
Abstract

Due to the risk of hypoxia following general anaesthesia, supplemental oxygen administration in the immediate post-anaesthetic care period is widely regarded as a standard of care. We recently audited the rate of failure of delivery of supplemental oxygen in this period in our institution, and sought to identify the causes and contributory factors (Quality Assurance activity identifier code R0253/15).
Over a 175-day period, 22 anaesthetic nurses (from a total staff bank of 37) were assigned to be silent observers of supplemental oxygen delivery during weekday elective operating lists, which had at least one patient requiring the use of an oxygen mask during the recovery period. All nurse observers were trained in this role by our research nurse.
The nurse did not inform other staff of their role in order to preserve the normal staff workflow. The nurse would observe the placement of the Hudson mask by the anaesthetist at the end of each case and would check that the oxygen cylinder (located either under or at the foot-end of the bed) to confirm that the cylinder was turned on and had a sufficient reserve of oxygen for transport of the patient to the post-anaesthesia care unit (PACU). Any instance of failure of oxygen flow to the patient once fitted with a Hudson mask (either due to tubing not connected to the cylinder, cylinder not turned on, or cylinder empty) for a minimum of 15 s was deemed a ‘reportable event’. This would then trigger the observer to inform the anaesthetist and to document the cause. The nurse would then follow the patient to the PACU maintaining surveillance until transfer of the oxygen source to the wall-mounted oxygen outlet, including its activation. Any instance of the mask unwittingly remaining without oxygen flow for greater than 15 s, either during transport or during handover in the PACU, was similarly deemed a ‘reportable event’, triggering the observer to inform staff so that the flow could be instituted.
From a total of 4566 eligible cases performed at the institution over the study period, 511 operative cases were audited. This was a non-randomised convenience sample. There were a total of 37 instances of failure of supplementary oxygen delivery in 32 patients, yielding an event rate of 6.3% (95% confidence intervals (CI), 4.47–8.71%). Causes included failure to turn on the oxygen cylinder (18), failure to connect oxygen tubing (17), connection to an empty cylinder (2), and failure to turn on an oxygen wall outlet (2); two events had two simultaneous causes. There were no events caused by failure of an oxygen cylinder when used correctly. Figures 1 and 2 outline locations in the patients’ care pathway where events occurred and their causes.
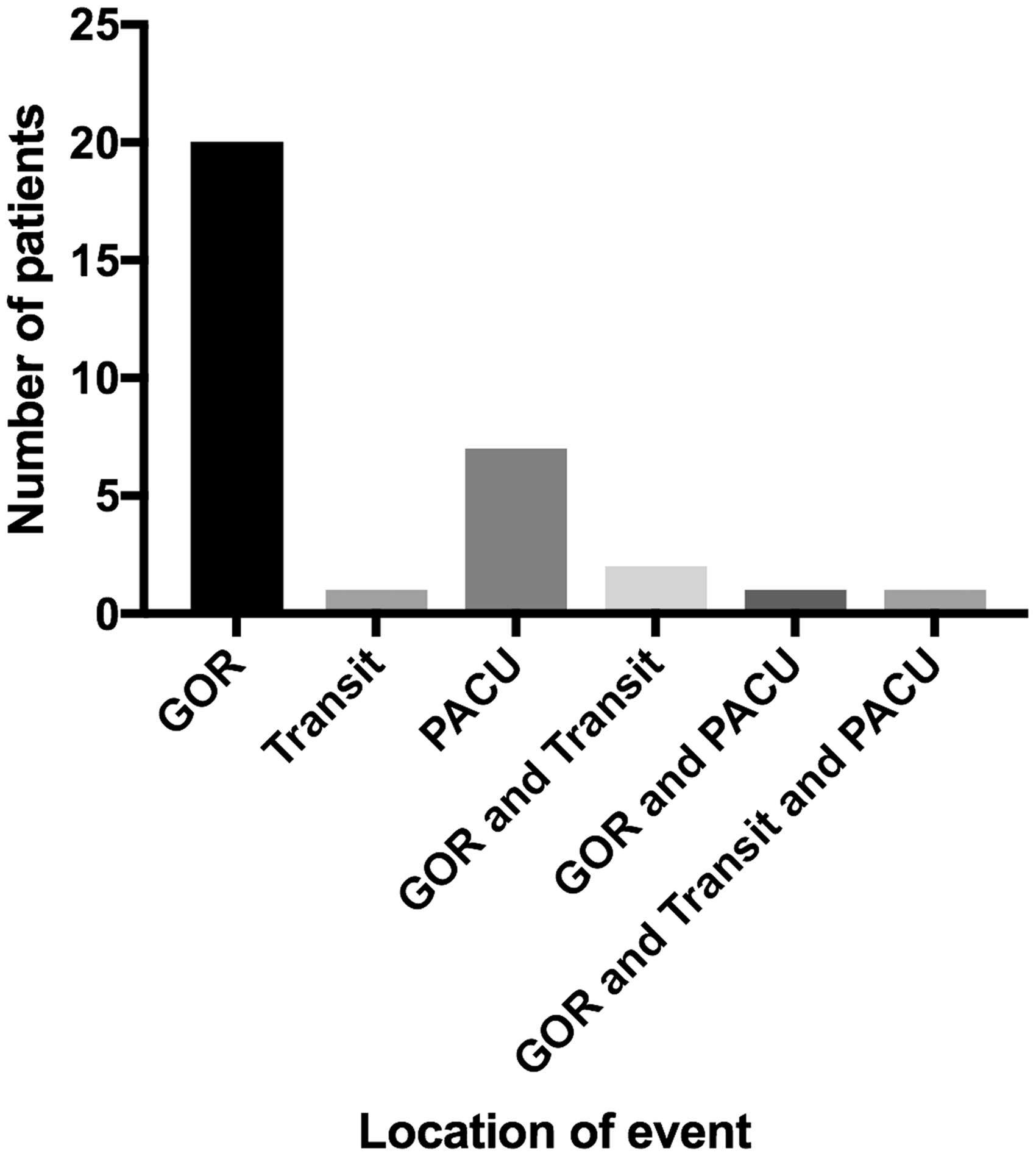
An overview of the failure of supplementary oxygen delivery events at different points in the patient transition through postoperative care.GOR: general operating room, PACU: post-anaesthesia care unit.
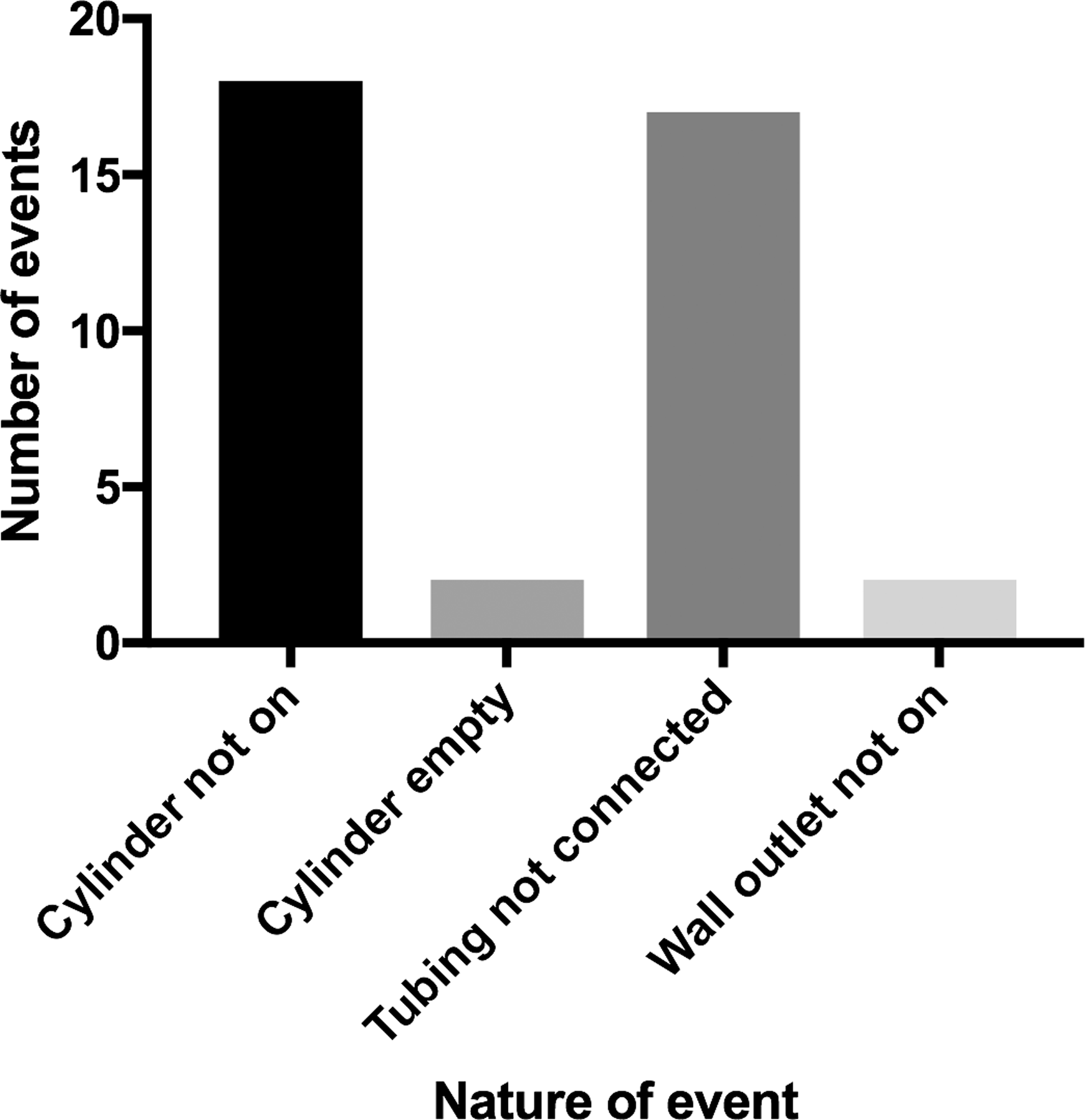
A breakdown of the causes of failed supplementary oxygen delivery in the 37 patients.
Our 6.3% event rate must be interpreted with caution due to the possibility of selection bias. Nevertheless, even accounting for the possibility of a selection bias, the results are concerning. As with any audit, these findings pertain mostly to our institution. However, it is likely that similar errors would be observed in other institutions in Australia and the region that use a similar process for transfer of patients from operating theatres to PACUs.
There have been several previous reports of failure to provide appropriate delivery of supplementary oxygen in a variety of hospital settings, including a patient safety alert by the National Health Service (NHS) in the United Kingdom.1–5 As in our audit, most cases were due to human error rather than equipment failure. Nevertheless, concerns about oxygen cylinder regulator design have been expressed,4,5 and faulty dial regulators have been reported. 6 Our findings support these previous reports.
Following the example of the NHS, all staff involved in patient care should be alerted to the potential errors in the delivery of supplementary oxygen to patients, and anaesthesia departments should ensure that all staff are aware of these errors and take measures to avoid them in their practice.
Footnotes
Acknowledgements
The authors acknowledge the editing assistance of Professor David A. Scott and the diligent work of Candice Williams (Anaesthetic Clinical Nurse Specialist) for her role in training and recruiting of observers and collecting data.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors have disclosed their ownership of the SureflO2™ (SureflO2 Trading Pty Ltd, Oakleigh, Victoria) device, which is a visual indicator of gas flow into medium concentration oxygen masks. The authors did not perform any observation or data collection to minimize bias but acknowledge this presents a potential conflict of interest as this study examines oxygen flow failure into Hudson type masks.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.