
Abstract
Modern near-infrared spectroscopy technology is increasingly adopted to measure cerebral tissue oxygen saturation. However, the normal range of cerebral tissue oxygen saturation in adults with such technology is unknown. We sought to measure cerebral tissue oxygen saturation in healthy volunteers using the novel O3 Regional Oximetry® device (Masimo Corporation, Irvine, CA, USA) and assess its relationship with key physical and haemodynamic characteristics. For ≥5 minutes, we continuously recorded cerebral tissue oxygen saturation, pulse oximetry, cardiac index and mean arterial pressure. We assessed for differences in cerebral tissue oxygen saturation between hemispheres, sex, skin type, comorbidity or smoking status, and for associations between cerebral tissue oxygen saturation and age, height, weight, SpO2and haemodynamic parameters. We recorded >32,000 observations in 98 volunteers aged 22 to 60 years, including 41 (42%) males. One-fifth had one or more co morbidities (n=22, 22.5%), one-tenth were either current or former-smokers (n=13, 13%), and most had a Fitzpatrick skin type of 3 or lower (n=84, 86%). The mean combined average cerebral tissue oxygen saturation was 67.6% (95% confidence interval 66.8%–68.6%). We found statistically significant differences in cerebral tissue oxygen saturation according to hemisphere and an association between cerebral tissue oxygen saturation and mean arterial pressure and cardiac index. The combined average cerebral tissue oxygen saturation in 98 healthy volunteers was 67.6% with a narrow confidence interval and no combined average cerebral tissue oxygen saturation was below 56%. We also observed statistically significant yet quantitatively small cerebral tissue oxygen saturation differences between hemispheres, and an association between cerebral tissue oxygen saturation and mean arterial pressure and cardiac index.
Keywords
Introduction
There is growing interest in the measurement of regional cerebral tissue oxygen saturation (SctO2) through near-infrared spectroscopy (NIRS) technology.1–3Using adhesive sensors applied to each side of the forehead, NIRS analyses the relative absorbance of oxyhaemoglobin and deoxyhaemoglobin in the microcirculation of left and right frontal lobe cerebral tissue.4Tissues in this region are susceptible to ischaemia, therefore NIRS provides a contemporaneous estimation of the balance between regional cerebral oxygen supply and demand. The microcirculation of such tissue is non-pulsatile and is measured during cardiopulmonary bypass5,6and in deceased patients.7SctO2is a derived value and depends on the degree to which the arterial and venous blood contribute to the microcirculation.8Manufacturers use different processing algorithms, therefore SctO2values are not considered to be interchangeable between devices.9,10Subsequently, SctO2levels are typically compared to the patient’s baseline reading or reference values, with changes in cerebral tissue oxygen saturation to <80% of baseline or lower than 50% (absolute) associated with an increased incidence of post-operative cognitive dysfunction,11,12stroke13and other measures of morbidity.6However, normative values for clinical devices are essential to allow for definition of abnormality during clinical use. Moreover, available reference values have important limitations. In particular, they depend upon SctO2changes in individual patients11,12and are related to ‘normative’ values from intensive care unit (ICU) patients,14those awaiting cardiac or vascular surgery,1,15,16or are obtained with older technology in small cohorts.17,18Furthermore, such values do not take into account variables that might affect them such as hemisphere, sex, comorbidity and smoking status, skin type, height, weight, cardiac index, mean arterial pressure and other key haemodynamic parameters.
Accordingly, we aimed to measure SctO2using the Masimo O3-Regional Oximeter (O3-RO®, Masimo Corporation, Irvine, CA, USA) device in healthy adults and to assess for differences in SctO2between hemispheres, sex and comorbidity and smoking status, and for associations between SctO2and key physical, demographic and haemodynamic parameters.
Materials and methods
Study design and ethics
Human research ethics committee (HREC) approval (HREC no. LNR/15/Austin/468) was granted for a prospective observational study of healthy adult volunteers in a large teaching hospital.
Study participants
According to HREC instructions, an e-flyer was distributed via email inviting ICU staff to consider participation. Those who volunteered presented for participation where verbal and written information was provided. If satisfied, written informed consent was obtained and the option of withdrawal of consent was provided via a pre-printed withdrawal of consent document. Participants were included if they were aged 20 to 60 years and did not have pre-existing neurological disease or any disease that affected their cardiorespiratory function.
Technology
SctO2was recorded using the O3-RO®.19This was achieved through the placement of a disposable adhesive sensor to each side of the forehead. The sensor contains one light source and two photodetectors: intracranial and extracranial. Infrared light is emitted and reflected towards both detectors. The intracranial detector measures the haemoglobin oxygen saturation in the outer frontal cerebral cortex at a depth of 20 mm. The shallower extracranial detector measures superficial tissues that may be affected by photon scatter as a result of extracerebellar tissue reflections, significant variations in pigmentation and brain water content.20,21
Haemodynamic parameters were recorded with the recently Food and Drug Administration (FDA) approved ClearSight™ device22(Edwards Lifesciences, Irvine, CA) for the continuous non-invasive measurement of cardiac output23–25and mean arterial pressure.25,26
Data collection
Each volunteer provided information regarding demographics, co morbidities, over-the-counter medication use and smoking status. We continuously recorded data in a quiet environment with the participant sitting for a minimum of five minutes.
Study outcomes
The primary outcome of the study was measurement of the SctO2in healthy adult volunteers.
Secondary outcomes included assessing for differences in SctO2between hemispheres, sex, skin type, comorbidity and smoking status. Additional secondary outcomes assessed for associations between SctO2and age, sex, skin type, smoking status and key haemodynamic parameters.
Data analysis
Over a ≥5-minute period for each volunteer, the O3-RO® and ClearSight™ devices recorded data at 2- and 20-second intervals respectively. During data cleaning, data were inspected and range checks were performed. Frequency distributions were assessed through visual inspection of the shape of histograms for quantitative variables and consistency checks were performed for categorical variables. Data collected were correlated time-series and were analysed as such. Descriptive data for continuous variables were summarised as correlated time-series. The intra- and inter-patient correlated times-series data were further assessed for normality using the Skewness and Kurtosis test with Bootstrapping. Associations between continuous variables and dichotomised variables were assessed using correlated time-series linear regression. The differences between continuous variables were assessed using correlated time-series mixed models. The magnitude of difference within each participant’s recorded SctO2was assessed. For each participant, a combined average SctO2was calculated (left SctO2 + right SctO2/2). The height and weight of volunteers were entered into the ClearSight™, which calculated the body surface area (DuBois Formula: surface area (m2) = 0.007184 × height (cm)0.725 × weight (kg)0.425).27The systemic vascular resistance (SVR, dynes/s cm5) and SVR index (dynes/s cm5/m2) were estimated using a right atrial pressure of 0 mmHg. Skin type was recorded using the Fitzpatrick Scale.28Continuous variables were expressed as mean standard deviation (SD) with 95% confidence intervals whereas categorical values were expressed as number (n) and percentage (%). Categorical skin type, comorbidity and smoking status data were each dichotomised as skin type: three or lower versus four or more; comorbidity: present versus absent; and smoking status: never versus current or former. The frequency distribution of SctO2values was normal, therefore assessment of the differences between SctO2and dichotomous variables was performed using the Student’s t-test. Statistical analysis was undertaken with Stata 14® (Stata Corporation, College Station, TX, USA) and a two-sided p-value of <0.05 was taken to indicate statistical significance.
Results
Physical and demographic data
We recorded 32,130 cerebral tissue oxygen saturation observations in 98 healthy volunteers, aged 22 to 60 years, 41 (42%) male. One-fifth had one or more co morbidities (n = 22, 22.5%), one in 10 were either current or former-smokers (n = 13, 13%) and most had light skin (Fitzpatrick skin type of 3 or lower, n = 84, 86%) (Table 1, Electronic Supplementary Material 1). The range of the difference in SctO2values recorded within each participant was 1% to 10%, with a median of 2.5% (interquartile range 2% to 3%). Skewness and Kurtosis assessment for normality in the intra-individual and inter-individual SctO2values were both non-significant in left (p = 0.41, p = 0.23) and right (p = 0.08, p = 0.48) hemispheres respectively (Electronic Supplementary Material 2).
Participant characteristics, n = 98.
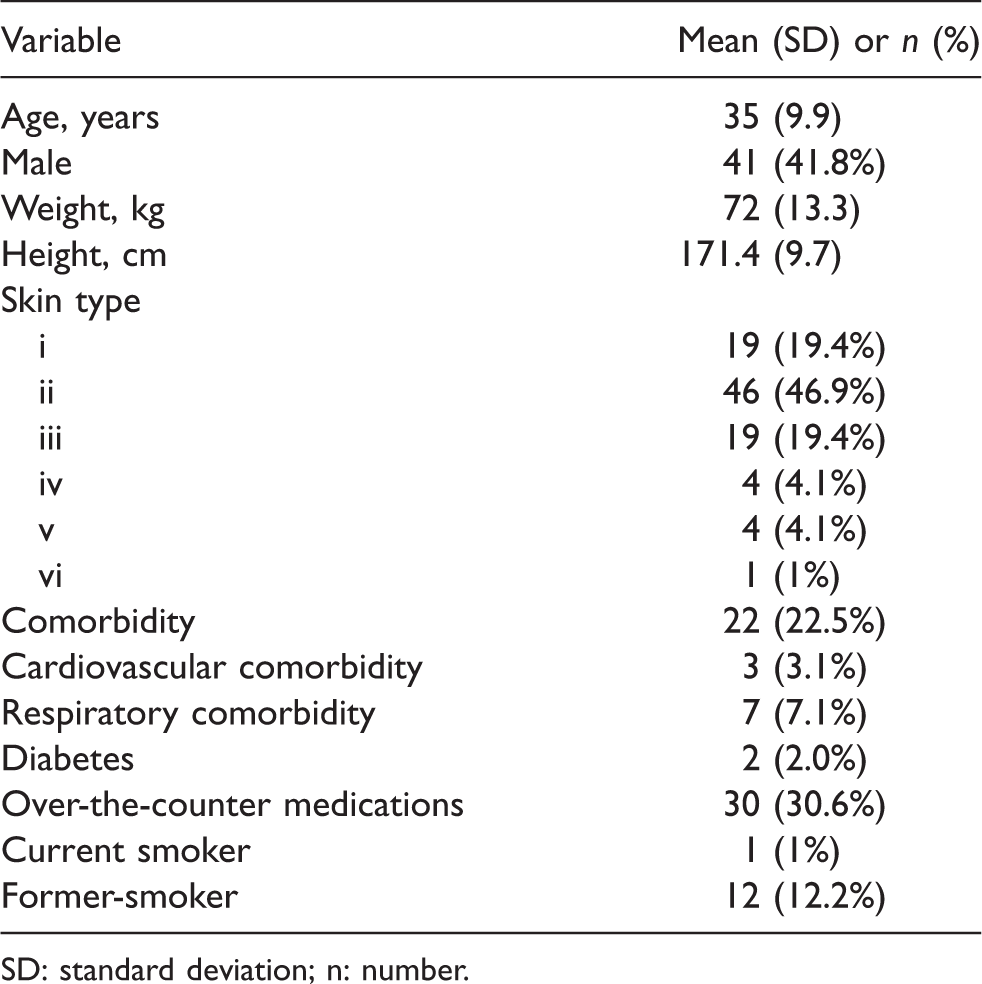
SD: standard deviation; n: number.
SctO2,haemodynamic and peripheral oxygenation measurement
The mean left, right and combined average SctO2were 67.3%, 67.9% and 67.6%, respectively and each approximated a normal distribution. None of the 95% confidence intervals were lower than 66.5% or greater than 69.1% for any of the left, right or combined average SctO2(66.5% to 68.4%, 66.8% to 69.1% and 66.8% to 68.6%, respectively). To one single whole number, the lowest observed SctO2among participants was 50% for the right, 57% for the left and 56% for the combined value. The mean SpO2, blood pressure, heart rate and other haemodynamic parameters were all within normal values and are presented in Table 2.
Mean cerebral oximetry and haemodynamic baseline values.
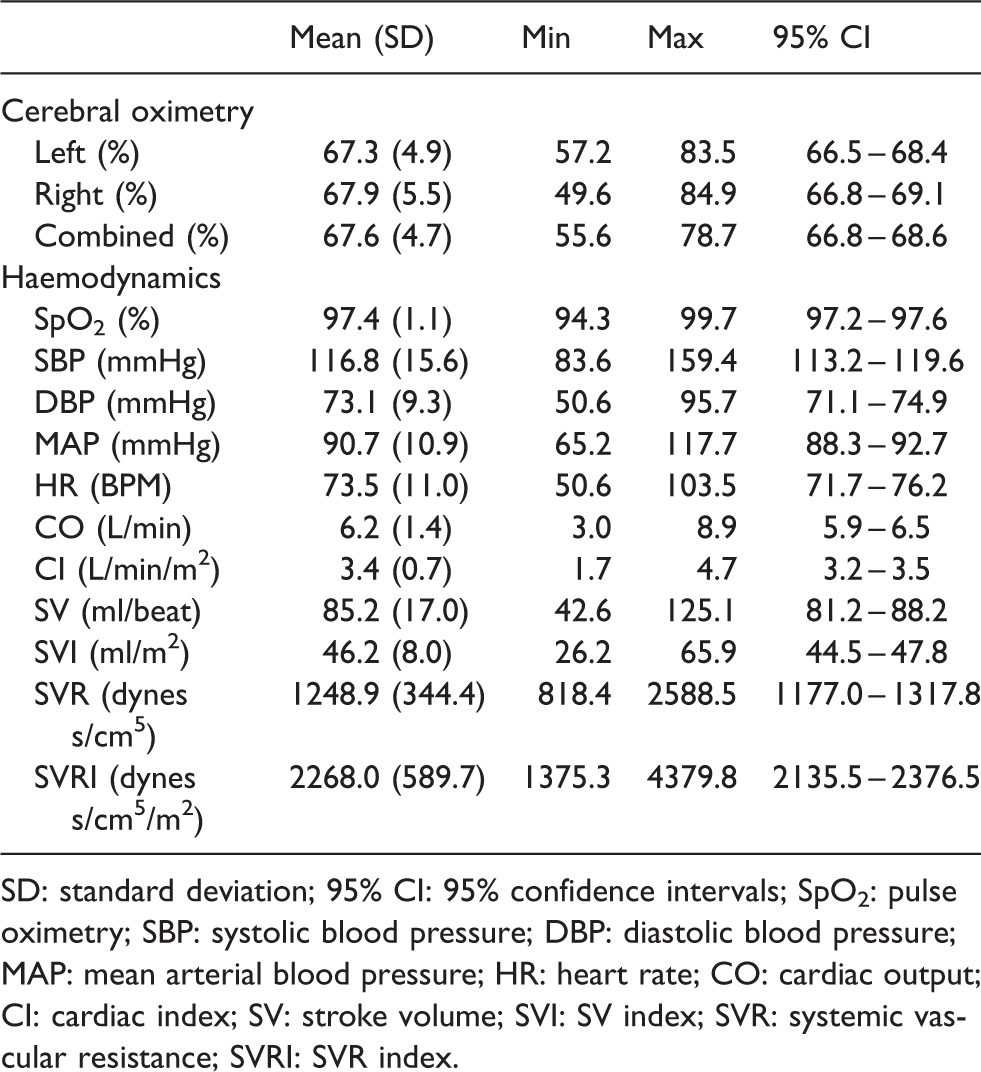
SD: standard deviation; 95% CI: 95% confidence intervals; SpO2: pulse oximetry; SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean arterial blood pressure; HR: heart rate; CO: cardiac output; CI: cardiac index; SV: stroke volume; SVI: SV index; SVR: systemic vascular resistance; SVRI: SVR index.
Differences between SctO2and dichotomous variables
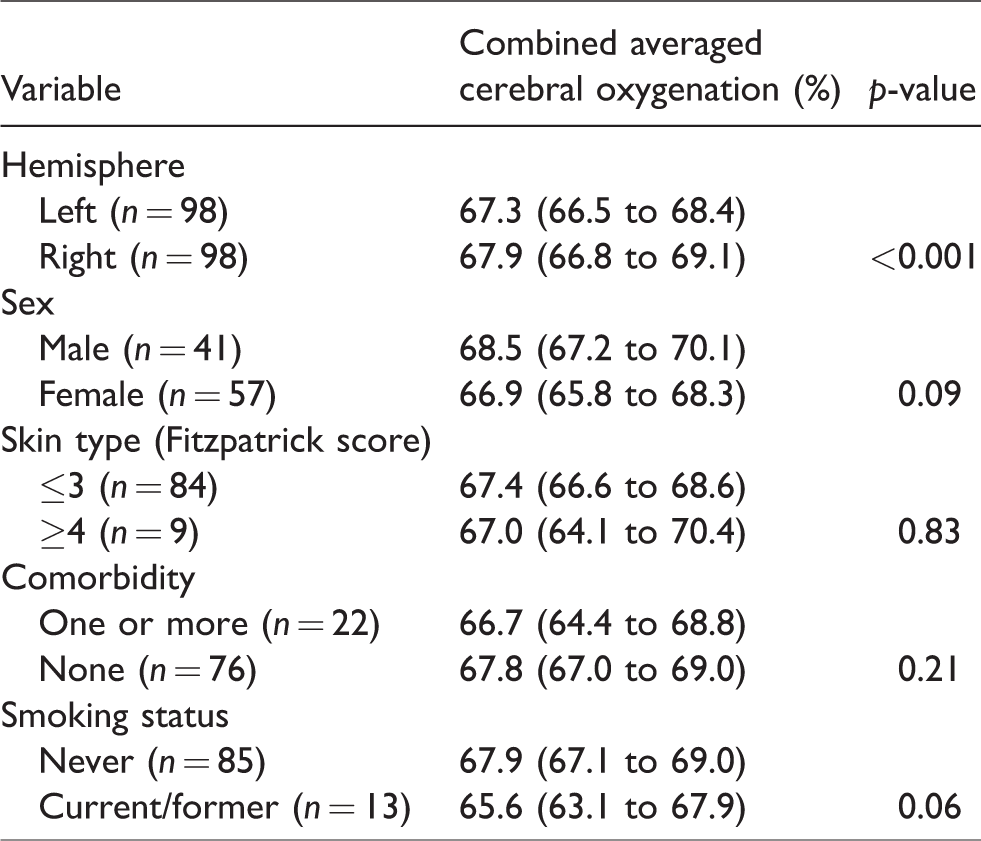
There was a difference between hemispheres (p < 0.001) and no further statistically significant differences in SctO2according to sex (p = 0.09), skin type (p = 0.83), comorbidity (p = 0.21) or smoking status (p = 0.06) (Table 3).
Differences between combined cerebral oximetry and dichotomous variables presented as mean (95% confidence interval).
Association between SctO2and continuous variables
On univariable linear regression analysis, increasing mean arterial pressure (MAP) (p = 0.001) and cardiac index (CI) (p = <0.001) were associated with an increased SctO2. Each 10 mmHg increase in MAP and 1 L/min/m2increase in CI was associated with a 0.01% and 0.1% increase in SctO2, respectively. However, there was no association between SctO2and darker skin (p = 0.84), current or former-smokers (p = 0.06) and male sex (p = 0.10) (Electronic Supplementary Material 3). The associations between MAP and CI and SctO2were maintained in multivariate regression analysis (Electronic Supplementary Material 4).
Discussion
Key findings
In a large cohort of healthy adults, we found a mean combined average SctO2of approximately 68% with narrow confidence intervals of approximately 1%. Moreover, no combined average SctO2was below 56%. Finally, we observed statistically significant yet quantitatively small differences between hemispheres, and an association between SctO2and MAP and CI, respectively.
Relationship to previous studies
Data presented in a 2017 systematic review of 11 randomised controlled trials using NIRS technology across a range of devices in pre-operative cardiac surgery patients described a near identical baseline and reference range SctO2of 66.4% and 51%–82%, respectively.29Despite concerns regarding the differences between measurement devices, this comprehensive study noted ‘considerable statistical heterogeneity’ among those analysed. However, this baseline data refers to those awaiting cardiac surgery and as such, they are not healthy adults. The first study of SctO2, a 1998 prospective study of 93 healthy people by Misra et al., found a similar SctO2of 67.1% (SD 8.8%, 95% confidence intervals 65.3%, 68.9%),20with a range of 48%–79%, and a 3.7% difference between hemispheres (p = 0.044). However, this study utilised outdated technology (INVOS 3110A™, Somanetics Corporation, Troy, MI, USA), performed fewer right hemisphere SctO2measurements, included predominantly females (69%) and did not present demographics or medical history details. A 2004, prospective observational study in 1000 patients scheduled to undergo cardiac surgery using the INVOS 4100/5100c™ devices (Somanetics Corporation, Troy, MI, USA) reported a mean SctO2of 67% (SD 10%, 95% confidence intervals 66.4%, 67.6%).1Of interest, 5.4%, 1.6% and 1.5% of patients recorded a baseline SctO2of <50%, <40% or >85%, respectively. However, these were patients awaiting coronary artery bypass grafting, or aortic or mitral valve replacement, with an age range up to 91 years. Furthermore, no details regarding premedication and oxygenation were provided. In 2000, Kim and colleagues prospectively measured SctO2in 42 healthy subjects aged 20–36 years using the INVOS 4100™ (Somanetics Corporation, Troy, MI, USA) device and found a higher mean SctO2of 70.7% (SD 6.1%, 95% confidence intervals 68.9%, 72.5%).17However, only the right hemisphere SctO2was recorded, invasive lines (arterial, jugular bulb) were inserted and participants were made to breathe through an occlusive facemask. Furthermore, the signal processing algorithm was altered by the manufacturer part-way through the study. A 2015 prospective observational study using the INVOS 5100C™ device (Covidien, Dublin, Ireland) by Valencia et al.30in 50 patients undergoing minor surgery described a lower SctO2of 62.0% (SD 10.4%, 95% confidence intervals 59.1%, 64.9%) with a wide range of SctO2values (30%–92%), differences between sex (67.6% male, 60.0% female, p = 0.023) and associations between SctO2and body weight (p = 0.014), height (p = 0.014), American Society of Anesthesiologists (ASA). Physical status (p = 0.045) and chronic renal failure (p = 0.005). However, this study did not involve healthy individuals but patients presenting for hernia repair or mastectomy for malignancy (including eight patients (16%) with severe systemic disease and substantive functional limitations), had a small sample size (n = 50) and was predominately comprised of women (72%).
Implications for clinicians
Our study implies that in healthy adults the mean SctO2measured with modern technology is close to 68% with narrow confidence intervals of 1%, and with no difference between hemispheres. Moreover, given a lowest mean combined bi-hemispheric SctO2value of 56%, it implies that an SctO2value below 56% should be considered ‘abnormally low’. In addition, the very few SctO2values below 60% seen in our study imply that persistent measurements below such a threshold should be viewed with concern. Finally, our observation that SctO2values were not affected in any clinically significant amount by hemispheres, sex, skin type, comorbidity or smoking status, age or any haemodynamic parameter implies that in healthy adults, cerebral tissue oxygen saturation in unaffected by these factors.
Strengths and limitations
To our knowledge, this is the first time that SctO2has been measured in a large cohort of healthy adults using modern technology with simultaneous, continuous measurement of cardiac output and blood pressure, thus enabling the assessment of the impact of these as well as other key factors on SctO2. The normal distribution observed, the tight 95% confidence intervals and the lack of difference or associations with other factors imply a degree of face validity, concurrent validity, construct validity and content validity for our observations. The sample size was the largest cohort of healthy adults ever tested. Due to the quantity of recorded data points from the SctO2monitoring device, we describe statistically significant associations between SctO2and continuous variables. However, the absolute changes in SctO2in most variables are quantitively small and of minimal clinical consequence. The O3-RO® used more advanced and updated NIRS technology to measure arterial and venous signals to produce a SctO2value. The O3-RO® signal can be affected by sensor site and placement.31However, cerebral tissue oxygen saturation has been validated in several studies14,17,19,32and SctO2measurement continues to be of interest in current research.29,33The ClearSight™ estimates cardiac output using volume-clamp pulse-contour technology, which relies upon assumptions regarding the individual’s aortic impedance.34–36However, this device has been validated against alternatives in several articles23,24,37–39and is now FDA approved for such measurements. Healthy adults over the age of 60 years were excluded, which limits the applicability of this information for persons in this age group. Future studies of those in well patients in the older age range are warranted. The interpretation of appropriate SctO2values and the subsequent management of changes in SctO2is the topic of several interventional studies.3,18,40,41However, such interpretation is affected by knowledge of normative values, thus providing reference values for SctO2is of diagnostic and therapeutic relevance.
Conclusions
In summary, we performed a prospective observational study in 98 healthy adults to measure SctO2. We identified a mean combined average SctO2of 67.6% with tight confidence intervals of 66.8% to 68.8%, and a normal distribution, and no combined average SctO2value was below 56%. Finally, we observed statistically significant yet quantitatively small differences between hemispheres and an association between SctO2and CI and MAP, respectively. These findings have significant implications regarding the clinical interpretation of SctO2and the application of this information to individual patients.
Supplemental Material
Supplemental Material1 - Supplemental material for Modern technology–derived normative values for cerebral tissue oxygen saturation in adults
Supplemental material, Supplemental Material1 for Modern technology–derived normative values for cerebral tissue oxygen saturation in adults by Christopher T Eyeington, Paolo Ancona, Eduardo A Osawa, Salvatore L Cutuli, Glenn M Eastwood and Rinaldo Bellomo in Anaesthesia and Intensive Care
Supplemental Material
Supplemental Material2 - Supplemental material for Modern technology–derived normative values for cerebral tissue oxygen saturation in adults
Supplemental material, Supplemental Material2 for Modern technology–derived normative values for cerebral tissue oxygen saturation in adults by Christopher T Eyeington, Paolo Ancona, Eduardo A Osawa, Salvatore L Cutuli, Glenn M Eastwood and Rinaldo Bellomo in Anaesthesia and Intensive Care
Supplemental Material
Supplemental Material3 - Supplemental material for Modern technology–derived normative values for cerebral tissue oxygen saturation in adults
Supplemental material, Supplemental Material3 for Modern technology–derived normative values for cerebral tissue oxygen saturation in adults by Christopher T Eyeington, Paolo Ancona, Eduardo A Osawa, Salvatore L Cutuli, Glenn M Eastwood and Rinaldo Bellomo in Anaesthesia and Intensive Care
Supplemental Material
Supplemental Material4 - Supplemental material for Modern technology–derived normative values for cerebral tissue oxygen saturation in adults
Supplemental material, Supplemental Material4 for Modern technology–derived normative values for cerebral tissue oxygen saturation in adults by Christopher T Eyeington, Paolo Ancona, Eduardo A Osawa, Salvatore L Cutuli, Glenn M Eastwood and Rinaldo Bellomo in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
We would like to thank the volunteers from Austin Health ICU (nursing staff, secretarial staff, pharmacists, patient support staff and medical staff) for choosing to give their time for this study to be completed.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Information from this study was presented in part at the 2017 Australian and New Zealand Intensive Care Society Annual Scientific Meeting at the Gold Coast, Australia, on 12 October 2017. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by an unrestricted educational grant from the Austin Hospital Anaesthesia and Intensive Care Trust Fund. None of the authors or the institutions they work for have or are expected to receive any financial or other incentives from Masimo Corporation or Edwards Lifesciences. Neither Masimo Corporation nor Edwards Lifesciences were not involved in any stage of the study design, implementation, data analysis or manuscript preparation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.