
Abstract
Electrical cardioversion (ECV) is a potentially life-saving treatment for haemodynamically unstable new-onset atrial fibrillation (AF); however, its efficacy is unsatisfactory. We aimed to elucidate the factors associated with successful ECV and prognosis in patients with AF. This retrospective observational study was conducted in two mixed intensive care units (ICUs) in a university hospital. Patients with new-onset AF who received ECV in the ICU were enrolled. We defined an ECV session as consecutive shocks within 15 minutes. The success of ECV was evaluated five minutes after the session. We analysed the factors associated with successful ECV and ICU mortality. Eighty-five AF patients who received ECV were included. ECV was successful in 41 (48%) patients, and 11 patients (13%) maintained sinus rhythm until ICU discharge. A serum potassium level ≥3.8 mol/L was independently associated with successful ECV in multivariate analysis (odds ratio (OR), 3.13; 95% confidence interval (CI), 1.07–9.11; p = 0.04). Maintenance of sinus rhythm until ICU discharge was significantly associated with ICU survival (OR 9.35; 95% CI 1.02–85.78, p = 0.048). ECV was successful in 48% of patients with new-onset AF developed in the ICU. A serum potassium level ≥3.8 mol/L was independently associated with successful ECV, and sinus rhythm maintained until ICU discharge was independently associated with ICU survival. These results suggested that maintaining a high serum potassium level may be important when considering the effectiveness of ECV for AF in the ICU.
Background
Atrial fibrillation (AF) is the most common arrhythmia in critically ill patients, occurring in about 13% of patients admitted to medical or general intensive care units (ICUs). 1 AF reduces cardiac output and results in haemodynamic disturbances and is associated with increased mortality. 2 Chronic AF is associated with an increased risk of thrombotic complications, including stroke. These adverse consequences mean that AF is considered as an independent predictor of in-hospital mortality in critically ill patients.3–5
Treatment of new-onset AF involves rate and rhythm controls. Synchronised direct current electrical cardioversion (ECV) and/or antiarrhythmic drugs can be used for rhythm control. ECV aims to provide fast and effective conversion of AF to sinus rhythm (SR) 6 and was recently recommended for use in patients with severe haemodynamic failure due to new-onset AF. 7 ECV is successful in about 90% of outpatients with AF8,9 and in 71% of post-cardiac surgery patients. 10 However, the success rate in patients undergoing noncardiac surgery11,12 and the factors associated with successful ECV for new-onset AF in the noncardiac surgical ICU have been inadequately studied.
In this observational study, we investigated the demographics of critically ill patients with new-onset AF treated with ECV to clarify the success rate of ECV and identify the factors associated with successful ECV and mortality.
Methods
Study design and population
This retrospective observational study was performed in two mixed ICUs (emergency and medicosurgical ICUs) in Hiroshima University Hospital from January 2010 to September 2016. The study protocol was approved by the institutional review board of Hiroshima University (Trial registration: E-667, registered 31 January 2017). We reviewed medical charts, databases of bedside electrocardiograms (ECGs), and medical records for ICU patients and selected consecutive patients (age ≥18 years) with new-onset AF after ICU admission who received biphasic ECV for the first time. Patients with permanent pacemakers were excluded.
New-onset AF was defined as the first AF rhythm on ECG occurring during an ICU stay. AF rhythm was diagnosed by the attending physicians using either a bedside monitor (Philips, Tokyo, Japan) or 12-lead ECG. The usual indication for ECV was haemodynamically unstable AF patients, while the final decision to implement ECV was made by the attending ICU physicians. ECV was performed using a HeartStart XL® (Philips, Amsterdam, Netherlands), with the delivered energy during the ECV session determined by the ICU physicians. An ECV session was defined as consecutive shocks performed within 15 minutes.
Successful ECV was defined as conversion to SR for at least five minutes after an ECV session. Unsuccessful ECV was defined as sustained AF rhythm within five minutes after an ECV session.
Data collection
We collected demographic data for all the included patients, including age, sex, disease category, past history of AF and cardiac surgery, Acute Physiology and Chronic Health Evaluation (APACHE) II score upon ICU admission, and Sequential Organ Failure Assessment (SOFA) score at the onset of AF. We also recorded patient data including implementation of mechanical ventilation and renal replacement therapy, use of diuretics, presence of infection, and potential or modifiable risk factors or associated conditions including heart rate, blood pressure, body temperature, serum potassium and calcium level, arterial pH, white blood cell count, C-reactive protein level, concurrent use of inotropes and vasopressors at any dose (including norepinephrine, dopamine and dobutamine) and pre-ECV treatment with antiarrhythmic drugs including β-blockers, sodium channel blockers and amiodarone.
The delivered energy, number of shocks, time from the onset of AF until the first ECV, and success rates of ECV were recorded using the ACSYS patient data system (Philips, Tokyo, Japan) or a bedside ECG data storage system. The stability of SR and recurrence of AF until ICU discharge were retrospectively reviewed manually using the ACSYS patient data and ECG data storage systems. The clinical outcomes were the development of cerebral infarction, length of hospital and ICU stays, and mortality.
Statistical analysis
Values are given as median (interquartile range; IQR) or number (percentage), as appropriate. Categorical variables were compared between successful and unsuccessful ECV sessions using Fisher’s exact tests, and continuous variables were compared using Mann–Whitney U tests. The associations between characteristics and successful ECV and ICU mortality were assessed by multivariate logistic regression analysis with backward stepwise variable elimination. Factors with a p value ≤ 0.10 in univariate analyses and parameters previously reported to be associated with successful ECV such as age, APACHE II score, SOFA score, use of β-blockers and use of amiodarone were entered into the multivariate model. Regarding ICU death, factors with a p value ≤ 0.10 in univariate analyses, age, APACHE II score and SOFA score were entered into the multivariate model. Parameter thresholds (e.g. serum potassium level) were decided using receiver operating characteristic (ROC) curve analysis. A p value ≤ 0.05 was considered significant. All statistical analyses were carried out using JMP statistical software (version 13.0.0; SAS, Cary, NC, USA).
Results
Patient demographics
Eighty-five patients with new-onset AF were included during the study period. Their median age was 71 (IQR, 64–78) years, and there were 58 men (68%) (Table 1). The median APACHE II score on ICU admission and SOFA score at the onset of AF were 26 (IQR, 17–34) and 8 (IQR, 5–11), respectively (Table 1). Concomitant infection was present in 47 patients (55%), 13 patients (15%) were undergoing cardiac surgery, and 14 patients (16%) had a past history of AF. The duration of ICU stay was 16 (IQR, 9–25) days (Table 2) and the overall ICU mortality was 35%.
Patient characteristics and status at onset atrial fibrillation.
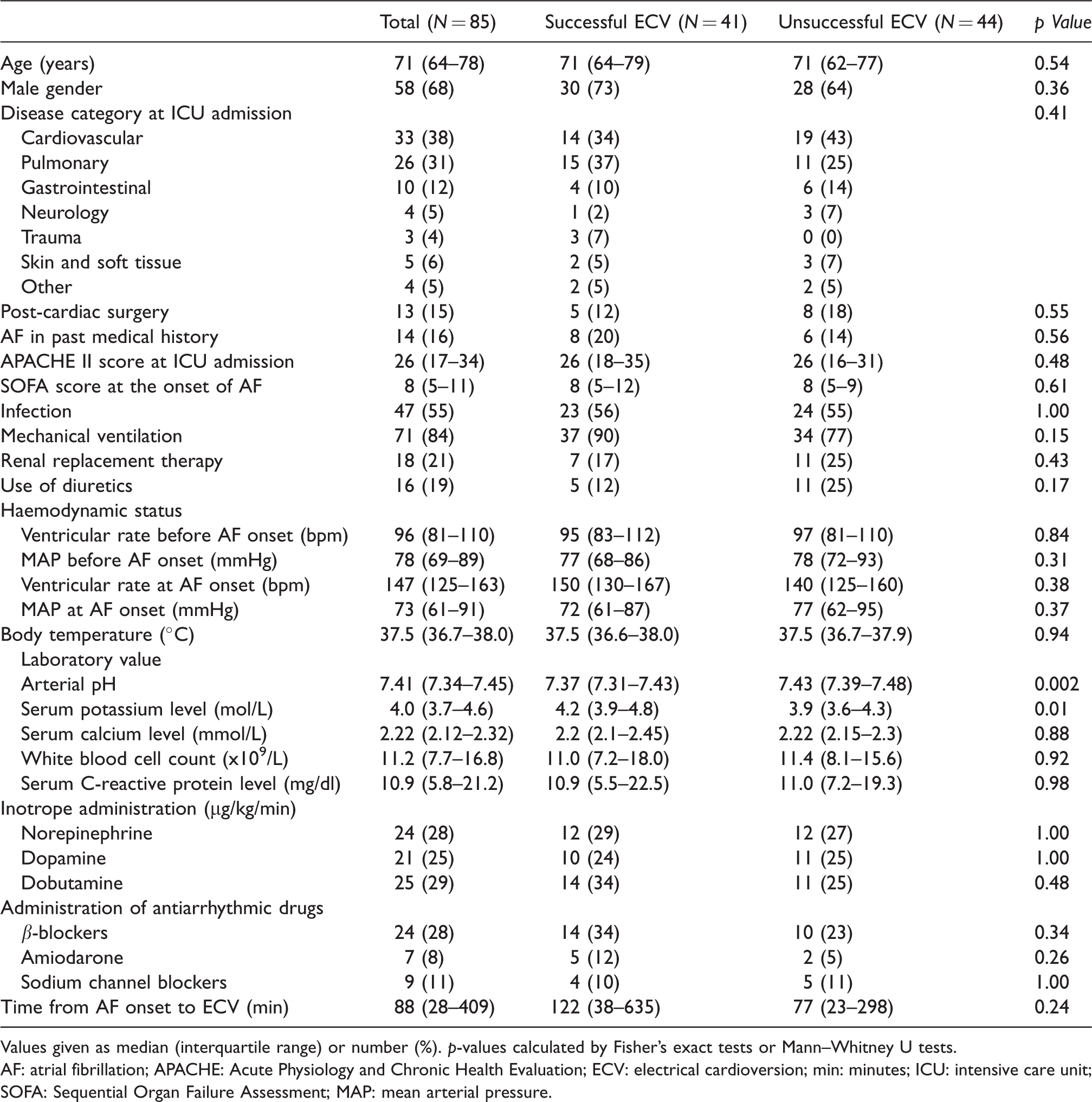
Values given as median (interquartile range) or number (%). p-values calculated by Fisher’s exact tests or Mann–Whitney U tests.
AF: atrial fibrillation; APACHE: Acute Physiology and Chronic Health Evaluation; ECV: electrical cardioversion; min: minutes; ICU: intensive care unit; SOFA: Sequential Organ Failure Assessment; MAP: mean arterial pressure.
Patient outcomes.
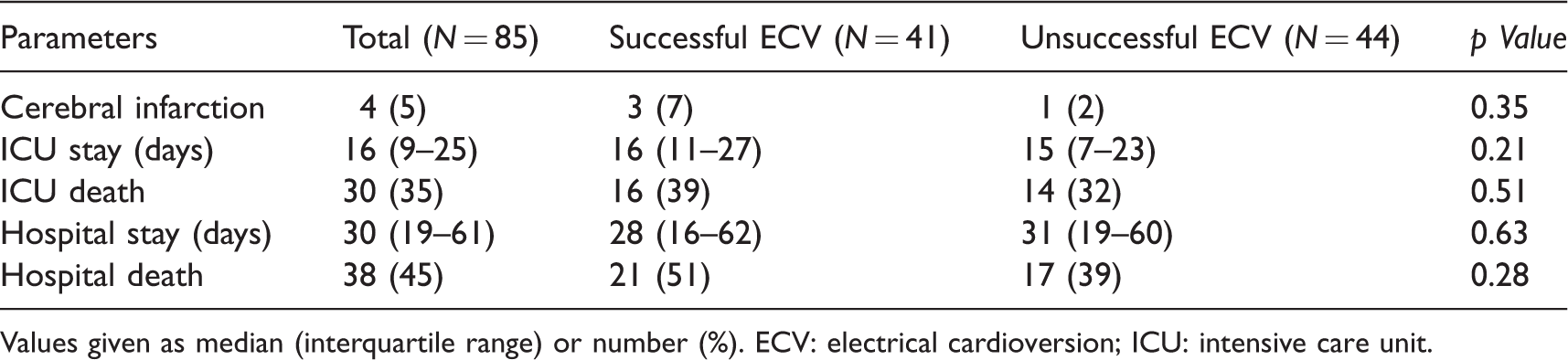
Values given as median (interquartile range) or number (%). ECV: electrical cardioversion; ICU: intensive care unit.
Success of ECV
ECV was successful in 41 (48%) patients (Figure 1), including 11 (13%) who maintained SR until ICU discharge and 30 (35%) who had recurrent AF. Among the 44 (52%) patients with unsuccessful ECV, seven (8%) did not return to SR until after ICU discharge, while 37 (44%) returned to SR during their ICU stay.
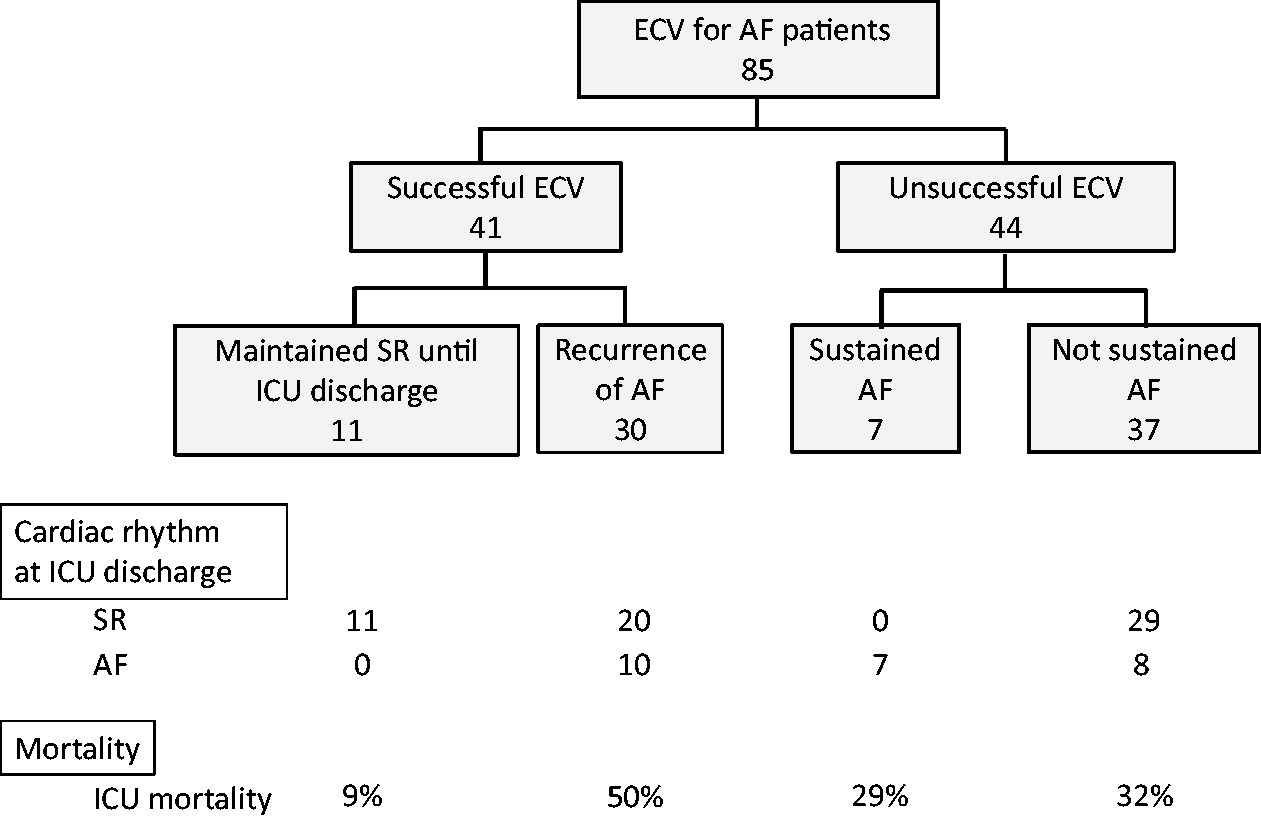
Diagram of new-onset AF patients who received ECV. AF: atrial fibrillation; ECV: electrical cardioversion; ICU: intensive care unit; SR: sinus rhythm.
Clinical practices of ECV
The 85 ECV sessions included 142 shocks, with a median of one (IQR, 1–2) shock per ECV session. Patients with successful ECV received fewer shocks than patients with unsuccessful ECV (1 versus 2; p = 0.00003). The distribution of numbers of ECVs is shown in Figure 2(a). The delivered ECV energies in the first and second shocks were ≤100 J in 91% and 83% of all ECV patients, respectively (Figure 2(b)).
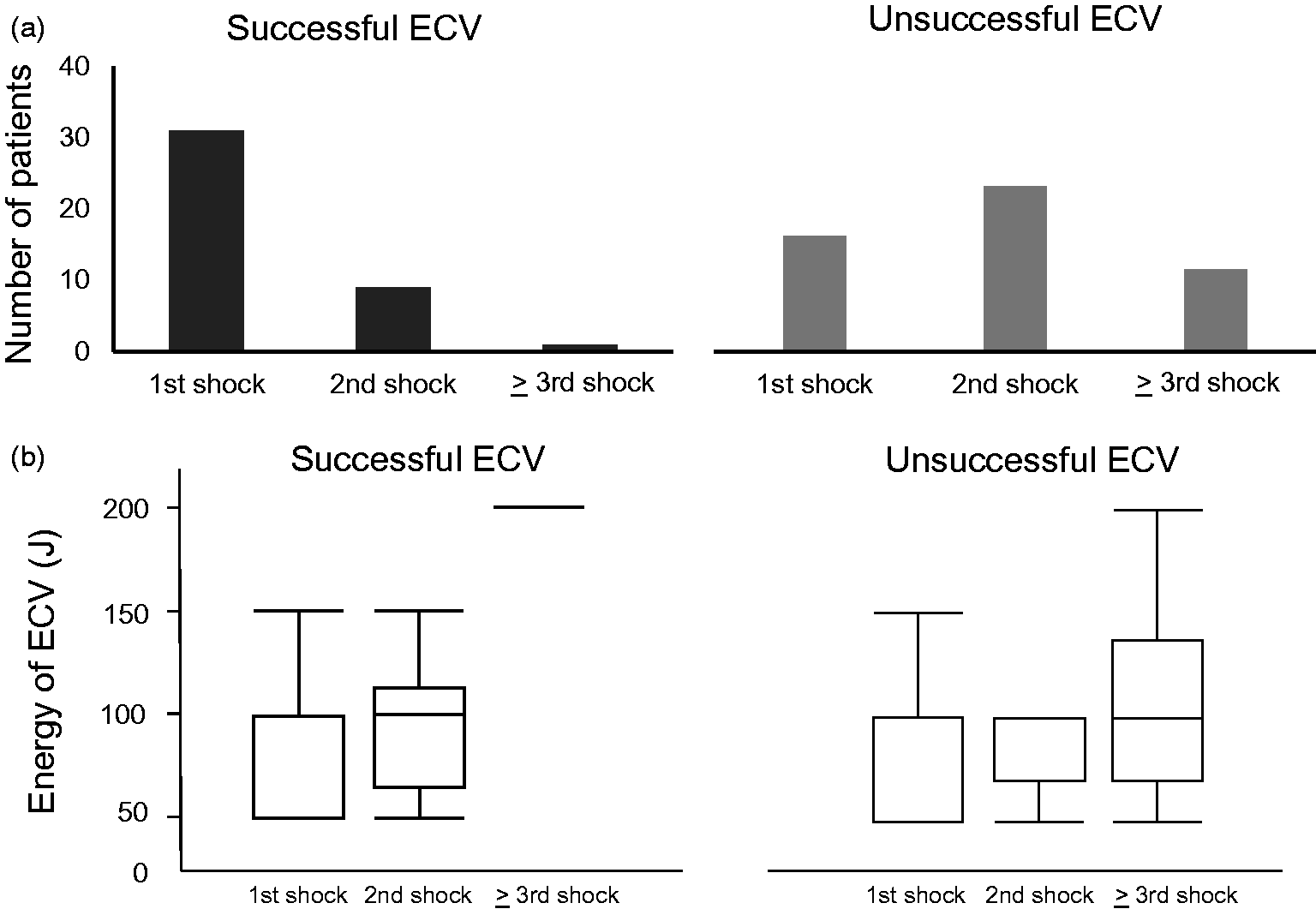
(a) Numbers of patients with successful and unsuccessful electrical cardioversion (ECV) undergoing various shock cycles. (b) Delivered energy in each shock cycle in patients with successful and unsuccessful ECV.
Comparison between successful and unsuccessful ECV
The baseline characteristics of patients with successful and unsuccessful ECV were similar (Table 1). However, arterial pH was significantly lower (7.37 versus 7.43; p = 0.002) and serum potassium level was significantly higher (4.2 versus 3.9 mol/L; p = 0.01) in patients with successful ECV compared with those with unsuccessful ECV.
The use of inotropes and antiarrhythmic drugs accompanied by ECV were similar in patients with successful and unsuccessful ECV. The occurrence of cerebral infarction, and ICU and hospital mortality were also similar in both groups (Table 2).
Factors associated with successful ECV
Based on the nearest point to 100% sensitivity and 100% specificity in the ROC curve analysis, the cutoff value for serum potassium level to detect successful ECV was 3.8 mol/L (e Figure 1). A serum potassium level ≥3.8 mol/L was associated with successful ECV in univariate analysis (odds ratio (OR), 4.05; 95% confidence interval (CI), 1.53–11.73; p = 0.004) (Table 3) and was also independently associated with successful ECV in multivariate analysis adjusted for arterial pH (OR, 3.13; 95% CI, 1.07 – 9.11; p = 0.04) (Table 3). In addition, higher arterial pH (per 0.1 increase) was associated with successful ECV in the univariate analysis (OR, 0.59; 95% CI, 0.37 – 0.94; p = 0.02), but it was not independently associated with successful ECV in the multivariate analysis (OR, 0.71; 95% CI, 0.43–1.17; p = 0.18).
Univariate and multivariate analyses of factors associated with successful ECV.
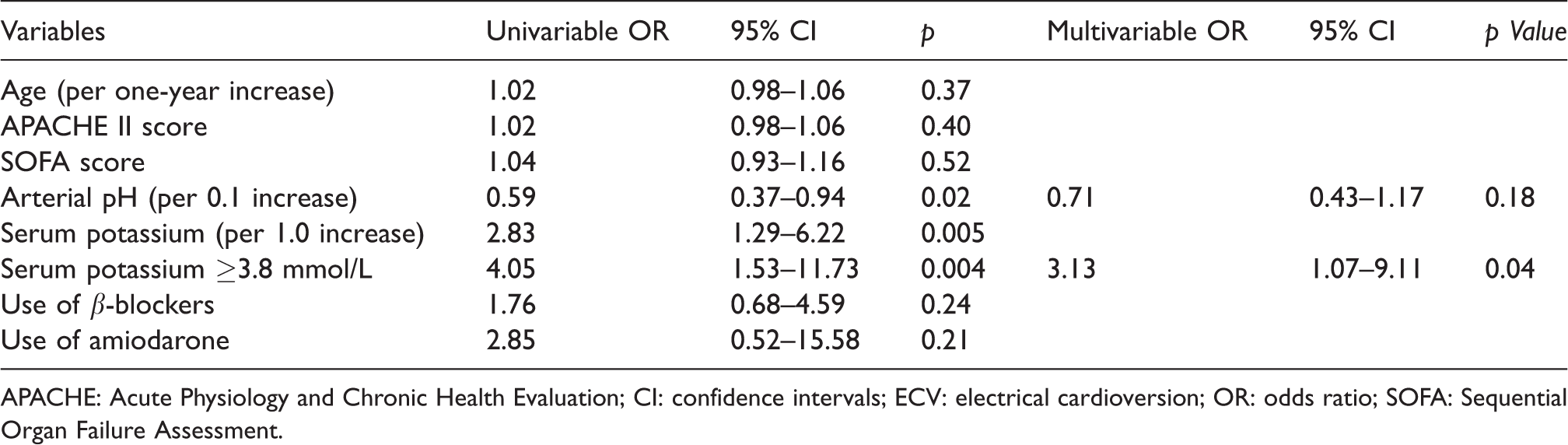
APACHE: Acute Physiology and Chronic Health Evaluation; CI: confidence intervals; ECV: electrical cardioversion; OR: odds ratio; SOFA: Sequential Organ Failure Assessment.
Factors associated with ICU mortality
Univariate analysis identified higher arterial pH (per 0.1 increase) (OR, 2.61; 95% CI, 1.57–4.78; p = 0.0001), infection at AF onset (OR, 0.38; 95% CI, 0.14–0.97; p = 0.04) and SR maintained until ICU discharge (OR, 6.44; 95% CI, 0.78–53.05; p = 0.08) as factors associated with ICU survival (Table 4). Higher arterial pH (per 0.1 increase) (OR, 3.02; 95% CI, 1.61–5.67; p = 0.0006) and SR maintained until ICU discharge (OR, 9.35; 95% CI, 1.02–85.78; p = 0.048) were also significantly associated with ICU survival in multivariate analysis adjusted for APACHE II (Table 4).
Univariate and multivariate analyses of factors associated with ICU survival.
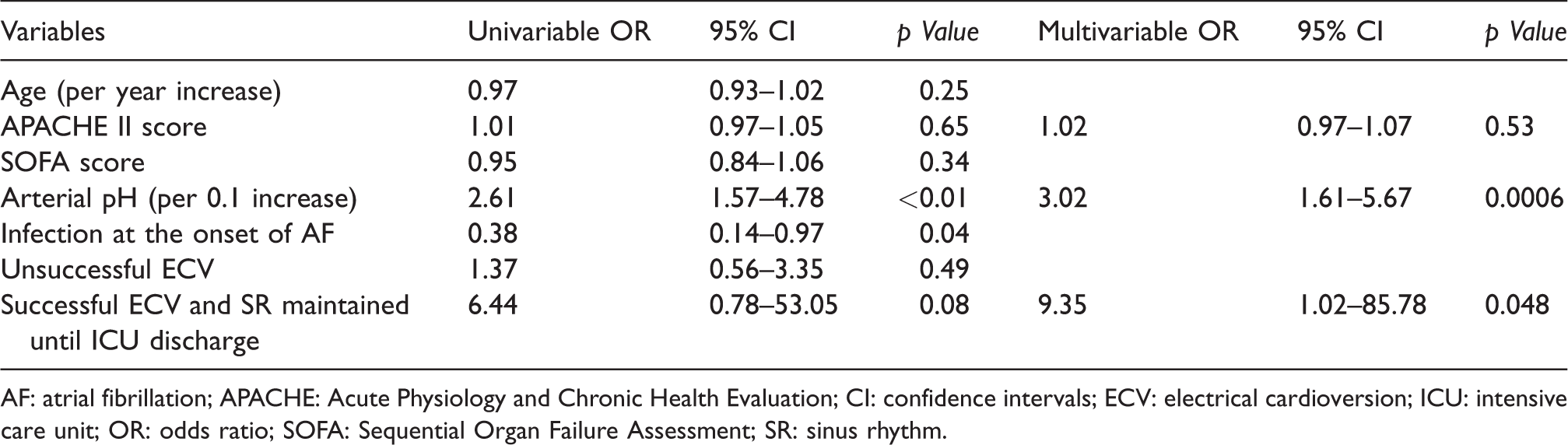
AF: atrial fibrillation; APACHE: Acute Physiology and Chronic Health Evaluation; CI: confidence intervals; ECV: electrical cardioversion; ICU: intensive care unit; OR: odds ratio; SOFA: Sequential Organ Failure Assessment; SR: sinus rhythm.
Discussion
The present study showed that ECV successfully restored SR in about 50% of cases of new-onset AF in critically ill patients with mixed backgrounds, but AF recurred in 73% of patients with successful ECV. A serum potassium concentration ≥3.8 mol/L was associated with successful ECV, while maintenance of SR until ICU discharge following successful ECV was associated with ICU survival. Keeping serum potassium concentration ≥3.8 mol/L at the moment of ECV for new-onset AF might be beneficial to achieve successful ECV.
Previous studies in post-cardiac surgery patients showed a high incidence of AF (30%–60%)13,14 and a frequency of successful ECV of about 35%–71%.10,11 However, information on AF and ECV in critically ill nonsurgical patients is limited. One study showed a high early recurrence rate of AF of 38% in septic patients, 4 which could be explained by the systemic inflammatory response being a cause of AF. 15 Activation of inflammatory signalling pathways 16 and the release of nuclear factor-κB and transforming growth factor-β1 were shown to influence the gene expression of lectin-type oxidised LDL receptor 1 and intercellular adhesion molecule 1 in atrial tissues, resulting in electrical dyssynchrony in the atrial myocardium. 17 However, the results of the current study found no significant association between increased serum C-reactive protein levels or increased body temperature and the recurrence of AF after ECV.
In contrast, higher serum potassium concentrations were significantly associated with successful ECV. This was in accordance with the results of previous studies.8,18,19 Repolarising potassium ion currents have been shown to activate normal membrane excitability in pulmonary vein myocardial sleeves and left atrium. 20 The expression of potassium ion channels in the myocardium varies, with a higher density in the atrium compared with the ventricles. 21 Hypokalaemia (<3.5 mol/L) induces electric vulnerability of the atrium, thus increasing the risk of AF. 22 In a clinical setting, Sultan et al. demonstrated that intravenous administration of potassium and magnesium before ECV increased the success rates of ECV and decreased the required ECV energy. 23 In this study, several factors that can potentially affect the serum potassium level, such as pH, renal replacement therapy and the use of diuretics, were not associated with successful ECV. These findings suggested that it might be advisable to adjust the serum potassium and to maintain serum potassium levels ≥3.8 mol/L to increase the success rate of ECV.
The current results also demonstrated that maintenance of SR until ICU discharge and pH were associated with survival. Physiologically, the restoration of SR after AF improves left ventricular ejection fraction due to synchronised atrial contraction and adequate filling pressures. 24 Gillinov and colleagues reported no significant difference in mortality between rate control and rhythm control in patients with new-onset AF after cardiac surgery; 25 however, given that AF promotes further AF, early rhythm control with ECV might help to prevent persistent AF. Yue et al. showed that persistent AF altered the gene expression of atrial ion channels in dogs, thereby altering ionic currents and promoting the occurrence of AF. 26 Prevention of recurrent AF and maintenance of SR thus appear to be important factors supporting a favourable outcome. Regarding pH, metabolic acidosis influences multiple organs including the cardiovascular and respiratory systems. 27 Notably, acidosis is not only a risk factor for the development of AF post-cardiac surgery, 28 but was also shown to decrease cardiac output and sensitivity to catecholamines. Acidosis may thus be a predictive marker of ICU mortality in AF patients requiring ECV.
This study had several limitations. First, we only included patients with new-onset AF who received ECV. We did not explore the relationship between these patients and AF patients overall, and the characteristics of AF patients who did not receive ECV were therefore unknown. Second, there was no written protocol for the indication and procedures of ECV, resulting in variations in the ECV energies delivered and the number of ECVs. The delivered energy in our study tended to be lower than in a previous study, 10 which could have affected the success rate of ECV. Third, adjunctive therapies (e.g. adjustment of pH and serum potassium levels) before and after ECV were not systematically defined. Fourth, this was a single-centre observational study with a relatively small number of patients. Fifth, the serum magnesium level, a potential covariate for successful ECV, was not included in the analysis, because some of the data were missing in the majority of the patients. Sixth, although we analysed stored ECG data, 12-lead ECG data were not available in all the cases, and we may therefore have missed some cases of recurrence of AF. Finally, because of the methodology of this observational study, the timing of ECV for AF and potassium management strategy at the moment of ECV could not be assessed.
Conclusion
The results of this retrospective study indicated that ECV was successful in about 50% of patients with new-onset AF in mixed ICUs. Higher serum potassium level was a predictive factor for successful ECV, and successful ECV and maintenance of SR until ICU discharge were associated with better ICU survival. Further studies are needed to investigate the potential factors associated with the maintenance of SR to establish a better understanding of new-onset AF in critically ill patients.
Footnotes
Acknowledgements
We thank all staff of Hiroshima University Hospital. We thank Susan Furness, PhD, from Edanz Group (![]() ) for editing a draft of this manuscript.
) for editing a draft of this manuscript.
The institutional review board of Hiroshima University (Trial registration: E-667, registered 31 January 2017) approved an opt-out method of informed consent.
Authors’ contributions include the following: MK, KH, SO, YK, YT and KO drafted the manuscript. MK, KH and NS participated in the design of the study and revised the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.