
Abstract

High flow nasal oxygen (HFNO) has been utilised in the intensive care setting for over 15 years. Its use in anaesthesia is rapidly increasing, providing an alternative to low flow oxygen devices during sedation for procedures such as bronchoscopy and gastroenterology as well as a potential role in non-invasive cardiological, radiological, emergency medicine and persistent pain procedures.1–3 The main advantages of heated and humidified HFNO are improved maintenance of adequate oxygenation with less drying of the upper airway mucosa, thereby improving patient comfort. However, one outstanding question is the role of wave-form capnography during patient sedation when HFNO is administered.
Maintaining patient safety while successfully completing the procedures under sedation, especially complex endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasound, requires careful titration of sedation ranging from moderate to deep sedation. The level of sedation may be difficult to predict, with a wide range of procedural difficulty, level of gastroenterologist and anaesthetist expertise as well as patient age and co morbidities. The use of HFNO in the gastroenterological suite may reduce critical incidents by providing high-inspired oxygen and slowing carbon dioxide rises related to respiratory depression. Currently, capnography is not available during HFNO usage and future development is required in this area before HFNO is acceptable for widespread use.
The need for routine capnography during sedation has been addressed by the Australian and New Zealand College of Anaesthetists (ANZCA) Guidelines on Monitoring During Anaesthesia. 4 These state that “a monitor of the carbon dioxide level in inhaled and exhaled gases…should be immediately available for any patient undergoing sedation”. In addition, the background document includes the following: “For sedation techniques that do not require airway instrumentation capnography is optional and should be determined by the patient’s clinical requirement and depth of sedation, and not the availability (or lack thereof) of suitable equipment”. 5
In contrast, the Association of Anaesthetists of Great Britain & Ireland (AAGBI) Standards of Monitoring require an “end-tidal carbon dioxide monitor if the patient is sedated” in locations outside the operating theatre. 6 The AAGBI Safety Statement for the use of capnography outside the operating theatre states “Continuous capnography should be used for all patients undergoing moderate or deep sedation”. 7
The American Society of Anesthesiologists Standards for Basic Anesthetic Monitoring include the following “During moderate or deep sedation the adequacy of ventilation shall be evaluated by continual observation of qualitative clinical signs and monitoring for the presence of exhaled carbon dioxide unless precluded or invalidated by the nature of the patient, procedure, or equipment”. 8 The United States of America Joint Commission on the Accreditation of Healthcare Organizations recommends capnographic monitoring of respiration during procedural sedation for elective ERCP to improve patient safety. 9
Guidelines to the Practice of Anesthesia prepared by the Canadian Anesthesiologists’ Society (CAS) require “capnography … to assess the adequacy of ventilation for moderate or deep procedural sedation”. 10
Based on the recommendations of these international authorities, it is recommended that wave form capnography is a highly desirable monitor during sedation during HFNO. Unfortunately, it would be expected that the high oxygen flow rates during HFNO would severely dilute expired carbon dioxide and make sampling impossible.
The author has in fact successfully used the following method of sampling carbon dioxide during gastroscopy when a bite block is being used. Figure 1a shows the use of a 14G cannula (Becton Dickinson Infusion Therapy Systems Inc., Sandy, UT, USA) placed in the oxygen inlet of an Oxyguard™ bite block (Endo-Technik Inc., Solingen, Germany). A hydrophobic disc filter (Flexicare Medical Inc., Irvine, CA, USA) has been attached to the cannula to protect the carbon dioxide sampling line from contamination. Figure 1b shows the small amplitude capnography waveform seen during HFNO when 60 L/min is being used. (Note: patient has given written consent for this photography to be used for publication). Future studies should explore the validity of this method and consideration of a purpose-built HFNO cannula for sampling end-tidal carbon dioxide.
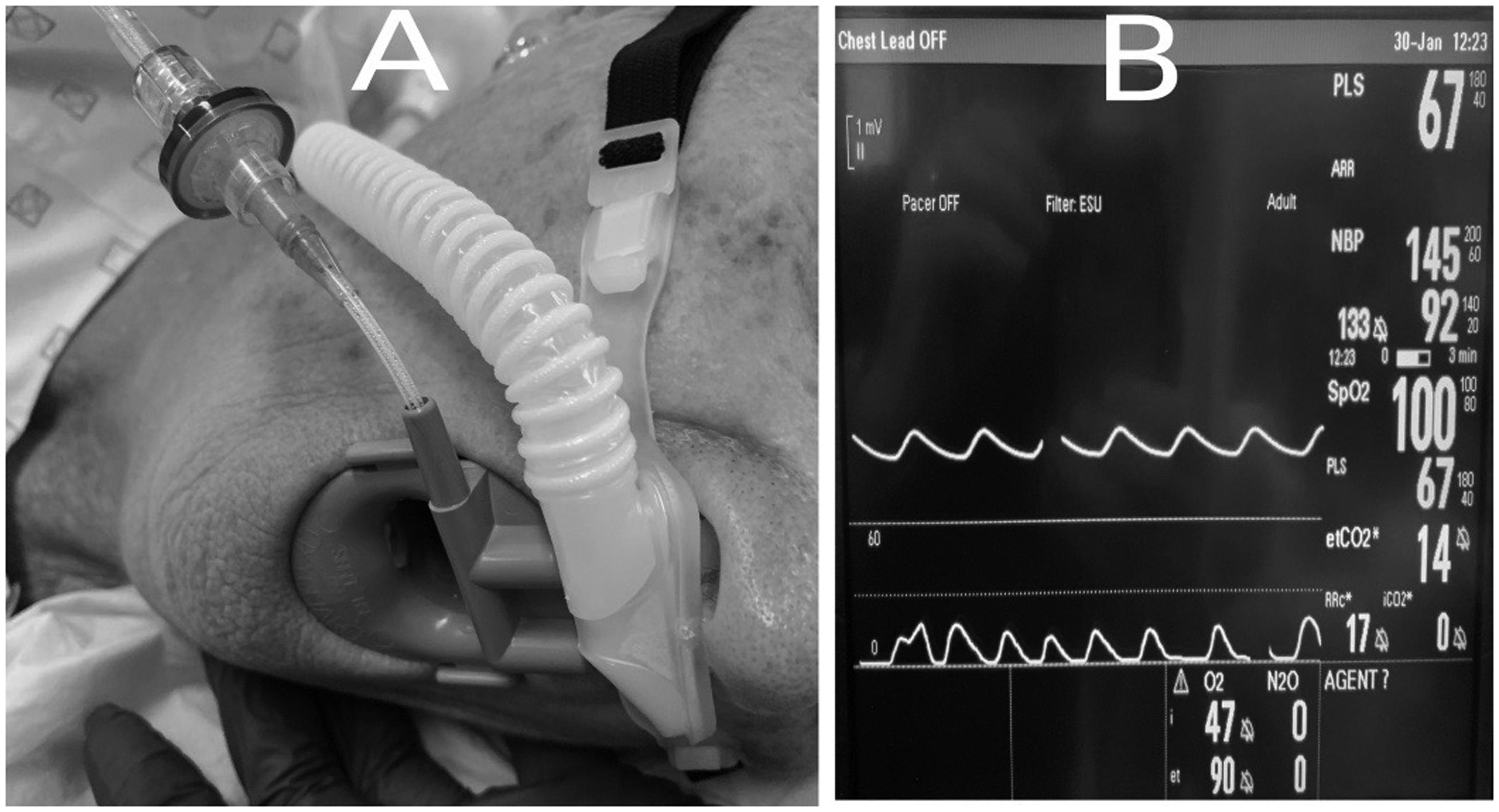
(a) End-tidal carbon dioxide sampling line with filter attached to 14G cannula which has been inserted into oxygen inlet of a bite block during HFNO administration. (b) Low amplitude waveform capnography occurring during HFNO at 60 L/min.
While this method of measuring end-tidal carbon dioxide may be used when HFNO is being administered, clinical observation by a vigilant anaesthetist remains paramount for patient safety. Loss of the capnograph waveform may indicate a number of potential issues such as upper airway obstruction, respiratory depression due to sedative drugs or blockage of the sampling line or filter.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.