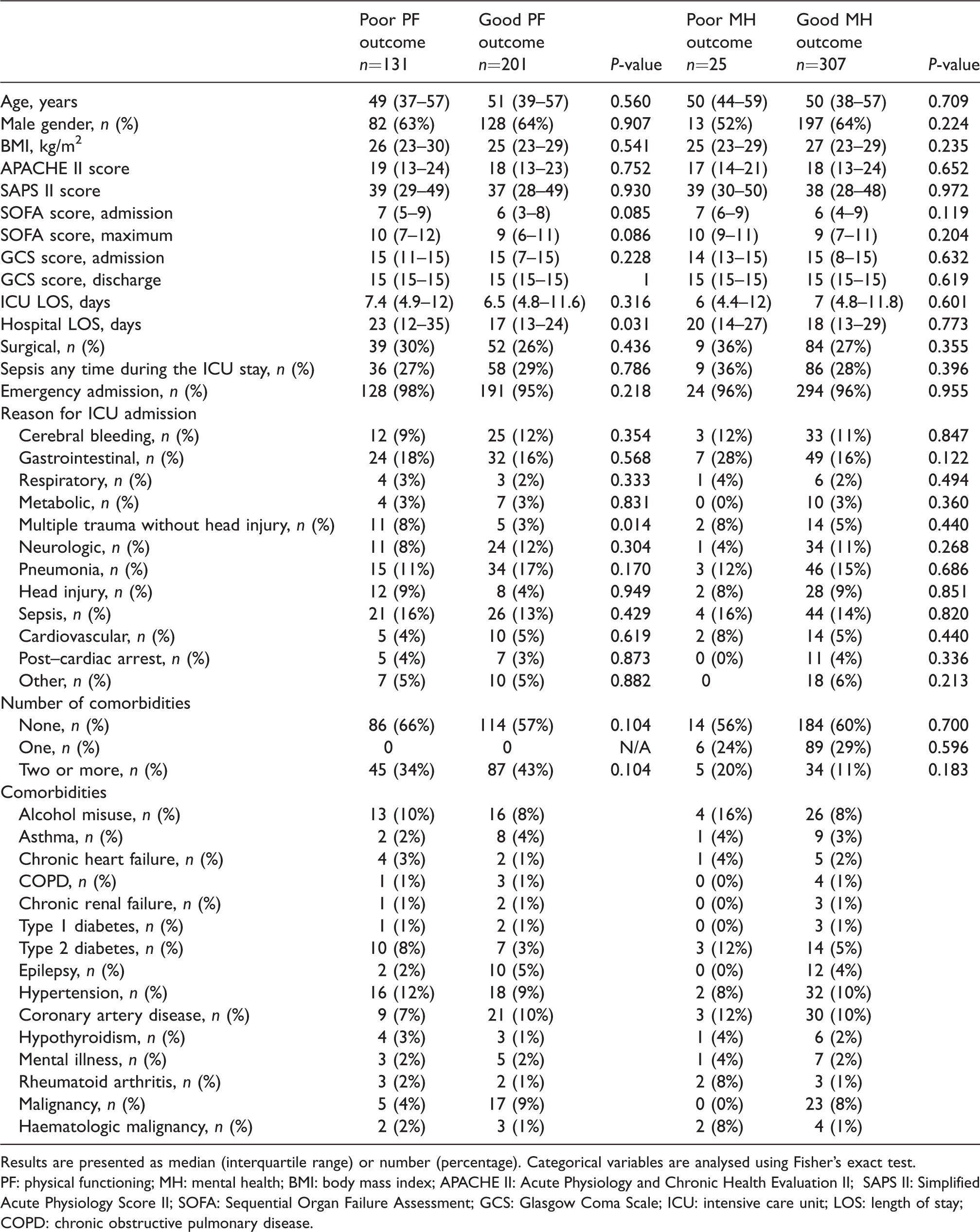
Results are presented as median (interquartile range) or number (percentage). Categorical variables are analysed using Fisher’s exact test.
PF: physical functioning; MH: mental health; BMI: body mass index; APACHE II: Acute Physiology and Chronic Health Evaluation II; SAPS II: Simplified Acute Physiology Score II; SOFA: Sequential Organ Failure Assessment; GCS: Glasgow Coma Scale; ICU: intensive care unit; LOS: length of stay; COPD: chronic obstructive pulmonary disease.
Intensive care unit and treatment events.
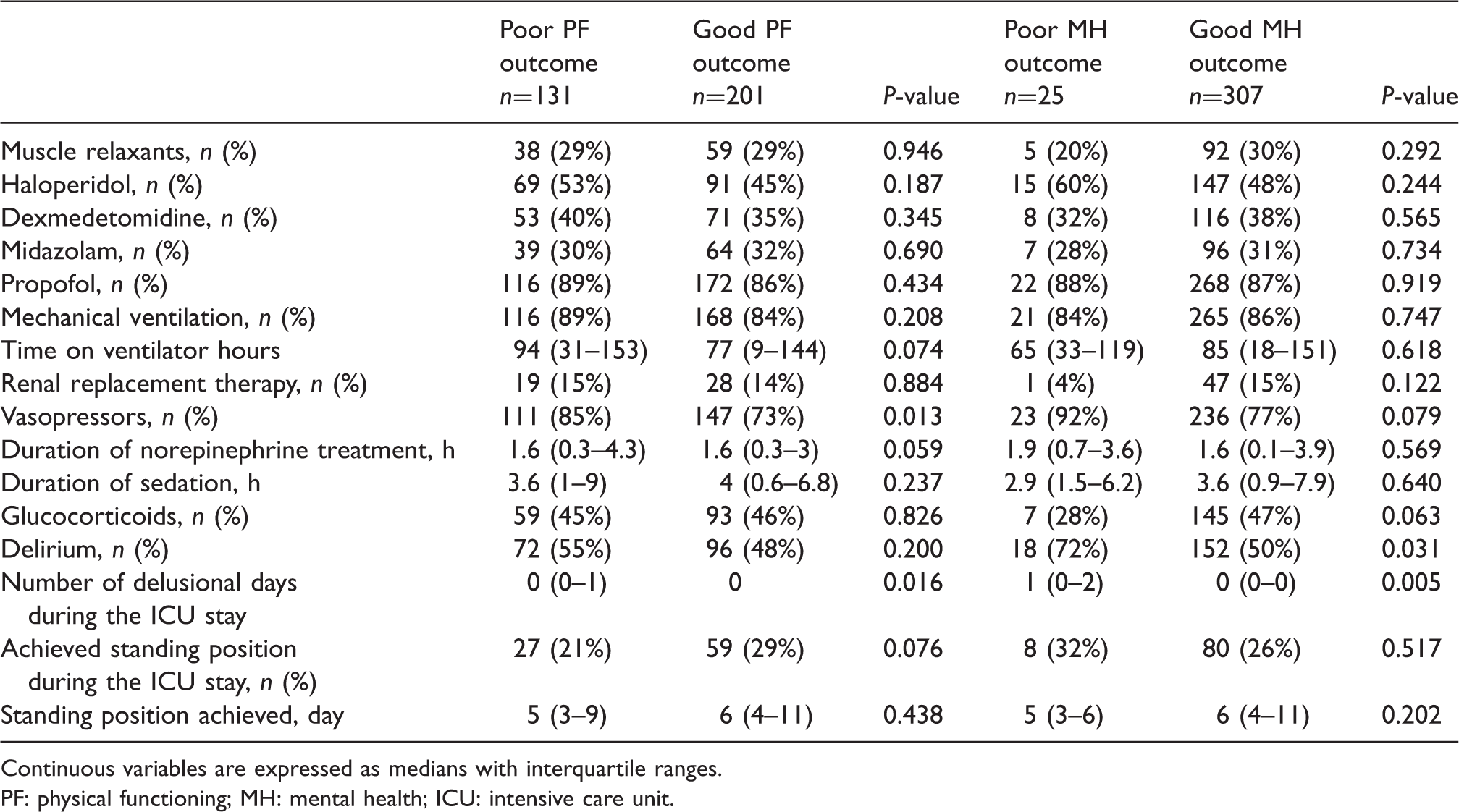
Continuous variables are expressed as medians with interquartile ranges.
PF: physical functioning; MH: mental health; ICU: intensive care unit.
The follow-up clinic data.
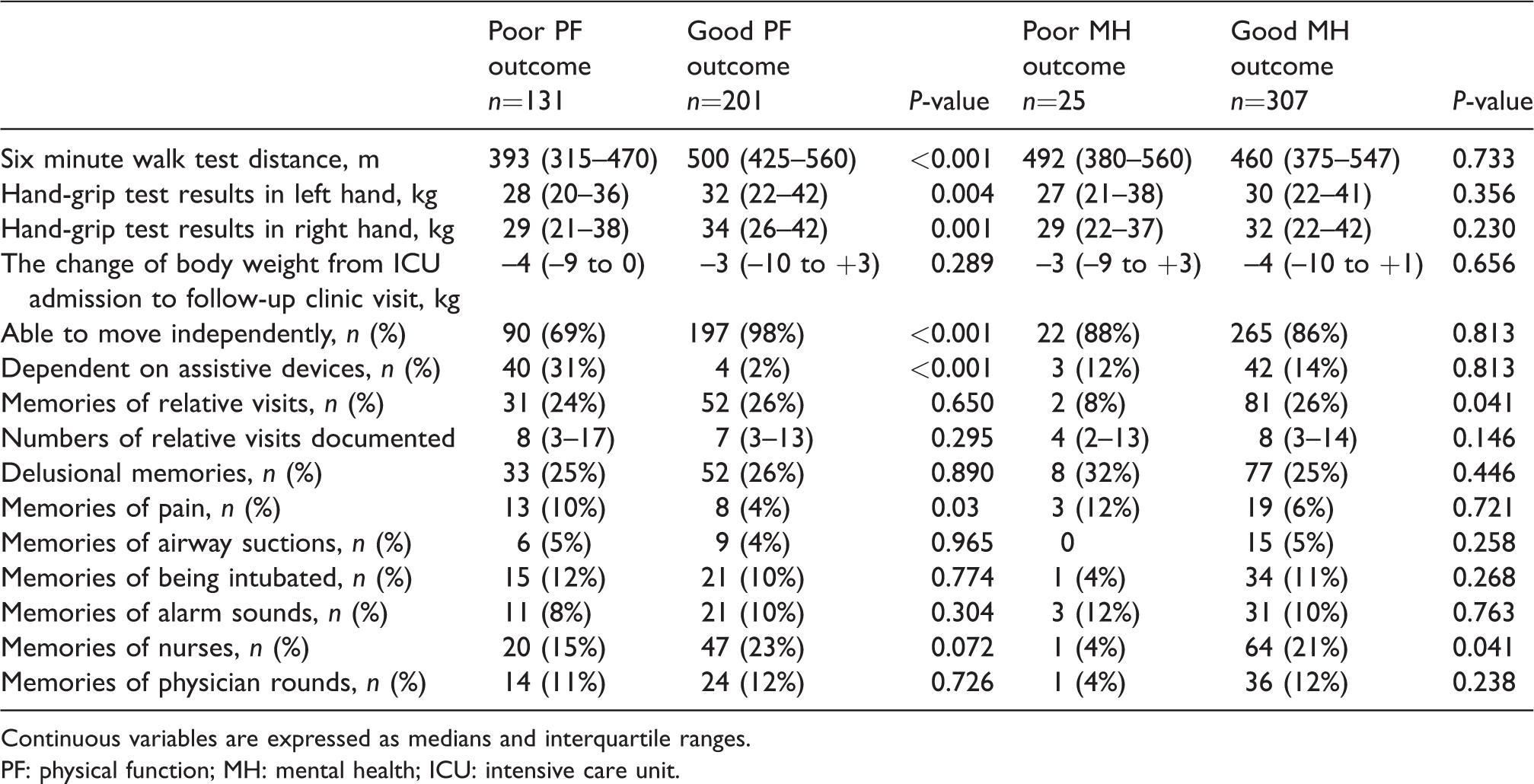
Continuous variables are expressed as medians and interquartile ranges.
PF: physical function; MH: mental health; ICU: intensive care unit.
Patients with an impaired MH outcome were more likely to have suffered delirium during the ICU period (72% versus 50%, P = 0.037). In their interview at the follow-up clinic, patients with an impaired MH expressed fewer memories of visits by relatives (8% versus 26%, P = 0.028) and fewer memories of nurses (4% versus 21%, P = 0.041).
In both impaired outcome groups (MH and PF), all of the RAND-36 HRQoL dimensions were lower compared with the normal outcome groups (Table 4). The only exception to this was the physical role dimension, where the difference did not achieve statistical significance between those patients with an impaired and those with a good MH outcome.
The RAND-36 health-related quality of life dimensions in patients reaching and not reaching two standard deviations below the population mean in physical functioning and mental health.
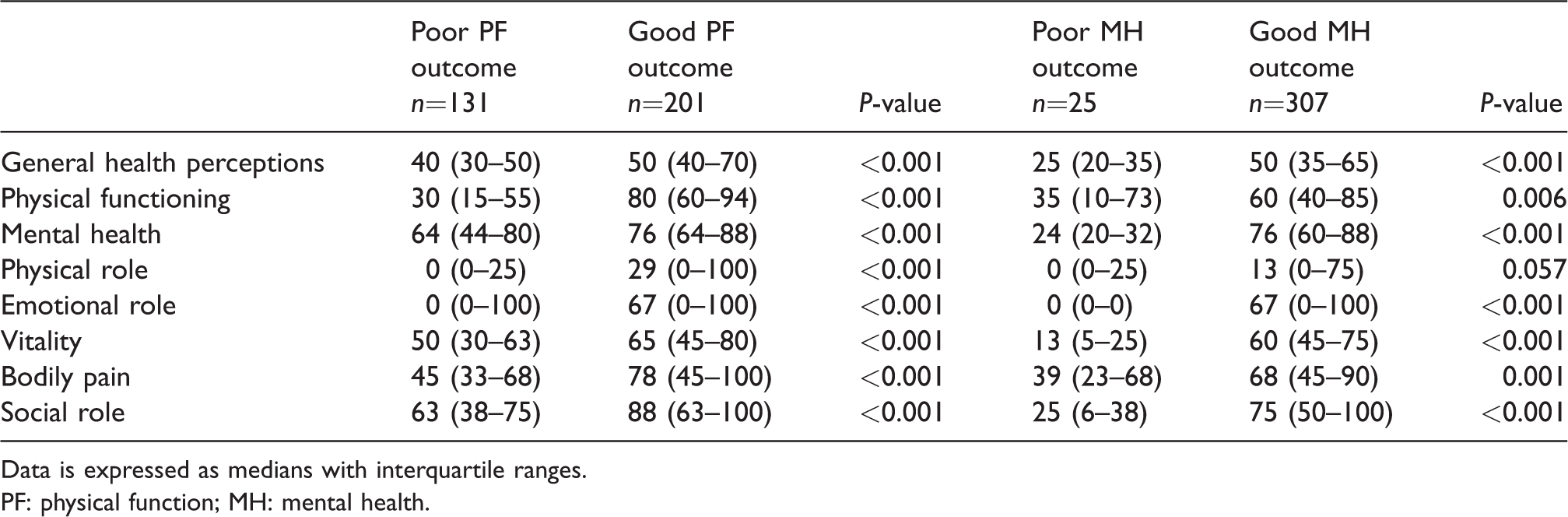
Data is expressed as medians with interquartile ranges.
PF: physical function; MH: mental health.
Discussion
Our study had the following main results: There were no demographic differences between those with impaired or normal PF or MH. Eleven out of 16 (68.8%) multitrauma patients had impaired PF. Those with impaired PF had more memories of pain after ICU treatment, and those with impaired MH had a higher rate of delirium during ICU stay and fewer memories of the ICU stay.
The majority of patients personally filled out the HRQoL questionnaires, and the PF was objectively measured using the 6MWT and the hand-grip test. In a prospective cohort study published in 2016 and conducted in a Canadian post-ICU follow-up clinic with a patient population closely similar to ours, 25 it was demonstrated that decreased results in the hand-grip test and 6MWT were associated with a reduction in the PF domain scores of the RAND-36 questionnaire.
In our study, there were no differences in the number of comorbidities or in the severity of illness on admission between those with impaired and with normal post-ICU PF.
In contrast to this, differing results were previously published in an earlier report. 26 These results considered the effect of pre-ICU comorbidities on post-ICU HRQoL, in a study group composed of patients older than those in our study (median age 58.8 versus 50 years) and using a questionnaire completed at a later stage than in our group (six versus three months after the hospital discharge). 26 These differences in study design might explain the differing results obtained. In a different study, similar conclusions were drawn regarding how the severity of illness on admission, measured using APACHE II scores, was shown not to be associated with an impaired health-related quality of life. 27 The results from these studies, however, might not be generalisable to our selected, working-age study group from a mixed ICU patient population and a three-month follow-up period.
More than one-third of our study population suffered impaired PF in their everyday life, which is similar to that reported in earlier publications. 28 Every fourth one of our patients achieved a standing position during the ICU period. The standing position as an achievement of mobilisation has also been used in other publications. In a German one-day point-prevalence study of mechanically ventilated patients, 29 the standing position at the bedside was achieved by only 2% of mechanically ventilated patients. In our study, no difference in achieving the standing position was observed between those with impaired or with normal PF three months after their ICU stay. In another study, 51% of patients who received early physical and occupational therapy achieved the standing position during mechanical ventilation and 43% of the patients receiving early physical therapy were discharged home. 24 Taken together, although the standing position could be a good measure of body control and a marker of global PF, our study does not support this; 71% of those with a normal PF at three months post-discharge had not achieved a capacity to stand during the ICU stay.
In our series, only 7% of the patients had memories of pain three months after their ICU stay. This is lower than that reported in an earlier study, with 40% of patients reporting memories of pain three months after the ICU stay. 30 Memories of pain have been reported to be an independent risk factor of post-traumatic stress symptoms. 31 We have no data on post-traumatic stress symptoms, but interestingly in our series there was no difference in the frequency of memories of pain between those with impaired and those with normal MH. However, those with impaired PF more often had memories of their pain experience during their ICU stay in our series, highlighting the importance of adequate analgesia during the ICU period.
At the follow-up clinic visit, the majority (68%) of patients with an impaired physical outcome were unable to walk or mobilise themselves without assistance and one-third of them needed assistive devices to enable their mobilisation. In the 6MWT, the mean values were 393 m in patients with an impaired PF and 500 m with a normal PF. It is notable that both of these values differ from the Finnish reference values, which are 572 m in males and 538 in females aged 60–69 years (the mean values in the younger population have not been validated). This finding may suggest that a patient’s own expectations of their physical capacity were more optimistic compared with reality when they filled in the PF section of the RAND-36 questionnaire. Also, patients with an impaired PF outcome self-reported a significant decrease (mean value below –2 SD) in every HRQoL dimension including general health perceptions, emotional wellbeing, physical role, emotional role, vitality, bodily pain and social role. This finding suggests that the impaired PF outcome is related to an immense and complex burden on an individual’s everyday life after critical illness.
Only 8.1% of patients in our study experienced an impaired MH status at the three-month follow-up visit, which was only slightly more than the Finnish annual average of 5% in the prevalence of depression. 32 In previous reports, the prevalence of post-ICU MH disorders has been shown to be much more frequent.3,4,7,33 The only peri-ICU factor associated with an impairment in MH subsequently was delirium during the ICU stay. This risk factor is known to be associated with cognitive dysfunction after ICU treatment. 34 During the follow-up clinic visits, patients with a better MH outcome expressed more actual memories of the visits by their relatives and also memories of the ICU nurses. This finding supports earlier findings that memories of real events during critical illness may protect from later anxiety and the development of post-traumatic stress disorder–related symptoms. 35
Our study has several limitations. First, in the assessment of delirium we have focused on hyperactive delirium, as we did not use a true confusion assessment module (e.g. ICU-CAM). Both hypo- and hyperactive forms of delirium may impact on subsequent symptoms and thus our assessment may underestimate the true frequency of delirium in our material.
Second, our study population was biased towards patients achieving better outcomes in both PF and MH status. This was due to our post-ICU follow-up clinic’s invitation policy, which focuses on working-age patients. Our invitation policy also excluded some patient groups (mentioned above) who were assumed not to benefit from rehabilitation information and debriefing conversation. We can assume that the HRQoL was significantly lower in these patient groups compared with the general population mean values.
Third, almost a quarter (24.5%) of the patients who were invited to the follow-up clinic did not attend or return the questionnaires. The actual PF and MH outcomes in these patients remained unclear. If the population of non-attenders hypothetically included more normal or impaired PF and MH ICU survivors, this might significantly impact on the study results.
Fourth, in this study, the pre-ICU data of the patients’ physical capacity, psychological status and HRQoL was not available. Thus, we have no reliable data or baseline values of the patients’ pre-ICU status as regards PF and MH at the follow-up clinic visit, and we cannot be certain whether our patients had any PF or MH impairment before their critical illness. However, our aim was not to examine the effect of any ICU treatment on the patients’ PF or MH, but rather to document ICU patients’ PF and MH status at three months after hospital discharge to enable initiation of any necessary therapeutic and/or supportive interventions.
Clinical impact and future studies
Longitudinal studies containing prospective data from ICU patients’ medical and socioeconomic history would be informative when defining more accurate prognostic factors considering the long-term outcomes after critical illness. More accurate prognostic factors of impaired outcomes will be helpful to guide the planning of rehabilitation services for those who are most at risk of developing PF or MH problems after their critical illness. Our results suggest that patients who had delirium, multitrauma, delusional memories or memories of pain during their ICU stay are mostly likely to benefit from further follow-up after their hospital discharge.
Conclusion
Impaired PF was more frequent than impaired MH at three months after critical illness in working-age adults. Multitrauma and memories of pain were risk factors for subsequent impairment in physical function. Delirium during the ICU stay and a lack of memories of visits by relatives or the attending nurses were related to MH after critical illness.
Supplemental Material
Supplemental material for Factors associated with impaired physical functioning and mental health in working-age patients attending a post–intensive care follow-up clinic three months after hospital discharge
Supplemental Material for Factors associated with impaired physical functioning and mental health in working-age patients attending a post–intensive care follow-up clinic three months after hospital discharge by Miikka Niittyvuopio, Janne H Liisanantti, Jaana Pikkupeura, Michael B Spalding, Sinikka Sälkiö and Tero I Ala-Kokko in Anaesthesia and Intensive Care
Footnotes
Acknowledgement
The expertise of our follow-up clinic nurses in patient care is highly appreciated.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.