
Abstract
Most medical practitioners are not specifically trained to diagnose or manage in-flight medical incidents, yet there may occur a moral obligation to do so when least expected. We felt that knowledge of the frequency of emergency versus non-serious medical incidents, in addition to the clinical spectrum of incidents most often encountered, would be of interest to medical practitioners and, in particular, critical care physicians, who happen to find themselves asked to assist with such events. To this end we collaborated with the Department of Medical Services of a major Australian airline to define the incidence, severity, and type of all in-flight medical events encountered over the course of a year’s flights. We audited in-flight medical data collected over a continuous 12-month period, which covered 131,890 international and domestic flight sectors transporting more than 27 million passengers. There was an average of 296 medical events per month (3555 in total) making the per-flight incidence of a medical event approximately 1:40 (2.7%). Of these in-flight incidents, 915 (26%) were graded as emergencies, with the commonest descriptors of such incidents being either loss of consciousness (37%) or a suspected cardiovascular event (12%). Six of these 915 emergencies proved fatal. Twenty-one flights were diverted due to medical incidents (<0.016% of all flights), with 52% of these attributed to suspected cardiac events. In this series, medical in-flight events were recorded in approximately one in 40 flights, whereas medical emergencies occurred in approximately one in 150 flights.
Introduction
A passenger air flight is a physiologically stressful environment for the human body. During the flight, at a typical cabin altitude of 6000–8000 ft, the fraction of inspired oxygen is lower, approximating 0.16 FiO2.1,2 The Federal Aviation Administration (FAA) requires airlines to maintain cabin pressures at below 8000 ft; 3 barometric pressures may change rapidly and air at high pressures contains lower humidity. 4 This may exacerbate pre-existing conditions for susceptible passengers, such as the cardiopulmonary compromised. Anxiety, fear of flying, claustrophobia, turbulence, and take-off or landing may further increase risks for unexpected clinical deterioration. These factors, combined with the general stressors of travel – sleep deprivation, jet lag, gastrointestinal upset, missing usual medication doses, and pro-thrombotic stasis – increase the risk of a passenger suffering a medical emergency occurring during longer flights.
Although most medical practitioners are able to implement basic life support skills, critical care physicians are trained in airway management and advanced life support and are accustomed to giving resuscitative drugs such as intravenous (IV) adrenaline. 5 The presence of a practising critical care physician in the event of a mid-air crisis could thus prevent an adverse outcome. Yet, even for such specialists, the prospect of being called upon at short notice to provide urgent medical care to an unwell fellow passenger may evoke anxiety for several reasons, 6 as is well described by Eastwood. 7 First, the unfamiliar and cramped fit-out of a commercial passenger aircraft poses logistic challenges in assessing patient status and providing appropriate care: it may be difficult to lie an unwell or unconscious patient flat, equipment may be very different to that encountered in a hospital setting, and the working environment may be noisy and turbulent. Second, assistant help may need to be provided by aircrew or medical staff not currently practising acute medicine. Moreover, administering a duty of care to an undiagnosed and previously unseen patient, while exposed to the scrutiny and emotions of non-medical passengers, could increase professional stress. Third, there may be concern relating to legal liability or a formal complaint in the event of a less-than-ideal outcome, and there can be no firm expectation of any thanks or reward from the patient or airline.
To investigate the frequency with which such events occur, we have undertaken an analysis of in-flight medical incidents with the cooperation of a major Australian commercial air carrier. We aimed to determine the frequency of clinical in-flight events, and the severity and nature of these events. We also documented the equipment available on board for managing such incidents.
Methods
Data were collected from all of the airline’s international and domestic flights across 12 consecutive months during 2015–2016. The data were extracted by the airline retrospectively from (a) accounts of medical incidents by cabin crew, and (b) medical notes written by assisting doctors. These data are collected and stored privately by the airline in a custom-made database. Permission was given by the airline to publish this subset of fully de-identified data regarding event counts, medical categorisations, and flight diversions.
Medical incidents were characterised primarily in terms of presentation and severity. The airline assigns an internally devised severity grade to each incident – ranging from grade I to grade III, with grade III events being the most severe. Events were also categorised in terms of whether ground-based telemedicine services were utilised, and whether the aircraft medical kit was required. Relevant to this aim, the International Air Transport Association (IATA) has published a list of recommended medical equipment to be carried on board all passenger aircraft; the IATA-recommended contents of an airline medical kit are reproduced in Table 1. It is our impression that most major airline medical kits exceed these minimum requirements.
Aerospace Medical Association recommended emergency medical kit (IATA medical manual, 2018: 68–69). 9
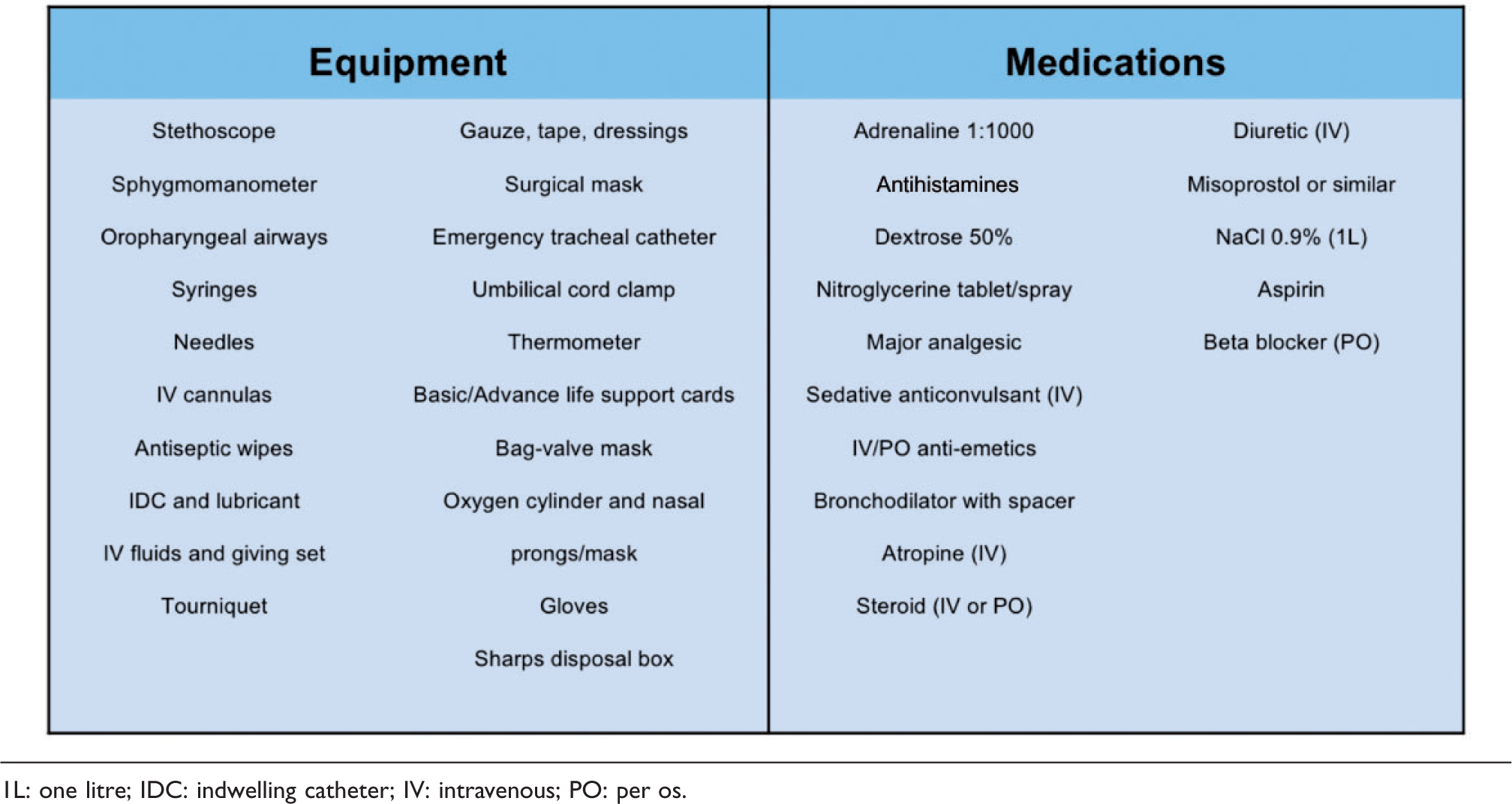
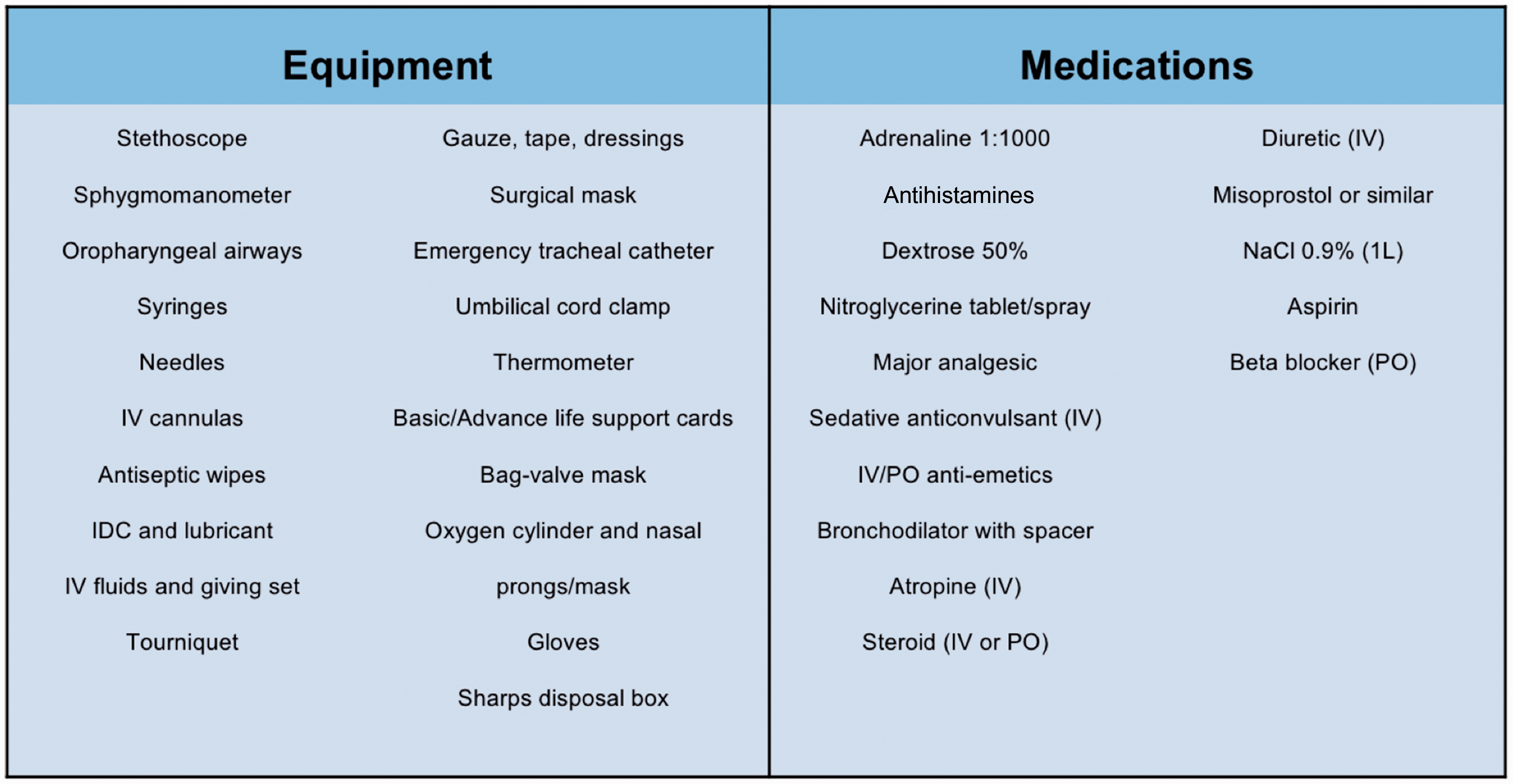
1L: one litre; IDC: indwelling catheter; IV: intravenous; PO: per os.
Results
Frequency of in-flight medical incidents and emergencies
The airline reported an average of 296 medical events per month (total 3555 over 12 months) on Australian domestic and international flights over the period of interest during 2015–2016, translating into a frequency of approximately one medical event per 40 flights. To place this in context, in a 12-month period the airline operates 131,890 domestic and international flights carrying over 27 million passengers. Most (74%) of events were non-emergent, and were classified as grade I or grade II events.
Specific records were maintained about sentinel medical incidents, which were all definable as grade III events, hereinafter termed ‘emergencies’. There were a total of 915 emergencies (26% of all recorded incidents) over the study period. Six of these (0.66% of all emergencies) were fatal.
Flight diversions and medical kit usage associated with medical incidents
In the 12-month period, there were 21 flight diversions due to a medical event (2.3% of all emergencies, and only 0.6% of all medical events). Of these, 52% were attributed to a suspected cardiac event, with neurological causes (e.g. seizure, suspected stroke, loss of consciousness) making up the second most common group at 14% (Figure 1). We had insufficient data to relate the frequency of diversions to the duration of flight sectors.
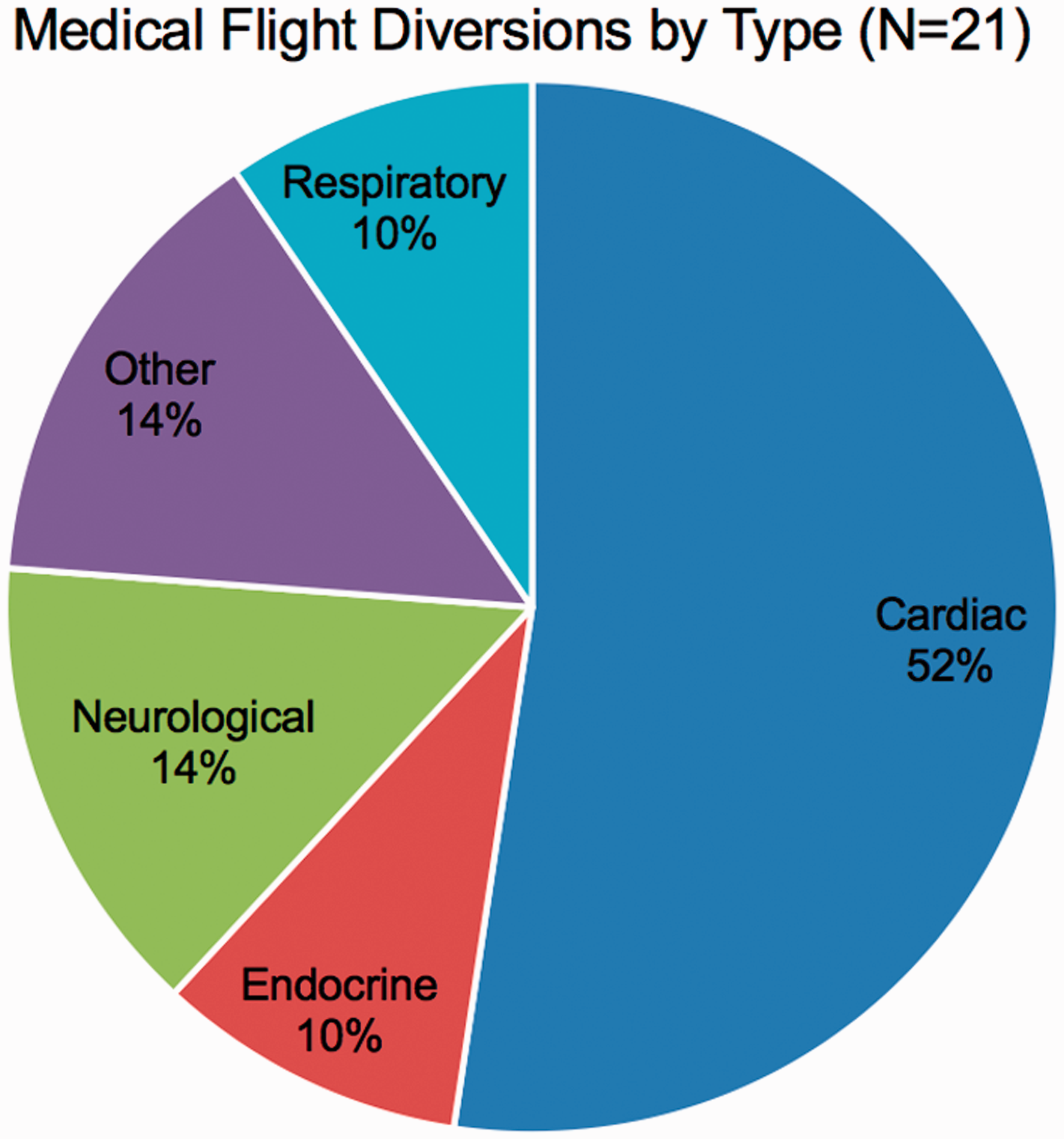
Cause-dependent medical flight diversions occurring on an Australian airline's domestic and international flights over a 12-month period during 2015–2016.
The airline’s physician medical kit was utilised in 37% of all the medical incidents, whether emergency or non-emergency. Although no breakdown of the latter subgroups is available, this statistic indicates that some medical incidents of less than emergency severity as defined here – e.g. grade II events – nonetheless required use of the medical kit. Ground-based telemedicine services were contacted in 18.9% of all medical events, presumably triggered by an emergency rather than a non-emergency in-flight event (although no such sub-analysis was available).
Presentation of medical incidents and emergencies
The accounts of in-flight emergencies (grade III emergency events excluding death) were grouped by the airline into six broad categories: cardiac arrest, chest pain, anaphylaxis, loss of consciousness, seizure and death. Of the 915 medical emergencies, 374 were recorded as ‘other’, indicating that the diagnosis was either unclear or not documented for other reasons. These latter cases are not included in our clinical presentation analysis. The remaining 541 emergencies were assigned a presentation category by airline staff. Loss of consciousness was the most common, accounting for 37% of all emergencies.
Discussion
The main findings of this study are that in-flight medical events are uncommon (about one in 40 flights), with emergencies making up only about 25% (about one in 150 flights). Very few required a flight diversion (<1% of all medical events).
Airlines attempt to screen patients who are known to be high-risk, and have medical advisors for this purpose. While there are no universal criteria for assessing a patient’s medical fitness to tolerate a flight, protocols are evolving and being updated. 8 For example, the IATA medical manual includes a guideline for assessing fitness to fly, which many airlines follow. 9
Airline staff routinely undergo annual first aid training and refresher courses, including cardiopulmonary resuscitation (CPR) and the use of an automated external defibrillator (AED). 9 Minor events can be managed by cabin crew who can provide first aid, simple analgesia, and reassurance to distressed passengers; for such minor ailments, flight attendants have access to a first aid kit which is stored separately to the medical kit. 10 On the other hand, airline medical kits provide basic clinical equipment to deal with common medical conditions. The content of the kit varies between airlines, but usually include a basic number of drugs, a stethoscope, sphygmomanometer, IV fluids, cannulation equipment, personal protective equipment and basic airway adjuncts. Flight attendants may use the medical kit only under the direction of a licensed medical practitioner. An AED was carried on all flights in this study, and carriage of such is recommended by the IATA. 9 According to US Federal Aviation Administration regulations, a medical kit and AED are required for passenger aircraft operation. 10 Some airlines supply more advanced resuscitation equipment; on Lufthansa long haul flights, for example, intubation equipment including endotracheal tubes and a laryngoscope is provided. 11 Some aircraft have the capacity to store a deceased person in a compartment in the event of their death. 12
Methods of data collection for in-flight medical incidents tend to be airline-specific, making it challenging to obtain a clear overview of past research in this field. For example, one study reported that in-flight medical emergencies occur only in 1:604 commercial flights, 13 but such data depend on the definition of in-flight medical emergency and/or the duration of flights analysed. There is no standard categorisation system for in-flight medical incidents used by all carriers.
Common medical incidents reported include syncope, followed by gastrointestinal disturbance and respiratory complaints;10,13 other frequent presentations include cardiovascular symptoms, non-syncopal neurological symptoms, trauma, allergic reactions, obstetric or gynaecological emergencies, psychiatric disturbance and intoxication. 10
Reports vary widely as to the frequency of involvement of a medical doctor during in-flight medical incidents, with individual studies quoting anywhere between 12% 14 to 86% 15 – a broad range that presumably reflects geographic factors, flight duration, aircraft passenger load and differences in the definitional severity of the medical incidents studied. Overall, volunteer medical professionals have been reported to be involved in approximately 35% of all in-flight medical incidents. 16 In support, data from Air Canada indicate that a nurse, doctor or paramedic rendered assistance in 49–53% of in-flight medical emergencies. 2 It is by no means infrequent, however, that there is no medical practitioner available.8,17 Airlines may be required to request proof of medical qualifications or identification of volunteer physicians, and to keep records of the incident including who attended and the treatment or intervention they provided. Volunteering physicians should document their assessment and interventions using either a standard airline medical incident form, or in some other written form able to copied for one’s own professional records. 10
Medical practitioners have been reported to be involved in as many as 85% of medical incidents where the flight was diverted due to a sick passenger. 16 Diversion rates are higher in cases where physicians are involved or the AED is used, compared to those incidents managed by nurses, paramedics or flight crew alone.13,17 However, it is not possible to make inferences from these data.
Diverting the plane is a complicated decision with far-reaching implications, and so must take into consideration factors such as flight safety, on-board fuel, cost, medical facilities, ground-based medical teams and transport time, and ability to land at the closest appropriate airport. For example, as pragmatically highlighted by Ruskin et al., cardiopulmonary resuscitation (CPR) may need to be interrupted during a landing, creating safety concerns for both patients and doctors that need to be discounted prior to any diversion. 18 A study by Valani et al. found that cardiac events were the most common precipitant of medical flight diversions, followed by neurological symptoms. 19 A recent German study in 2017 is in accordance with these results, reporting chest symptoms, circulatory collapse and altered mental status as the commonest cause of diversions. 20 Unsurprisingly, medical incidents causing diversions are associated with a higher death rate of 22%, compared with only 0.7% of all on-board medical emergencies. 16 This previously reported figure of 0.7% is similar to the 0.66% death rate (as a proportion of all emergencies) observed in our study. A 1996–1997 study of US flights found that of 15 on-board fatalities, only four (27%) resulted in a flight diversion. 17 This could indicate a preponderance of cardiac arrests with non-shockable rhythms in that series (some of which may not even be witnessed at first during a flight), as pointed out by Ruskin et al. 18 It is the airline captain who makes the decision as whether or not it is necessary to divert the plane, and in case of dispute or uncertainty, the captain can take advice from both in-flight medical support and specialist ground-based telemedicine physicians. 8
In the case of an emergency diversion and landing (or in fact any medical event that occurs on board), a ground medical team may be contactable. The purpose of this is not only to provide real-time advice for acute on-board management of the patient, but also to assist in coordinating medical services for a ground response team upon landing. Modern on-board telemedicine facilities are capable of transmitting live video and audio communications and even 12-lead electrocardiogram (ECG) (if available) to experienced critical care physicians on the ground. Telemedicine providers may have insurance that legally covers actions of involved practitioners, but this should not be assumed. Once the ground medical team has been contacted, and provided that the communication is clear, the medical practitioner may have reduced medicolegal liability for on-board interventions if they are following instructions given. 8
To the best of our knowledge, there is no mandatory legal obligation for a medical practitioner to assist in an emergency situation. In the landmark Dekker v Medical Board of Australia case, 21 in which a radiologist failed to provide medical assistance to the victims of a motor vehicle accident, no charge was laid; the Court ruled that doctors do not have a legal duty to provide medical treatment to someone who is not their patient. 22 However, although no fault was proven, it is notable that the case lasted for 12 years until its dismissal due to lack of evidence at a tribunal in 2013, and such a lengthy duration of proceedings would likely have caused personal and professional distress. 23 This case illustrates issues relevant to providing in-flight medical aid, in that the event occurred in a remote environment without medical support, and the practitioner was not specifically trained in the field of critical care or trauma patients.
According to the Medical Board of Australia’s code of conduct, good medical practice includes rendering assistance in an emergency within the limits of one’s own capabilities. 24 From a legal perspective, the Good Samaritan law protects practitioners who have offered their skills in good faith to aid a person in need. The specific laws of the in-flight situation are less clear, particularly where international travel is involved, since laws differ between countries. Technically, an on-board medical practitioner may be subject to the laws in the country the aircraft is registered in, the country of destination, and/or the country the aircraft was flying over when the event occurred.25,26 To the best of the authors’ knowledge, there has not been a case in which a health practitioner has been held liable as a consequence of not becoming involved in an in-flight medical emergency. 27 On the other hand, a recent lawsuit was filed in the USA against American Airlines after the pilot refused to divert a six-hour flight for an unwell passenger despite the pleas of a doctor on board. The 25-year-old woman died during the flight from a pulmonary embolism despite the doctor’s attempts to resuscitate her; after she arrested, the AED on board was found to be faulty. The case is still proceeding, and the outcome may set a precedent for future legal actions surrounding in-flight medical incidents in the USA. 28
In the USA, volunteering doctors are rendered some degree of protection under the Aviation Assistance Act of 1998,
29
which states that, An individual shall not be liable for damages in any action brought in a Federal or State court arising out of the acts or omissions of the individual in providing or attempting to provide assistance in the case of an in-flight medical emergency. (p. 2)
Good Samaritan laws in Australia do not protect practitioners if their on-board interventions are proven to be demonstrably negligent, impaired (e.g. due to alcohol intoxication, such as may not be uncommon in the off-duty setting), or intentionally harmful.
25
The most recent review of the Australian Law of Negligence highlights this lack of universal protection: A complete exemption from liability for rendering assistance in an emergency would tip the scales of personal responsibility too heavily in favour of interveners and against the interests of those requiring assistance. In our view, there are no compelling arguments for such an exemption. (p. 12)
30
There are several important limitations of this study. First, the study sample is limited by its small size, and by the data having been obtained from a single albeit major airline over a period of less than two years. Second, the data were retrospective. Third, the data were obtained from written accounts by airline staff, with the primary data not able to have been assessed by the researchers due to confidentiality restrictions. Fourth, there was a lack of recording of a precise final diagnosis for the medical incident – i.e. events were categorised into provisional diagnostic suspicions such as ‘cardiac’ and ‘neurological’ – both of which represent a diverse range of diagnoses. Fifth, there were no data regarding longer-term outcomes of patients after leaving the aircraft. Sixth, with respect to flight diversions, length of flight sector data were not available, making it difficult to make inferences from the diversion data. Seventh, this study was focused on an Australian airline, making the outcomes potentially more relevant to Australian than other country cohorts. Finally, we stress that the foregoing is presented for purposes of discussion only; it is not based on formal legal advice, and provides no guarantees or warranties to any third party.
Conclusions
In this series, medical in-flight events were recorded in approximately one in 40 flights, whereas medical emergencies occurred in approximately one in 150 flights. The in-flight medical kit was used for 37% of all medical events. This confirms that the majority of in-flight medical incidents are non life-threatening. Loss of consciousness was the most common emergency, followed by a suspected cardiovascular event. Emergencies requiring a flight diversion were very rare, as were in-flight deaths.
Footnotes
Acknowledgements
The authors acknowledge the kind cooperation and participation of Qantas Airways Australia and Avant Medical Indemnity Insurance. They wish to thank David Preswick of Qantas Airways and Morag Smith of Avant for their contribution to this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.