
Abstract
Iron deficiency is common in colorectal cancer. Despite perioperative guidelines advocating for the correction of non-anaemic iron deficiency prior to major surgery, the impact of this pathology on postoperative outcome is unclear.
We conducted a single-centre, historical cohort study of 141 elective resections for colorectal cancer. We stratified non-anaemic patients into iron deficient and iron replete groups, and collected data on baseline characteristics, preoperative laboratory results, intraoperative events and postoperative outcomes. As this study was an exploratory work for future research, a P-value of 0.25 was considered relevant. Patients in the deficient group demonstrated lower baseline ferritin (median (interquartile range, IQR) 76 (41–141) µg/L versus 207 (140–334) µg/L, P < 0.001) and transferrin saturation (mean (standard deviation, SD) 18% (8%) versus 32% (12%), P < 0.001) than those in the replete group, and lower starting haemoglobin (mean (SD) 138 (10) g/L versus 144 (12) g/L, P = 0.01). The deficient group had increased re-admission (25% (24%) versus 4% (11%), P = 0.15) and all-cause infection (25% (24%) versus 5% (14%), P = 0.24). A decrease of two days in days alive and out of hospital at postoperative day 90 was seen in the deficient group on univariate analysis (median (IQR) 81 (75–84) versus 83 (78–84), P = 0.25). This reduced to 1.24 days in multivariate adjusted quantile regression analysis (P = 0.22). Days alive and out of hospital at day 90, postoperative re-admission and postoperative infection may be meaningful outcome measures for future prospective observational work examining non-anaemic iron deficiency in patients undergoing major surgery for colorectal cancer.
Introduction
Preoperative anaemia is associated with morbidity and mortality in patients undergoing major surgery. 1 The most frequent cause of anaemia in patients undergoing surgery for colorectal cancer is iron deficiency.2,3 Perioperative guidelines and consensus statements recommend aggressive management of iron deficiency anaemia as a key component of prehabilitation prior to major surgery,4–7 and large, randomized, controlled trials examining the role of parenteral iron in managing preoperative iron deficiency anaemia are ongoing. 8
While negative consequences of preoperative anaemia are increasingly recognized, there is little in the literature that addresses non-anaemic iron deficiency as a target for preoperative intervention. Evidence extrapolated from studies in exercise physiology
9
and heart failure
10
suggest that correcting non-anaemic iron deficiency with intravenous iron preparations is associated with improved quality of life. Management guidelines increasingly recommend correcting iron deficiency regardless of haemoglobin concentration.6,7 However, these recommendations lack prospective validation. Possible targets for future prospective research may include:
Determining whether non-anaemic iron deficiency is associated with adverse postoperative outcomes, and; If associated with adverse effects, a) can non-anaemic iron deficiency be corrected with iron supplementation, and b) is postoperative outcome subsequently improved?
As part of a research programme investigating the prevalence of non-anaemic iron deficiency in patients undergoing major surgery for colorectal cancer and its consequences for postoperative outcome, and to provide data for the design and feasibility of future work, we undertook a retrospective analysis of all non-anaemic elective patients who underwent resection of a primary colorectal malignancy in our centre between January 2013 and December 2016. This historical cohort study explores associations between non-anaemic iron deficiency and: 1) length of hospital stay, 2) days alive and out of hospital, and 3) incidence of postoperative complications, relative to a non-anaemic and iron replete group.
Methods
The study was approved by the Austin Health human research ethics committee with a waiver of individual patient consent (LNR/17/Austin/137). We evaluated consecutive patients who underwent elective resection of a colorectal malignancy between January 2013 and December 2016, via retrospective extraction of data from the electronic medical record (Cerner Corporation, North Kansas City, MO, USA). Patients were excluded from the cohort if they were anaemic at the time of pre-anaesthetic assessment, had received parenteral iron as part of a preoperative programme of optimization or had missing data that prevented accurate classification of their iron status. Anaemia was defined using the current World Health Organization criteria of a haemoglobin concentration (Hb) of less than 130 g/L for men and less than 120 g/L for women. 11
We stratified participants into two groups, using iron studies performed at the time of pre-anaesthetic assessment: 1) non-anaemic and iron replete (replete), and 2) non-anaemic but iron deficient (deficient). The definition of iron deficiency is based on common criteria used in the literature.3,10
Iron deficient was defined as: a.Absolute iron deficiency: serum ferritin of <100 µg/L (regardless of transferrin saturation (TSAT) or C-reactive protein (CRP) level), or; b.Functional iron deficiency: serum ferritin of 100–300 µg/L, where TSAT was <20% and/or CRP >5 mg/L. Iron replete was defined as serum ferritin >100 µg/L, where TSAT was >20% and CRP <5 mg/L.
We collected data describing preoperative characteristics: age; sex; height; weight; current history of diabetes mellitus, hypertension, cardiac failure or smoking; and American Society of Anesthesiologists (ASA) category. Baseline laboratory data from the time of anaesthetic pre-assessment were collected. This included baseline Hb, platelet count and mean corpuscular volume; prothrombin time, activated partial thromboplastin time (aPTT) and fibrinogen level; serum ferritin, CRP and TSAT; and serum urea, creatinine and albumin. We estimated mortality risk using the ColoRectal Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity (CR-POSSUM). 12
Intraoperative data included use of laparoscopic or laparoscopic-assisted approach; duration of surgery (defined as the time from first recorded to last recorded measurement on the anaesthetic record); the stage of malignancy using Dukes' criteria; and the graded surgical complexity: 1) major: isolated or extended right or left hemicolectomy or sigmoid colectomy, or 2) complex: abdominoperineal, low or ultralow anterior resection.
Postoperative outcome data included: length of acute care stay; requirement for, and duration of, subacute care admission (fast- or slow-stream rehabilitation); details of any re-admission to acute care within the first 90 postoperative days; planned or unplanned intensive care or high dependency admission; unplanned return to theatre; the Hb on postoperative day 3; the difference between Hb taken at pre-anaesthetic assessment and that taken on postoperative day 3; Hb at time of acute care discharge; requirement for allogeneic blood transfusion during initial acute care stay; incidence of wound infection (defined by a requirement for inpatient antibiotic therapy); incidence of other infection (such as lower respiratory or urinary tract infection, and again, defined by requirement for inpatient antibiotic therapy); mortality within the first 90 postoperative days; and days alive and out of hospital (DAOH) at postoperative days 30 and 90. 13
The DAOH-90 was the primary outcome measure. DAOH was originally described as a health economic measure.14–16 It is calculated by subtracting the total amount of time spent by the patient away from their setting of usual care (i.e. home) as a consequence of an index clinical event (such as surgery), from the time available for follow-up (i.e. 30 days, 90 days, etc.). Secondary outcome measures included DAOH-30; acute care length of stay; requirement for re-admission to acute care; allogeneic blood transfusion at any point of the initial inpatient stay; mortality on postoperative day 90; Hb on postoperative day 3; difference between baseline and postoperative day 3 Hb; Hb on discharge from acute care; incidence of postoperative wound infection; incidence of any other postoperative infection; and incidence of any infection in the immediate postoperative period.
Every patient who underwent surgery in our institution that met the study criteria within the defined period was included. The start of the study period (January 2013) was determined by the start date of a hospital practice change to where routine iron studies were performed as part of the pre-admission process, regardless of Hb, for all patients undergoing surgery for colorectal cancer.
Continuous data are presented as means and standard deviations or, where data are non-parametric, as medians and interquartile ranges. Categorical data are presented as frequency and percentage. The deficient and replete populations were compared at baseline using unpaired Student’s t-tests for normally distributed data and the Kruskall–Wallis test for data that were not normally distributed. For binary variables the chi-square test was used to compare the populations of patients. The same analyses were conducted on post-baseline secondary outcomes. DAOH-30 and DAOH-90 were compared between the different populations of patients using quantile regression. 13 A multivariate quantile regression was also performed including the following factors in addition to population group: age, sex, body mass index, CR-POSSUM mortality score, estimated glomerular filtration rate, whether neoadjuvant therapy was given, whether a laparoscopic, or laparoscopic-assisted, approach was performed, presence of diabetes mellitus, active smoking history and duration of procedure. The analysis was conducted in keeping with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 17 Because this was an exploratory and feasibility study, and to avoid excluding findings that may be of use in future research, we considered a P-value of 0.25 to be significant.
Results
A total of 265 patients received elective surgery for colorectal cancer during the study period and were screened for inclusion. Exclusions (Figure 1) included: 74 (28%) who were anaemic at the time of pre-anaesthetic assessment, 33 (12%) who received parenteral iron, 1 (0.4%) who received erythropoietin as part of a preoperative optimization strategy, four (2%) who received planned elective surgery emergently due to bowel obstruction and 12 (5%) with missing data. The final non-anaemic study cohort totalled 141 patients, of whom 36 (26%) were classified as replete and 105 (74%) as deficient. Compared with the replete group (Table 1), the deficient group had fewer women (51 (49%) versus 27 (75%), P = 0.01) and active smokers (13 (12%) versus 12 (32%), P = 0.01).
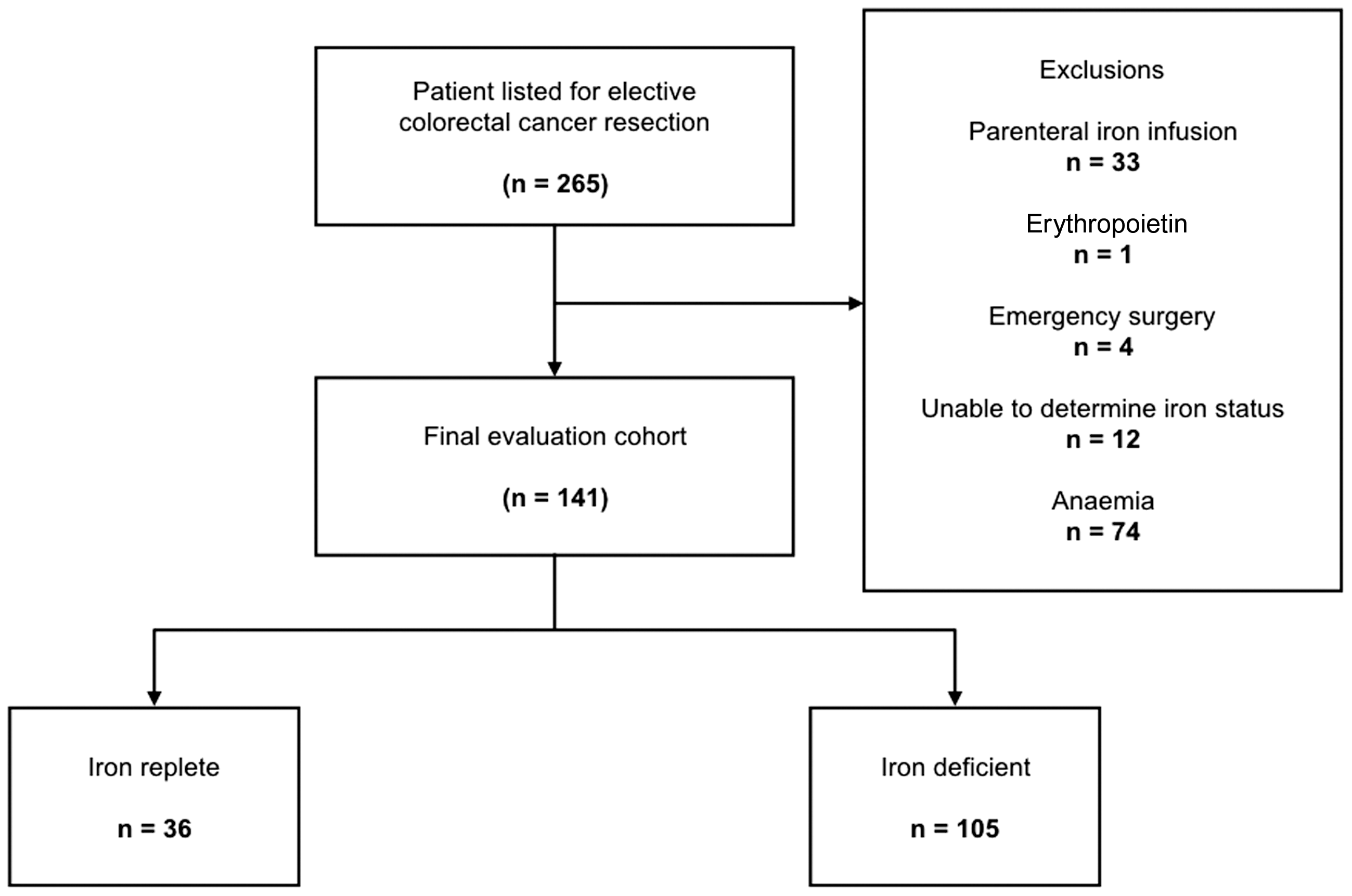
STROBE-style representation of study exclusions and group stratifications (Strengthening the Reporting of Observational Studies in Epidemiology).
Participant characteristics.
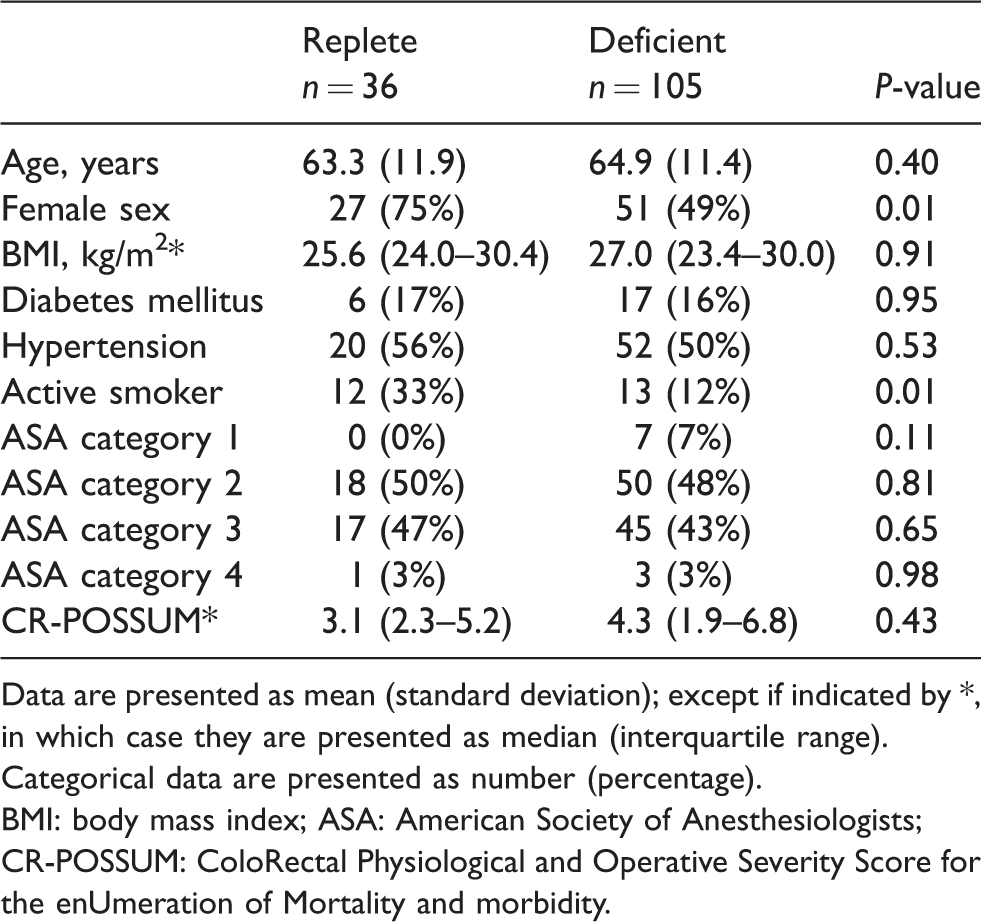
Data are presented as mean (standard deviation); except if indicated by *, in which case they are presented as median (interquartile range). Categorical data are presented as number (percentage).
BMI: body mass index; ASA: American Society of Anesthesiologists; CR-POSSUM: ColoRectal Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity.
Consistent with the group allocation criteria (Table 2), patients in the deficient group demonstrated a lower ferritin (median (interquartile range, IQR) 76 (41–141) µg/L versus 207 (140–334) µg/L) and TSAT (mean (standard deviation, SD) 18% (8%) versus 31% (12%)) than those in the replete group, and a lower starting Hb relative to the replete cohort (mean (SD) 138 (10) g/L versus 144 (12) g/L, P = 0.01).
Preoperative laboratory studies.
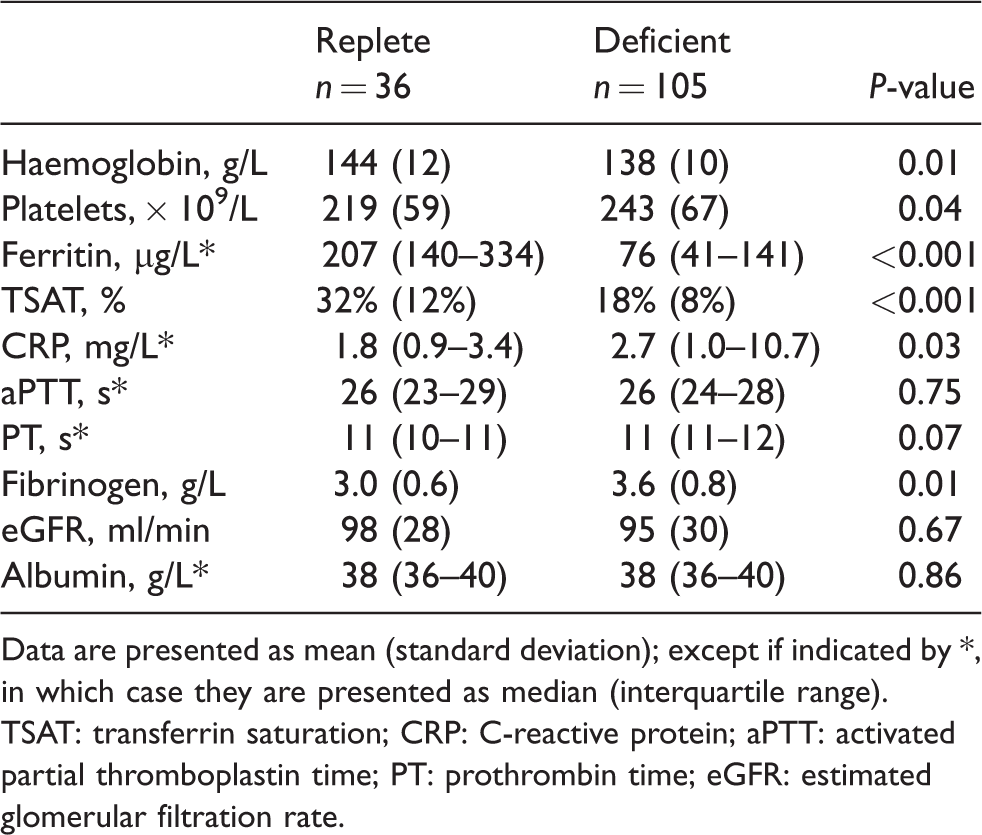
Data are presented as mean (standard deviation); except if indicated by *, in which case they are presented as median (interquartile range).
TSAT: transferrin saturation; CRP: C-reactive protein; aPTT: activated partial thromboplastin time; PT: prothrombin time; eGFR: estimated glomerular filtration rate.
No substantive, systematic differences were noted between the deficient and replete groups for stage of malignancy, operation type or technique, or duration of surgery (Table 3).
Intraoperative data.
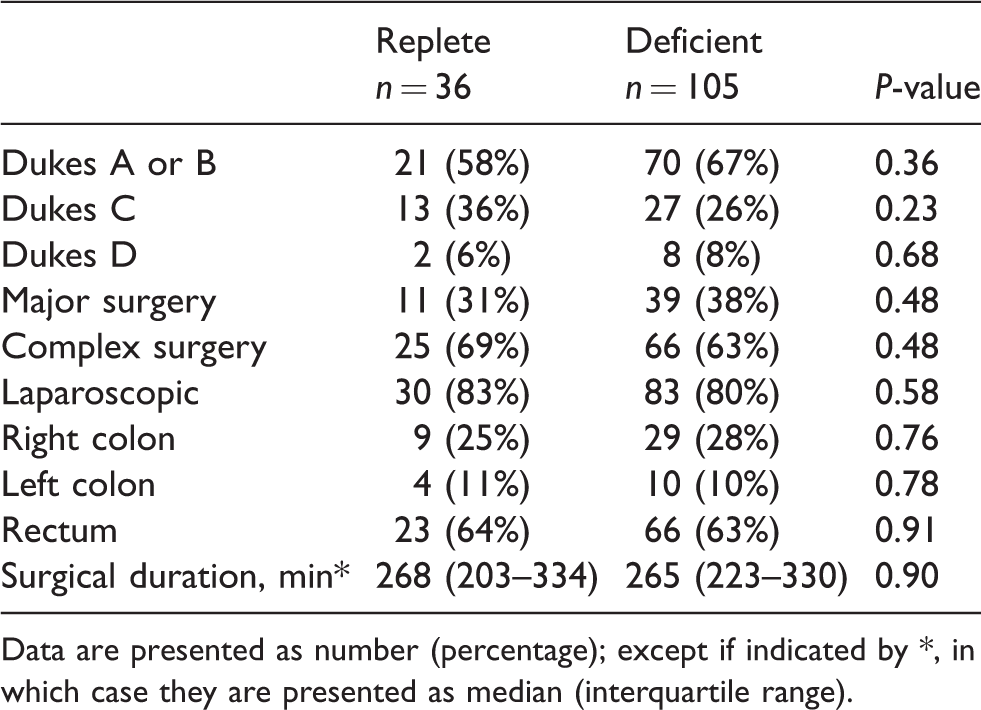
Data are presented as number (percentage); except if indicated by *, in which case they are presented as median (interquartile range).
Compared with the replete group, the deficient group (Table 4) had a lower Hb on postoperative day 3 (mean (SD) 116 (17) g/L versus 123 (21) g/L, P = 0.05) and a lower Hb on acute care discharge (mean (SD) 116 (17) g/L versus 125 (20) g/L, P = 0.01). Furthermore, the deficient group had roughly double the rate of re-admission to acute care (25 (24%) versus 4 (11%), P = 0.15), which in turn was a major factor in the observed difference in DAOH-90 of approximately two days on univariate analysis (81 (75–84) days versus 83 (78–84) days, P = 0.25). Where re-admission occurred, irrespective of iron status, it was for a substantial period (median (IQR) 9 (6–14) days). The most common reason for re-admission was infection (13 (45%)), followed by small bowel obstruction or ileus (6 (21%)), high output stoma and acute kidney injury (3 (10%)), non-specific abdominal pain (2 (7%)) and other causes, including gastrointestinal bleeding, subsequent procedures for metastatic disease and ischaemic bowel (5 (17%)).
Results of the multivariate analysis of DAOH are shown in Table 5 and Figure 2. The univariate decrease in DAOH-90 seen between the deficient and replete group of two days was reduced to 1.24 days after adjustment for age, sex, body mass index, CR-POSSUM score, estimated glomerular filtration rate, neoadjuvant therapy, laparoscopic technique, diabetes mellitus, active smoking status and duration of surgery (P = 0.22).
Missing data were composed of six baseline serum albumin and 12 coagulation profiles (incorporating prothrombin time, aPTT and fibrinogen). At 52 discrete measurements per patient, these missing data total 42 of a possible 7332 data points, or 0.57% of all possible data.
Discussion
We conducted a single-centre, historical cohort study of non-anaemic patients undergoing major or complex surgery for colorectal malignancy. The purpose of this study was to explore the prevalence of iron deficiency within this population, examine the association between non-anaemic iron deficiency and postoperative outcomes, and to assist in the design of future prospective work. Our results have three implications for the feasibility of future research in this area. First, non-anaemic iron deficiency is a common problem, affecting up to 50% of patients presenting for elective surgery for colorectal cancer. Second, 30-day follow-up after major intra-abdominal surgery may inadequately represent the possible medium- to long-term consequences of surgery and that future perioperative trials in this population should consider extending follow-up to 90 days in order to capture late complications and, particularly, multiday re-admission. Finally, a difference in 90-day DAOH (or home days) of one to two days is a reasonable anticipated difference between iron deficient and replete non-anaemic patients.
The results of this study are highly generalizable to first-world colorectal surgical practice. Data collected represent a comprehensive cohort from a major tertiary centre and account for both absolute and functional iron deficiency. Broad inclusion criteria have produced a study population that is likely to be representative of the patient cohort in other institutions. Our work demonstrates that a prospective study examining this condition is feasible and provides direction for statistical analysis and study powering.
The shortcomings of this project relate largely to its retrospective and exploratory nature. First, whilst we were able to record data pertaining to all re-admission episodes at our institution, we were not able capture data relating to other institutions. Some patients, particularly those who live in a rural environment, may have been admitted to other facilities without our knowledge, with implications for the incidence of re-admission during convalescence, as well as DAOH. Second, retrospective data collection increases the incidence of incomplete records and, in turn, incurs a risk of residual measurement error. We were limited in data collection to that information available from the electronic medical record, and unmeasured data (such as a frailty status, intraoperative blood loss, etc.) would need to be accounted for in subsequent prospective work.
A common concern with pilot or feasibility studies is interpretation of statistical significance. 18 The purpose of studies such as ours is to not provide definitive evidence of an association between non-anaemic iron deficiency and poor postoperative outcome, but, as Lee et al. suggest, ‘…to inform both the decision whether to conduct a confirmatory study, and the design of the larger confirmatory trial’. 19 To achieve this, we used increased α-levels to adequately identify important variables.20–22 Using an α-level of 0.25, several metrics we have measured are possible associations that may be targeted in future work, specifically DAOH-90, requirement for acute-care re-admission, and all-cause infection.
Preoperative iron deficiency with anaemia is associated with several adverse postoperative outcomes.23–25 Recently, best practice guidelines and international consensus statements have recommended the correction of non-anaemic iron deficiency before major surgery. These recommendations have been made despite a relative paucity of evidence for adverse effects of non-anaemic iron deficiency in surgical patients, particularly those undergoing surgery for colorectal cancer.6,7 In 2005, Beale et al. published a single centre series on the incidence of iron deficiency in colorectal cancer patients at time of presentation, finding that 26 of 105 (25%) demonstrated a TSAT <15% with a ferritin of >50 µg/L. However, this series did not attempt to link iron status or haemoglobin level with outcome. 2 Most recently, Wilson and colleagues have published a similar single-centre, historical cohort study of 339 patients examining the interplay between iron status and haemoglobin level in a similar patient population. Univariate analysis showed that severe iron deficiency (defined by a TSAT of <10%) was associated with a marked increase in the risk of complications, but once multivariate analysis was performed accounting for age, sex, ASA score, type of surgery and tumour location, this relationship was no longer statistically significant (odds ratio = 1.84, 95% confidence interval 0.94–3.60, P = 0.074), although the confidence interval suggested the presence of a clinically relevant result. 3 Our results suggest that non-anaemic iron deficiency is widespread, with 49% of all patients presenting for major surgery for a colorectal malignancy at our institution over the study period meeting accepted diagnostic criteria for non-anaemic iron deficiency. 10 It is not clear the extent to which this result reflects the known geographic variation in iron status, which in turn may reflect racial and socioeconomic factors.25,26
As perioperative medicine evolves, a large, international collaborative is working to define and standardize core outcomes to benchmark research in this area. 27 One patient-centred outcome metric that has attracted recognition is DAOH (or days at home), a patient-centred measure that incorporates mortality, hospital length of stay and duration of any re-admission. DAOH takes into account the physiological insult of the index event, and any early complications, and the burden of care that results from referral to subacute care and rehabilitation, and subsequent re-admission. It provides a more complete record and weighting of late complications which would not be reflected in more conventional metrics, such as length of hospital stay. Unlike length of hospital stay, increased DAOH is a positive outcome.
While this novel measure is being increasingly incorporated into clinical research, there remain some complexities associated with its use, specifically, the a priori definition of the time available for follow-up. Whilst a 30-day follow-up has been validated in the perioperative setting, 13 it is not clear whether this time period captures all late complications following the index surgery. This was highlighted by the third report of the National Emergency Laparotomy Audit (NELA) in the United Kingdom, which demonstrated an increase in mortality at 90 days, relative to mortality at 30 days, across all operative urgency and ASA categories. 28 These data do not provide information on the length of any inpatient stay or stays leading up to the date of death, or the causes of death, but they do raise the possibility that a 30-day follow-up period may be insufficient to detect late complications.
Our results may support the signal reflected in NELA, specifically, that major intra-abdominal surgery is associated with late complications. As noted in Table 4 of our study, there is no appreciable increase in length of stay during the immediate postoperative period on the basis of iron status (as shown by effectively equal length of hospital stay and DAOH-30 between the two groups). However, there is an overall increase in hospital re-admission in the deficient group, with an incidence of 24% compared with 11% in the replete group. These re-admissions represent later events, only fully emerging when the DAOH-90 data are considered and represent major complications sufficient to justify emergent re-admission to hospital. Therefore, not only do these episodes represent the financial cost of bed occupancy, but include the cost of investigation and treatment for an acute, late deterioration. 29 Data from The Netherlands has costed minor and major complications at €1623 and €16,059 respectively, 30 with associated cost to the patient, in long-term survival, 31 and individual financial burden. 32 Data from the Australian Institute of Health and Welfare showed that 16,682 new colorectal malignancies were diagnosed in Australia in 2017, representing 12.4% of new cancer diagnoses. 33 After exclusions for parenteral iron infusions and indeterminate iron status, and assuming our results are reproducible between centres, our results suggest that 49%, or 8109, of these patients may be affected by non-anaemic iron deficiency. If the signal demonstrated in our study can be validated with a larger prospective work, there would be substantial health economic implications. Given that the cost of a single bed-day in our institution is roughly AUD$1500, increasing DAOH-90 by a single day in non-anaemic, iron deficient patients would translate to a conservatively estimated cost saving of AUD$12.1m, although the costs of outpatient iron infusion (drug supply and clinical supervision of any planned infusion) would need to be accounted for in any comprehensive health economic analysis.
Postoperative outcomes.
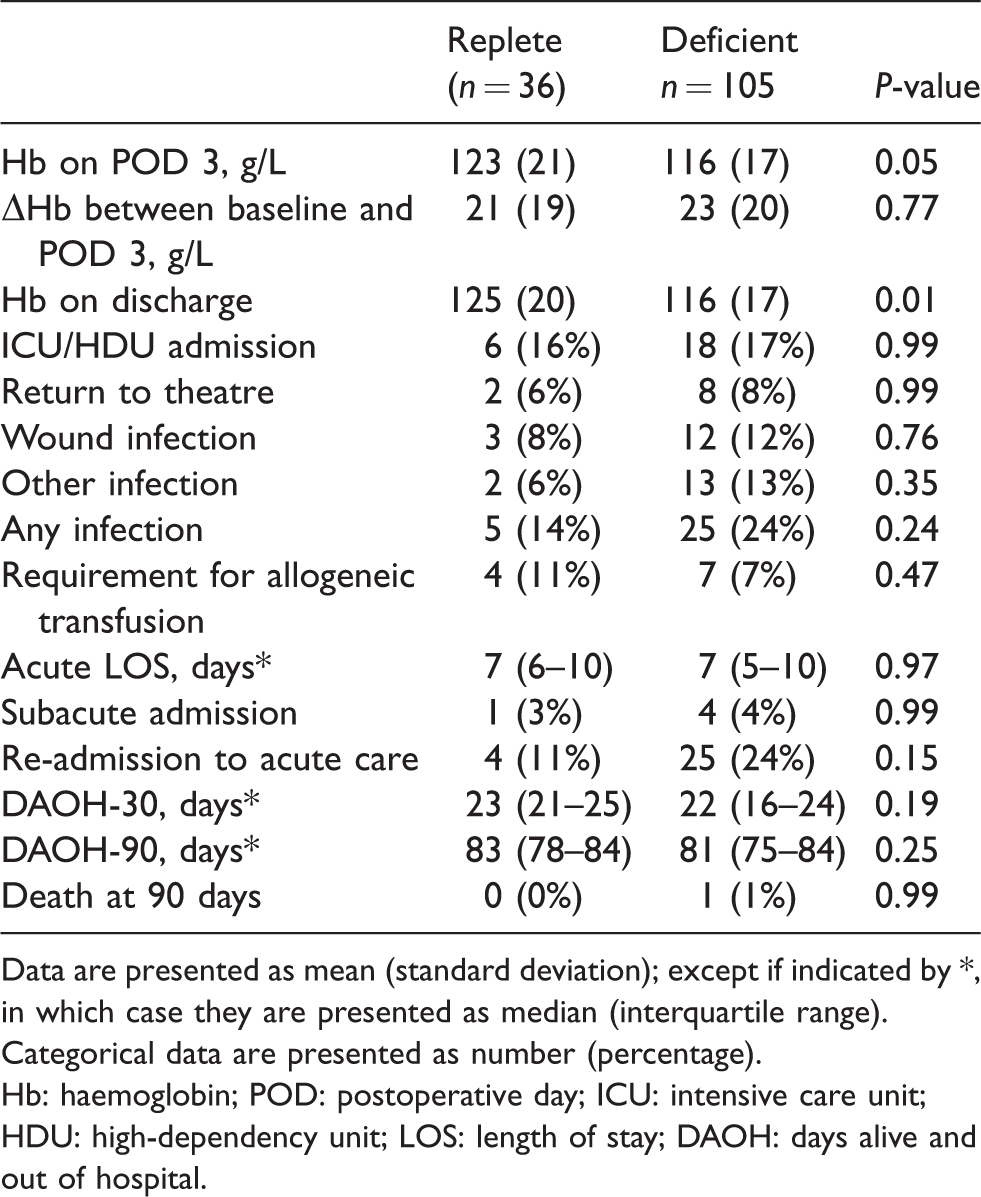
Data are presented as mean (standard deviation); except if indicated by *, in which case they are presented as median (interquartile range). Categorical data are presented as number (percentage).
Hb: haemoglobin; POD: postoperative day; ICU: intensive care unit; HDU: high-dependency unit; LOS: length of stay; DAOH: days alive and out of hospital.
Univariate and multivariate analysis of days alive and out of hospital.
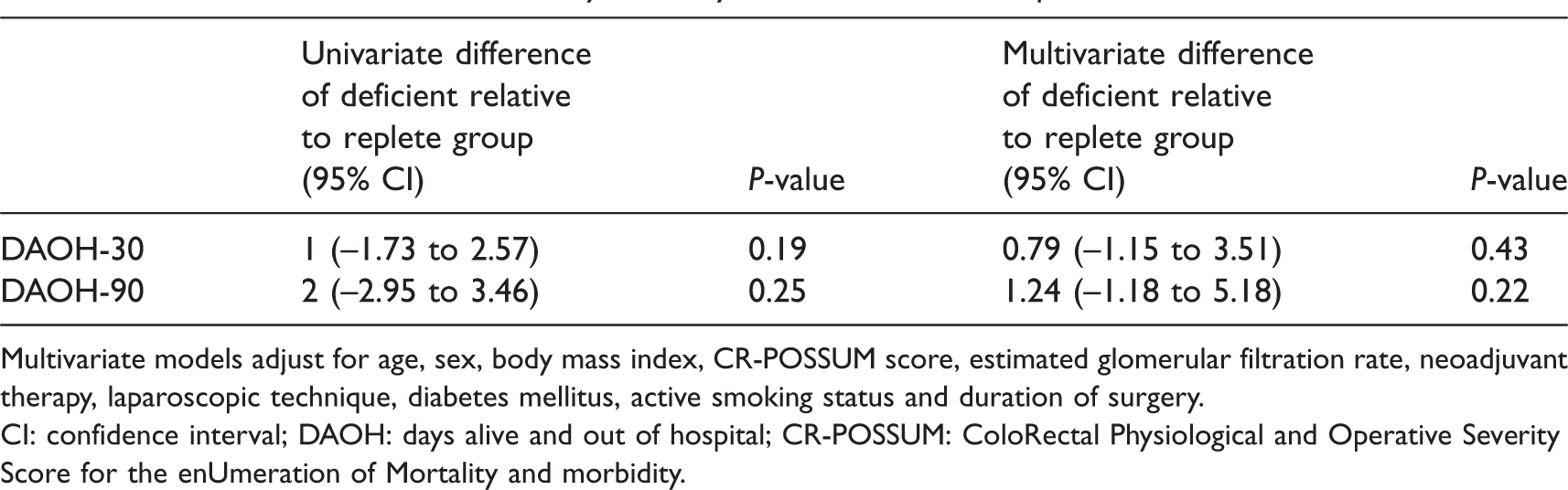
Multivariate models adjust for age, sex, body mass index, CR-POSSUM score, estimated glomerular filtration rate, neoadjuvant therapy, laparoscopic technique, diabetes mellitus, active smoking status and duration of surgery.
CI: confidence interval; DAOH: days alive and out of hospital; CR-POSSUM: ColoRectal Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity.
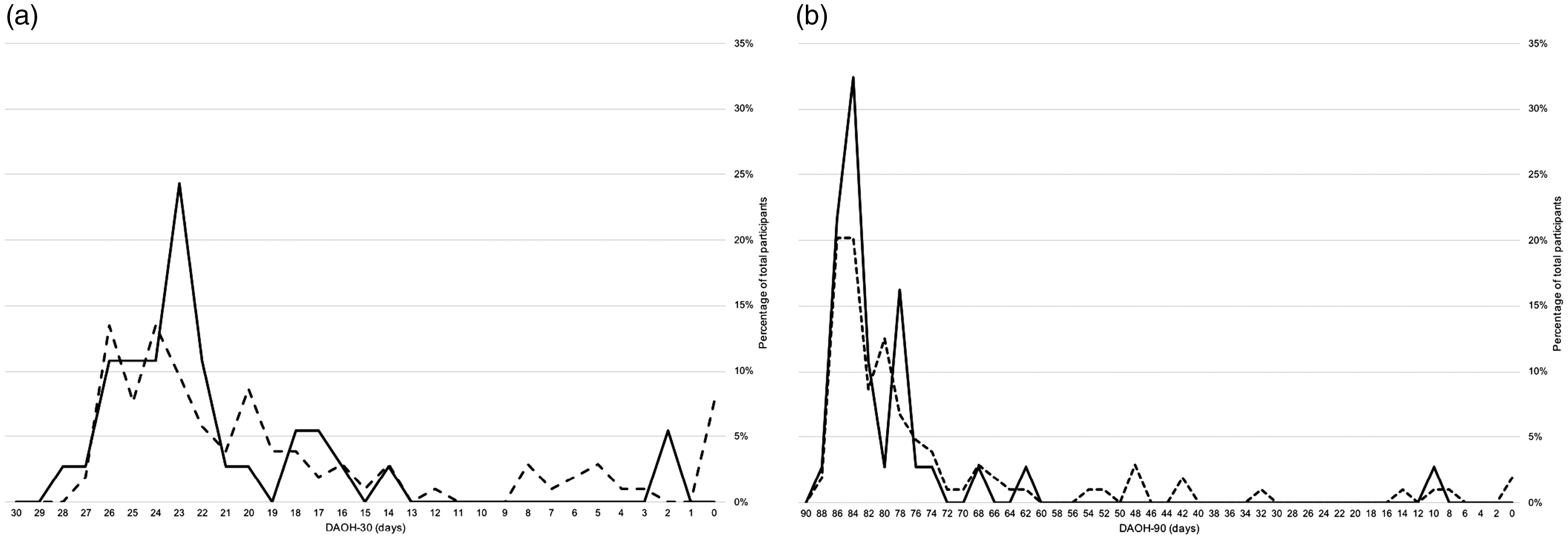
Frequency (%) of (a) DAOH-30 and (b) DAOH-90 across the two study groups. Dashed line, deficient group; solid line, replete group.
Given our results, we suggest conducting an adequately powered prospective study to quantify associations between non-anaemic iron deficiency and postoperative outcome. We suggest DAOH-90 as the primary outcome measure, with acute-care re-admission and all-cause infection as secondary outcome measures. The frequency of re-admission after day 30 suggests that hospital length of stay and 30-day metrics may be inadequate. We estimate a total of 400 evaluable participants would generate 83% power to detect a decrease in the median DAOH-90 from 83 to 81 days. Furthermore, we estimate that the screening of approximately 1000 patients undergoing major or complex resection of colorectal malignancy would be required to identify the requisite cohort. Such cohort work will then inform possible future intervention studies including preoperative iron therapy for patients who are not anaemic but are iron deficient.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Anaesthesia, Perioperative and Pain Medicine Unit of the Melbourne Medical School, University of Melbourne.