
Abstract
The provision of appropriate discharge analgesia can be challenging and is often prescribed by some of the most junior members of the medical team. Opioid abuse has been considered a growing public health crisis and physician overprescribing is a major contributor. In 2015 an initial audit of discharge analgesia at the Royal Perth Hospital led to the development of discharge analgesia guidelines. Compliance with these guidelines was assessed by a follow-up audit in 2016, which showed improved practice. This audit assesses discharge analgesia prescribing practices two years following guideline implementation. Dispensing data were obtained for analgesic medication over a three-month period from April to July 2017 and 100 unique patients were chosen using computer generated randomisation. Patients’ medical records were assessed against the hospital’s Postoperative Inpatients Discharge Analgesia Guidelines. The data collected were then compared with equivalent data from the previous 2015 and 2016 audits. Overall 83.4% of the 170 discharge analgesia prescriptions written were compliant with guidelines. The highest overall compliance rates were achieved for paracetamol (100%, up from 95.9% in 2016), celecoxib (96%, down from 100% in 2016), and oxycodone immediate release (IR) (74%, down from 88.9% in 2016). The quantity of oxycodone IR given on discharge complied with quantity guidelines in only 56% of cases. Overall there has been a significant and sustained improvement in appropriateness of discharge analgesia prescribing since 2015, though the results from 2017 show less compliance than 2016 and that achieving compliance with quantity guidelines is an ongoing challenge. This demonstrates the challenge of obtaining high adherence to guidelines over a longer time period.
Keywords
Introduction
Poor postoperative pain management has been associated with a number of adverse physiological and psychological effects.1,2 Poorly controlled acute postoperative pain is also a risk factor for chronic pain, which causes significant morbidity and economic cost. 2 Postoperative pain, and pain post-discharge has been identified by patients as a problem of considerable concern. 3 There is scope to improve the post-discharge pain experienced by surgical patients. A survey of 300 patients who underwent surgery found that post-discharge, 46% experienced moderate pain, 21% experienced severe pain, and 6% experienced extreme pain. 3
On the other hand, opioid abuse has been considered a growing public health crisis and physician overprescribing is a major contributor. 4 The provision of appropriate discharge analgesia can be challenging and is often prescribed by some of the most junior members of the medical team. Many opioid prescriptions may not be appropriate, and opioid prescriptions for acute pain can lead to unintended transition to long-term opioid use. 5 There may be significant variations in the amount of opioids that different doctors prescribe. Makary et al. found the amount of opioid tablets prescribed post routine laparoscopic cholecystectomy varied between 0 and 50, and only around 10% of prescriptions were considered to represent best practice. 4
The implementation of high-quality guidelines is one component in the provision of safe and effective acute pain management, and responsible opioid prescribing. There is evidence suggesting that guidelines can improve analgesic prescribing practices.6–8 Introduction of statewide guidelines has been associated with a significant decrease in quantity of opioid prescriptions by emergency physicians, and introduction of hospital guidelines may lead to improvements in ward-based opioid prescribing.6,7 Despite the potential positive effects, achieving ongoing compliance with guidelines remains a challenge.
Royal Perth Hospital (RPH) is a 450-bed tertiary teaching hospital in Western Australia. RPH provides an extensive range of surgical services including plastics, general surgery, orthopaedic, urology, and vascular. In 2015 an initial audit conducted at RPH assessed the prescription of analgesic medications on discharge for surgical patients. This led to the development of discharge analgesia guidelines (Table 1) and staff education by the Acute Pain Service (APS) and hospital pharmacists. These guidelines were introduced in 2015 and a follow-up audit in 2016 showed improvements in discharge analgesia prescription practices and a positive attitude from hospital pharmacists towards the guidelines.
Summary of the Royal Perth Hospital Postoperative Inpatients Discharge Analgesia Guidelines.
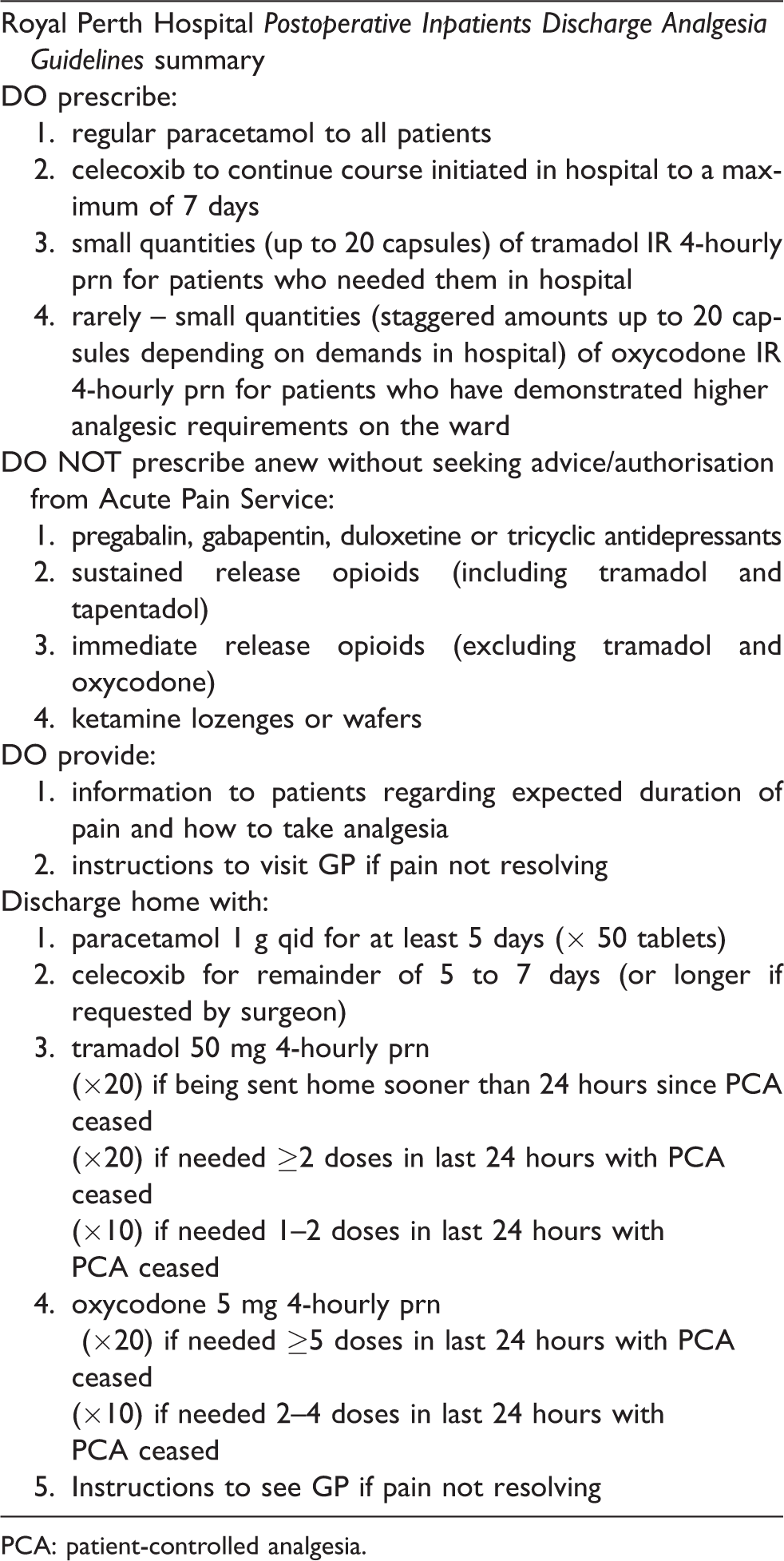
PCA: patient-controlled analgesia.
This audit aimed to assess whether the improvements in postoperative discharge analgesic prescribing has been sustained two years following the implementation of guidelines.
Materials and methods
This audit was approved by RPH as a quality improvement activity and approved for publication (WA Health GEKO approval 21877). The methodology for this 2017 audit was based on the previous audits performed in 2015 and 2016. Medication dispensing data were obtained for all patients discharged from RPH from the 1 April 2017 to 31 July 2017, then 100 unique patients discharged from surgical wards were randomly chosen using computer-generated randomisation.
Inclusion criteria: all patients prescribed analgesia when discharged from a surgical ward.
Exclusion criteria: patients prescribed paracetamol alone. Patients discharged from emergency and medical wards.
Data were collected retrospectively through review of patients’ medical records by three resident medical officers working in the RPH anaesthetics department. The medical records were assessed against the Royal Perth Hospital Postoperative Inpatients Discharge Analgesia Guidelines (Table 1), which included assessing which medications were prescribed, quantities and dosing of medications prescribed, overall compliance with the guidelines, involvement of the APS, and whether instructions were given to see their GP if pain is not resolving.
Prescriptions were classified as appropriate and complying with guidelines if following review of patients’ medication charts and inpatient medical notes (including assessing evidence of involvement of APS) the prescription was found to adhere to the ‘DO prescribe’ and ‘DO NOT prescribe anew…’ rules of the guidelines. In addition to overall compliance with guidelines (i.e. was the medication appropriate to prescribe?), the quantity of medication prescribed was assessed against recommended quantities in the guideline. Prescriptions for analgesic medication that patients were taking prior to admission to hospital were considered to be repeat prescriptions and excluded from analysis. The data collected were then compared with equivalent data from the previous 2015 and 2016 audits.
Results
Of the 100 randomised patients, 23 were excluded as they were prescribed only paracetamol. The medical records of a further 17 patients (22%) were unavailable so also excluded. There were slightly fewer patients reviewed in this audit than in previous years (60, vs 68 in 2016 and 70 in 2017). Of the 60 patients whose records were manually reviewed, paracetamol remained the most common analgesia prescribed with 80% of patients receiving a new script for paracetamol on discharge (Figure 1). This was followed by tramadol immediate release (IR) (62%), celecoxib (45%), and oxycodone in IR formulation (tablets) of 5 mg and higher (38%). This order of prescribing frequency has remained unchanged since the initial audit in 2015. There were no scripts written for oxycodone/naloxone slow release (SR), or oxycodone SR in the 2017 audit.
The percentage of patients being discharged with paracetamol, tramadol IR, celecoxib, oxycodone IR, and tapentadol SR has risen from the rates reported in the 2016 audit, while the percentage of patients being discharged with pregabalin and oxycodone/naloxone SR has fallen. The medications most compliant with quantity guidelines were paracetamol (96%) and celecoxib (86%), while those least compliant with quantity guidelines were tramadol IR (66%) and oxycodone IR (56%) (Figure 3).
Overall 83.4% of the 170 discharge analgesia prescriptions written were compliant with guidelines. This is down from an overall 93.5% compliance in 2016. The highest compliance rates were achieved for paracetamol (100%, up from 95.9% in 2016), celecoxib (96%, down from 100% in 2016), and oxycodone IR (74%, down from 88.9% in 2016) (Figure 2). Lowest compliance rates were achieved for pregabalin (50%, down from 92.9%), and tapentadol SR (60%, down from 80%). The APS was involved in 18% of discharges in the 2017 audit (up from 9% in 2016, down from 26% in 2015). Only 14% of patients were discharged with written instructions to see their GP if experiencing worsening pain.
Discussion
Overall discharge analgesia prescribing practice has improved since guidelines were first introduced in 2015, with the highest overall compliance with guidelines being achieved in 2016. Compliance with medication guidelines was higher than compliance with quantity guidelines, suggesting that appropriate discharge medications are being prescribed to patients, but too many tablets are being given. The decrease in compliance from the 2016 audit results demonstrates the challenge of maintaining ongoing compliance with guidelines over a longer time period. The low compliance rates for pregabalin and tapentadol SR are primarily a result of not obtaining APS input prior to prescribing these medications on discharge, a requirement that is stipulated in the guidelines. Compliance of opioid prescriptions with quantity guidelines is an important parameter clinically and for the community. The amount of inappropriately prescribed discharge opioids has decreased since 2015, but concerningly, the quantity of oxycodone IR given in 2017 complied with quantity guidelines in only 56% of cases.
Currently standards are maintained by informal and largely unstructured ward-based education of rotating junior doctors by pharmacy staff and other members of the healthcare team. The guidelines are placed on the walls of doctors’ offices in all wards. Pharmacists review all discharge prescriptions and contact prescribers if the prescription does not comply with the guidelines. Pharmacists also ask for an APS review for patients being prescribed pregabalin or SR opioids. However, prescribers often default to the maximum allowable Pharmaceutical Benefits Schedule quantities and there have been cases of conflict between prescribers, pharmacists and pain registrars. As the quantities in the guidelines are currently not binding, the pharmacists are not empowered to enforce the quantities stipulated.
There are multiple ongoing efforts to improve future compliance with the guidelines. They have been submitted to the RPH Drugs and Therapeutics Committee requesting endorsement of the guidelines as Standard Operating Procedures. It is expected that this will increase awareness of the importance of considered individualised discharge analgesic prescribing and improve compliance. A submission to put tapentadol IR onto the WA statewide formulary has been made with the goal to replace most oxycodone IR scripts by tapentadol IR, carrying a much-reduced risk of toxicity, 9 as well as of diversion and abuse. 10
There is a strong desire to increase the education frequency of junior doctors and registrars regarding the guidelines, however the resourcing and timing of this remains a challenge. There is also an effort to promote consultation with the APS for patients requiring slow release analgesia such as tapentadol, or atypical agents such as pregabalin. Furthermore, this audit is planned to continue on a yearly basis to assess ongoing compliance and changes, and there are plans to expand the scope of future audits to include other clinically relevant outcomes such as patients’ pain post discharge.
Several limitations of this audit were identified. Audits were conducted retrospectively over a three-year time period by different clinical staff. Though the data collected were the same each year, interpretations of guidelines in ambiguous situations may not have been consistent. In 2016 the guidelines were taken to be best practice and applied retrospectively to the data collected in 2015. While this should not affect comparisons of 2017 data to 2016 data, it may make comparisons of 2017 data to 2015 data less useful. Follow-up of patients post discharge was outside of the scope of this audit. It would be useful in future to assess the clinical impact of guideline compliance by assessing patients’ post-discharge pain scores. There have been numerous changes at RPH over the last three years, with some surgical specialties being moved to a different hospital, and many changing wards multiple times. There is also an ongoing changeover of staff, with junior medical officers’ rotations lasting around three months. This presents challenges in developing a strong guideline-based discharge analgesia prescribing culture, though these challenges are most likely not unique to RPH. Finally, a substantial number of medical records requested for audit were not available.
Despite numerous limitations the results of the 2017 audit suggest that overall the improvement in discharge analgesia prescribing has been sustained since the introduction of the guidelines in 2015, however more work is required to improve compliance of oxycodone IR with quantity guidelines. The decrease in compliance seen since 2016 demonstrates the challenge of maintaining high compliance with guidelines over a longer time period. Recommendations resulting from this audit include increasing focus on discharging patients with appropriate quantities of medication as part of individually considered analgesia plans.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.