
Abstract
Abstract
We report a case series of anaphylaxis to chlorhexidine-coated central venous catheters (CVCs) when used in cardiac surgical patients in our institution. Our experience, together with increasing reports of anaphylaxis to chlorhexidine-coated CVCs from other sources indicates that chlorhexidine-coated CVCs are not without additional risk.
Attempts to lower rates of catheter-related bloodstream infection has led to the widespread adoption of chlorhexidine-coated CVCs in the perioperative and critical care setting, including for routine cardiac surgery. However, closer scrutiny indicates that there is lack of strong evidence demonstrating a meaningful reduction in rates of sepsis or serious morbidity, especially with CVC dwell times of less than seven days. Given the lack of clear benefit, we recommend non-coated CVCs for routine cardiac surgery, with even consideration for chlorhexidine-coated CVCs when specifically indicated for patients at high risk of CVC infection.
Introduction
Chlorhexidine is a very commonly used antiseptic agent. However, anaphylaxis to chlorhexidine is an increasingly recognised complication. A recent cluster of three cases of anaphylaxis occurring shortly after insertion of chlorhexidine-impregnated central venous catheters (CVCs) in cardiac surgical patients has caused us to question the merits of their routine use in this setting.
The risks of CVCs are well known, and of particular concern has been the risk of catheter-related bloodstream infection (CRBSI). CRBSI has been found to be a major contributor to overall hospital-related infection, and various measures have been introduced to attempt to reduce the incidence of these infections. 1 One such measure is the use of CVCs impregnated with various anti-infective substances including chlorhexidine and silver sulfadiazine (C-SS). 2 Chlorhexidine, however, is being increasingly recognised as a significant allergen in the perioperative setting. 3 The following three cases occurred within a six-week time period at our institution, and highlight some of the concerns regarding the use of chlorhexidine-impregnated CVCs in routine cardiac surgical patients. All three patients gave consent to the publication of their details.
Case 1
Patient 1, a 71-year-old male, was scheduled for an inpatient mitral valve repair (MVR) for infective endocarditis (IE). He had been unwell with sepsis and worsening mitral valve regurgitation (MR) despite maximal medical therapy. Transoesophageal echocardiography (TOE) demonstrated a 1.6 cm vegetation on the anterior mitral valve leaflet with a perforation of the leaflet and severe MR with an eccentric jet. He had a background of acute on chronic kidney disease, ischaemic heart disease, hypertension, asthma and paroxysmal atrial fibrillation.
After establishing large bore peripheral intravenous (IV) access and connecting routine monitoring including a right radial arterial line, he was induced with midazolam 2 mg, fentanyl 500 μg, propofol 50 mg and paralysed with pancuronium 10 mg. He was also given a prophylactic dose of cefazolin 2 g. Endotracheal intubation was performed uneventfully and the patient was positioned and prepared for central line insertion. At 20 min after induction, a 5-lumen chlorhexidine-impregnated (C-SS) Arrowg+ard CVC was inserted uneventfully into the right subclavian vein. Within 5 min, the patient developed profound hypotension with a flat arterial pressure trace. His systemic arterial pressure was 40 mmHg and minimally responsive to multiple doses of phenylephrine and rapid administration of IV fluids. A period of increased airway pressure was observed with an abnormal end-tidal CO2 trace. A total of 200 μg of adrenaline was administered IV within a few minutes, which resulted in restoration of normal systemic and airway pressures and a mild tachycardia of 100 to 110 bpm. The surgery proceeded uneventfully without further requirement for adrenaline, and at the end of the case with removal of the drapes it was observed that he had widespread urticaria over his abdomen and upper thighs. Of note, in this case, his CVC was left in situ as it was thought by intensive care unit (ICU) staff that pancuronium was the more likely trigger. He subsequently had further hypotensive episodes requiring large volume fluid resuscitation overnight.
Mast cell tryptase levels (in μg/L, normal <11.4) at 1, 4 and 24 h were 12.5, 14.3 and 6.9, respectively. He was subsequently referred to the Australian and New Zealand Anaesthetic Allergy Group (ANZAAG) local testing centre, where he had intradermal testing to cefazolin, pancuronium, midazolam, propofol and chlorhexidine. After an initial negative reaction to chlorhexidine at 1:1000 concentration, he was retested at 1:100 and found to have a positive 9 mm wheal with minimal flare. All other agents tested negative.
Case 2
Patient 2, a 76-year-old male, was booked for a coronary artery bypass graft (CABG) after suffering a non–ST segment elevation myocardial infarction (NSTEMI) a week prior. He had severe three-vessel coronary artery stenosis, with moderate to severe stenosis of the left main coronary as well. The left ventricular ejection fraction (LVEF) was 45–50%, with regional systolic dysfunction and normal valves on echocardiogram. His past medical history included previous coronary stenting, hypertension, dyslipidaemia, gout, osteoarthritis, bilateral total knee replacements and gastro-oesophageal reflux. He was induced with midazolam 2 mg, propofol 70 mg, fentanyl 750 μg and pancuronium 8 mg and was also given cefazolin 2 g. Following intubation, he was positioned and prepared for central line insertion and remained haemodynamically stable for a period of 30 min. Shortly after insertion of a C-SS Arrowg+ard 5 lumen CVC, the patient developed profound hypotension that was unresponsive to large doses of phenylephrine, ephedrine and an IV fluid bolus. He was given adrenaline 50 μg IV, which resulted in normalisation of his blood pressure. At this time a generalised rash was observed. CABG proceeded after relative stability was achieved. Mast cell tryptase levels at 1, 4 and 24 h, respectively, were 20.7, 11.7, and 4.0 μg/L. Post-operatively, in intensive care, his CVC was changed to a non-impregnated line and all sources of chlorhexidine were removed from his room and replaced with iodine-based antiseptics. His post-operative course was complicated by a sternal wound infection, which led to a prolonged six-week stay.
Patient 2 was also referred to the local ANZAAG testing centre, where skin prick testing was negative for propofol, tranexamic acid, pancuronium and cefazolin, but strongly positive to chlorhexidine, with a 12 mm wheal and surrounding flare.
Case 3
Patient 3, also a 71-year-old male, was scheduled for CABG of one week following a NSTEMI. He had severe left main and three-vessel coronary artery disease with an echocardiogram demonstrating normal left ventricular function, normal right ventricle and normal valves. He had a documented allergy to potatoes with no other significant comorbidities. After a similar induction with midazolam 2 mg, propofol 30 mg, fentanyl 500 μg, pancuronium 10 mg and cefazolin 2 g, he remained stable until 10 min after insertion of a C-SS Arrowg+ard 5 lumen CVC, when he suffered a sudden and severe hypotensive episode associated with tachycardia. Again, there was no response to regular vasopressors and fluid boluses. After a few minutes, two doses of adrenaline 50 μg IV were given with good effect. He proceeded to have his CABG with haemodynamic stability. Post-operatively in intensive care, he was noted to have tongue and airway swelling with ongoing hypotension requiring significant vasopressor and inotropic support. He was treated with an ongoing adrenaline infusion, corticosteroids and antihistamines, and the CVC was changed to a non-impregnated line. After continued facial swelling, it was noted that he may have been reacting to the chlorhexidine impregnation of the central line dressings. These were subsequently changed to plain dressings with eventual stabilisation and discharge from hospital after eight days.
His mast cell tryptase levels at 1, 4 and 24 h were 29.3, 24 and 4.9 μg/L, respectively, and a chlorhexidine specific IgE radioallergosorbent test was also elevated, consistent with chlorhexidine as the trigger. As this patient was from overseas and there were additional barriers to further allergy testing, after discussion with an ANZAAG allergy specialist, it was felt there was enough evidence to assume chlorhexidine as the trigger. This patient was counselled and given a letter regarding his likely allergy to chlorhexidine.
Discussion
The three cases above occurred within a six-week time frame at a busy cardiothoracic surgical unit. Each of these patients suffered profound cardiovascular collapse that may have been assessed as a pulseless electrical activity (PEA) arrest if invasive arterial monitoring was not in place. These cases would be classified as grade 3 or 4 anaphylaxis with severe hypotension that would have likely required cardiopulmonary resuscitation if it were not for the cardiac setting with large bore IV access, invasive monitoring and prompt administration of vasopressors and IV adrenaline. While other diagnoses were considered with each case, the timing of events, appearance of rash, positive mast cell tryptase results and subsequent intradermal testing in two patients suggested anaphylaxis to chlorhexidine as the most likely diagnosis. Alternative diagnostic considerations such as tension pneumothorax, pericardial tamponade, septic shower, monitoring error and hypovolaemia were all considered and excluded in each case. In addition, the stability of each patient after induction for 20–30 min suggested that the induction agents were less likely to be responsible.
The offending CVC was removed in patients 2 and 3 post-operatively in the ICU. However, in patient 1, the CVC remained in situ despite ongoing instability and requirement for resuscitation in the ICU. The reasons for this were related to the relative stability achieved in the operating room, the initial uncertainty regarding the diagnosis, and the necessity to avoid further delay of the planned surgery. The failure to change the CVC in patient 1 was possibly related to a lack of consensus regarding chlorhexidine as a trigger. The authors of the recent 6th National Audit Project on Perioperative Anaphylaxis (NAP6) report recommend removing the impregnated CVC if anaphylaxis develops. However, diagnostic uncertainty is common in this setting. 4
Chlorhexidine, first introduced in 1954, is a cationic bis-biguanide antimicrobial agent with broad spectrum activity against gram-positive and gram-negative bacteria as well as dermatophytes, yeasts and some viruses. 5 It is used widely as a disinfectant for skin, oral cavity, dressings, surgical preparation solutions, lubricants, creams and in many other forms. The push to reduce CRBSI has led to the development and marketing of CVCs impregnated with various substances including chlorhexidine, minocycline, rifampicin, silver, platinum, heparin, benzalkonium, carbon and various combinations of these substances. Chlorhexidine–silver sulfadiazine has become one of the more common combinations, and the strong desire by hospitals to reduce infection rates has led to this CVC being used routinely in Australian hospitals including at our own institution.
While there has been some favourable evidence supporting the use of C-SS impregnated CVCs, on closer review many of the studies were not able to show clinically meaningful reduction in infection rates. For example Rupp et al. were able to show reduced rates of colonisation with C-SS lines compared with non-impregnated lines; however, they were unable to show a significant reduction in possible or definite CRBSI. 6 A systematic review published in 2008 identified 18 studies comparing C-SS impregnated CVCs with standard CVCs, and confirmed there was only a weak and not statistically significant association with reduced CRBSI rates however C-SS did reduce rates of catheter colonisation. 1 Of note, the catheter duration ranged from five to 20 days in these studies.
This topic has been reviewed by the Cochrane Collaboration, originally published in 2013 with an update released in 2016.
7
This review found a modest reduction in CRBSI with C-SS CVCs with a risk ratio of 0.73 (0.57–0.94); however, when assessing for meaningful outcomes such as clinical sepsis or mortality there was no significant difference between the groups. In addition, when analysed by rates of CRBSI per 1000 catheter days, the use of C-SS CVCs was associated with a higher risk [risk ratio 1.20 (0.70, 2.06)], although this was not statistically significant. An additional observation from this review was that the majority of studies showing benefit for impregnated CVCs were for patients in the ICU setting with less favourable results outside of the ICU. The authors concluded that: ‘Currently, while the overall body of evidence still allows recommendations in favour of their use in practice, there should be great caution in recommending the use of antimicrobial-impregnated CVCs across all settings without incorporating the current uncertainties on their overall benefits.’
7
A previous review of CRBSI in ICU patients found that the risk of CRBSI when dwell time was less than seven days was less than 1 per 1000 catheter days, and this relatively safe duration extended out to nine days when a ‘bundle’ of measures was implemented. 10
Chlorhexidine allergy is increasingly recognised as a problem in the perioperative setting, and this is thought to be a result of the increased use of chlorhexidine as an almost ubiquitous antimicrobial agent. 3 While the precise incidence of anaphylaxis to chlorhexidine remains unknown, numerous case series have been published since the mid 1980s. In Japan, a series of 13 cases of anaphylaxis to C-SS impregnated CVCs, including at least one death, led to a manufacturer voluntarily withdrawing the product from the market in 1997. 11 A PubMed search for anaphylaxis to chlorhexidine-impregnated CVCs revealed a total of 65 reports from 1994 to 2013. 12 These include a series of eight confirmed anaphylaxis cases for patients undergoing renal transplant, 13 and two series of cardiac surgical patients totalling seven cases.14,15
The increasing incidence of this problem was most recently illustrated in the report of NAP6, which reported chlorhexidine as being responsible for 10% of all episodes and the third commonest cause of perioperative anaphylaxis. 4
A further concern is that there may be under-reporting and under-recognition of chlorhexidine-impregnated CVCs as a cause for anaphylaxis.12,16 A combination of factors may contribute to this, including the fact that chlorhexidine may not be considered a traditional drug in clinical care, but rather a ‘hidden’ allergen. Many clinicians have described to the authors that they were unaware that the CVCs had a chlorhexidine coating, which may in part be due to the subtle labelling of the product. A review of the packaging of C-SS CVC (ARROWg+ard, Teleflex Medical Australia, Mascot, NSW) reveals that labelling of chlorhexidine as a component of the line coating is in small print that is not immediately apparent. In our experience, some clinicians have not been aware that, with ‘Arrow’ branded CVCs, the blue coloured catheters (with a blue sleeve) are coated with chlorhexidine–sulphasalazine whereas the yellow catheters without a sleeve are uncoated standard catheters.
An unfortunate illustration of this problem was described by Chen and Huda in 2016, where a patient suffered anaphylaxis intraoperatively after exposure to chlorhexidine-based skin preparation prior to IV cannulation. 17 Subsequent management included placement of a chlorhexidine-coated CVC leading to further haemodynamic collapse. The patient was stabilised with increasing doses of inotropes and vasopressors and moved to the ICU ward. Once in ICU an indwelling urinary catheter was inserted using a lubricant containing chlorhexidine leading to further patient deterioration. Subsequent testing revealed chlorhexidine as the offending agent leading to a change to that hospital’s anaphylaxis protocols to specifically recommend chlorhexidine-free lines and catheters when managing anaphylaxis.
The occurrence of three cases in a six-week period in our unit clearly represents an unusual cluster, as we are not aware of previous cases occurring in our unit, despite the use of C-SS CVCs for many years. Nevertheless, the authors are aware anecdotally of other cases occurring in different sub specialty areas and in other hospitals.
Of concern, although also anecdotal, is an impression by the authors that numerous hospitals in Australia and New Zealand have changed practice to use C-SS–impregnated CVCs as a routine standard of care in the critical care and perioperative settings. This practice may be inappropriate, because while there may remain a role for C-SS–impregnated CVCs in certain patients, the combination of a lack of clear evidence of benefit for perioperative use, the relatively short expected duration of CVC dwell time, and the recognised risk of anaphylaxis would suggest that these CVCs should not be used routinely in cardiac surgery. Our recommendation is that the standard CVC for routine cardiac surgery is a non-coated line, and that only those patients at high risk of CRBSI or prolonged expected duration of CVC be exposed to chlorhexidine-coated lines. These patients may include those with known immunosuppression, recent cardiogenic shock, mechanical support such as a left ventricular assist device or extracorporeal membrane oxygenation, thoracic organ transplantation recipients or multi-organ failure from other causes including sepsis, cardiac failure or severe comorbid disease. Another potential benefit to avoiding unnecessary chlorhexidine-impregnated CVCs is that in cases of unexpected profound cardiovascular collapse, it removes one of the differential causes of collapse and also removes the need to change a CVC in an unstable patient.
In conclusion, a push towards lowering rates of CRBSI has led to the widespread adoption of chlorhexidine-coated CVCs in the perioperative and critical care settings including routine cardiac surgery. Despite this, there is a lack of strong evidence demonstrating a meaningful reduction in rates of sepsis or serious morbidity in all patient groups, especially if the CVC dwell time is less than seven days. Increasing reports of anaphylaxis to chlorhexidine-coated CVCs and our recent cluster of three cases demonstrate that C-SS–coated CVCs are not without significant risk. We recommend non-coated CVCs for routine cardiac surgery with a consideration for C-SS CVCs only when specifically indicated (Table 1).
Recommended decision making for C-SS CVC versus non-coated CVC. a
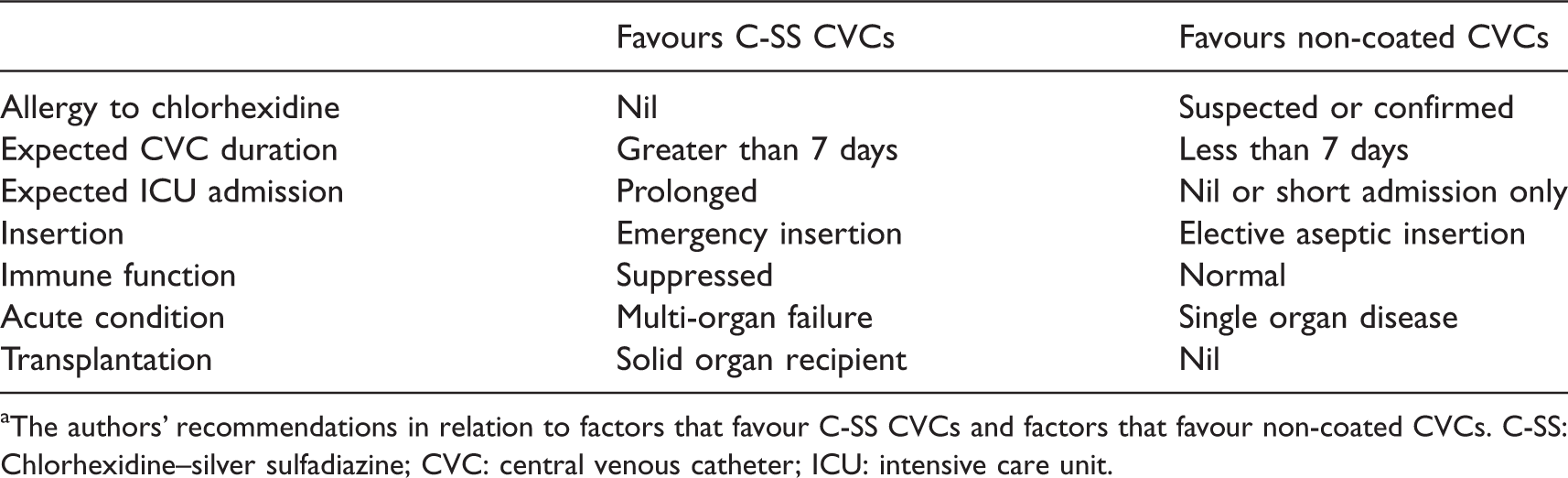
aThe authors’ recommendations in relation to factors that favour C-SS CVCs and factors that favour non-coated CVCs. C-SS: Chlorhexidine–silver sulfadiazine; CVC: central venous catheter; ICU: intensive care unit.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.