
Abstract
Abstract
Intermittent pneumatic compression (IPC) to the lower limbs is widely used as a mechanical means to prevent deep vein thrombosis in hospitalised patients. Due to a theoretical concern about impairing blood flow, thromboembolic-deterrent stockings and IPC are considered contraindicated for patients with peripheral vascular diseases by some clinicians. This study assessed whether IPC would alter peripheral limb muscle tissue oxygenation (StO2), and whether such changes were different during 10 minutes of sequential and single-compartment compressions. Twenty volunteers were randomised to have their left or right arm treated with a sequential or single-compartment IPC for 10 minutes, using the contralateral arm without compression as an intraparticipant control. After a five-minute wash-out period, the procedure was repeated on the same arm using the alternative mode of IPC. Both hands’ thenar muscles StO2 was monitored every two minutes for 10 minutes using the same near-infrared spectroscopy StO2 monitor. Both sequential (3.5%, 95% confidence intervals (CI) 2.7–4.2; p < 0.001) and single-compartment IPC (1.6%, 95% CI 0.4–2.8; p = 0.039) significantly increased muscle StO2 within 10 minutes compared to no compression; and the increments were higher during sequential compressions compared to during single-compartment compressions (2.1%, 95% CI 0.7–3.5; p = 0.023). This mechanistic study showed that both modes of IPC increased upper limb muscle StO2 compared to no compression, but the StO2 increments were higher with the multiple-chamber sequential compressions mode. Contrary to the theoretical concern that IPC may impair peripheral limb tissue oxygenation, our results showed that IPC actually increases oxygenation of the peripheral limb muscles, especially during the sequential compressions mode.
Introduction
Venous thromboembolism (VTE)—including deep vein thrombosis (DVT) and pulmonary embolism (PE)—is one of the most preventable causes of death and morbidity in hospitalised patients.1,2 In 2008, VTE accounted for more than 14,000 hospitalisations (or 70 per 100,000) and 5000 deaths in Australia. 3 And according to the New South Wales (NSW) Clinical Excellence Commission, a large number of hospital-associated VTEs (n = 2229) including fatal PEs were identified in 2012 and 2013.
The incidence of asymptomatic VTE, including PE, in critically ill or injured patients is very high despite anticoagulant prophylaxis. 4 In one cohort study, up to 10% of the patients already had unsuspected DVT at the time of intensive care unit admission. 5 Although anticoagulant prophylaxis remains a gold standard in preventing VTE, many clinicians perceive the risk of bleeding as more important than the risk of VTE, leading to a delay or even omission of VTE prophylaxis in a significant proportion of patients.6–8 Observational studies have suggested that a delay of more than one to three days in initiating VTE prophylaxis is associated with a threefold increased risk of VTE and possibly also mortality in critically ill and injured patients.9–12
Mechanical VTE prophylaxis, such as intermittent pneumatic compression (IPC), has the advantage of not inducing bleeding, and can be initiated as part of a multimodal approach to reduce risk of VTE for many critically injured or ill patients who are at risk of bleeding.13,14 Evidence suggests that IPC of the lower limbs, either alone or in combination with anticoagulant prophylaxis, is a cost-effective means to prevent VTE in a wide range of hospitalised patients.15–17 Nonetheless, peripheral vascular disease and surgical- or trauma-related leg wounds are often considered as contraindications to all forms of mechanical VTE prophylaxis, 18 assuming both IPC and thromboembolic-deterrent stockings (TEDS) would impair peripheral limb blood flow and wound healing. This hypothetical concern has resulted in discrepancies among different guidelines on whom, and when, an IPC is contraindicated among those with a leg wound, 19 despite an absence of evidence to suggest that IPC may compromise peripheral limb blood flow in those with peripheral vascular diseases.20–23 Underutilisation of IPC in patients with leg wounds in the critical care unit including those who have a coronary artery bypass surgery (CABG) vein-graft harvest wound in the legs is common. And this may, in part, explain why the leg with the great saphenous vein donor wound carries a higher risk of DVT compared to the leg without the wound after CABG. 24
Most IPC devices use brief cycles of pneumatic pressure below diastolic blood pressure to minimise venous stasis. Sequential compressions of the calf have been shown to increase femoral venous blood flow velocity similar to that achieved during ambulation. 25 In two small, before-and-after design, healthy volunteer studies (n = 8 and n = 14 including males only), IPC appeared to be capable of increasing tissue oxygenation.26,27 Whether such improvements were due to a higher cardiac output from an improvement in venous return, regional peripheral limb blood flow or venous tone is uncertain. 28 In addition, whether a multichamber IPC device—with sequential compressions starting from the distal part of the limb before compressing the proximal part of the limb—will have different effects on tissue oxygenation compared to a simple single-compartment compression IPC has also not been thoroughly investigated. 29
We hypothesised that (a) IPC will increase regional tissue oxygenation compared to no IPC; and (b) because of sequential centripetal compressive motions, a multiple-chamber sequential compressions mode IPC (Kendall Co, Mansfield, MA, USA) may increase tissue oxygenation more than a single-compartment mode IPC (Flowtron Universal, Huntleigh Healthcare, Manalapan, NJ, USA).
Methods
Participants and study procedures
After obtaining approval from the Royal Perth Hospital Ethics Committee (RGS0000000641; Australian and New Zealand Clinical Trials Registry: ACTRN12618000710224) and written informed consent, 20 adult volunteers with age more than 18 years were recruited into this intraparticipant, randomised, controlled trial (RCT). Volunteers with severe underlying coagulation derangement who may develop bruises easily with pneumatic compressions or those with upper limb neuropathic pain were excluded. Because IPC is not contraindicated in patients with underlying cardiopulmonary, neurological or mild peripheral vascular diseases, individuals with such diseases were considered eligible for enrolment.
In this study, we used the InSpectra tissue spectrometer (Hutchinson Technology, Hutchinson, MN, USA) to measure muscle tissue oxygenation (StO2). This device is a novel, noninvasive, haemodynamic monitor that utilises near-infrared spectroscopy (NIRS) technology to measure the proportion of oxygenated haemoglobin relative to total haemoglobin level in the tissue 30 and can provide continuous real-time peripheral StO2 data.31,32 Because the InSpectra reusable 15-mm probe can measure only thenar muscles’ StO2, not foot muscles’ tissue oxygenation, in this study we assessed the effects of IPC on the upper limbs instead of the lower limb tissue oxygenation.
After standard calibration the InSpectra StO2 probe was positioned on the participant’s hand to achieve the maximum tissue haemoglobin index (THI: a measurement that reflects the haemoglobin signal strength in the region of the microvascular bed sensed by the probe; >10 is considered as having an acceptable signal). Using the same InSpectra device, the StO2 of the thenar muscles in both hands (with and without IPC compressions) of the participants in an upright sitting position was monitored every two minutes for 10 minutes. Participants were randomised to have (a) their left or right arm to have the IPC, and (b) either the sequential or single-compartment IPC treatment first. The contralateral arm without IPC during the whole study period was used as an intraparticipant control. After a five-minute wash-out period, the procedure was repeated on the same arm using the alternative mode of IPC. The procedures of the study are described in Figure 1.
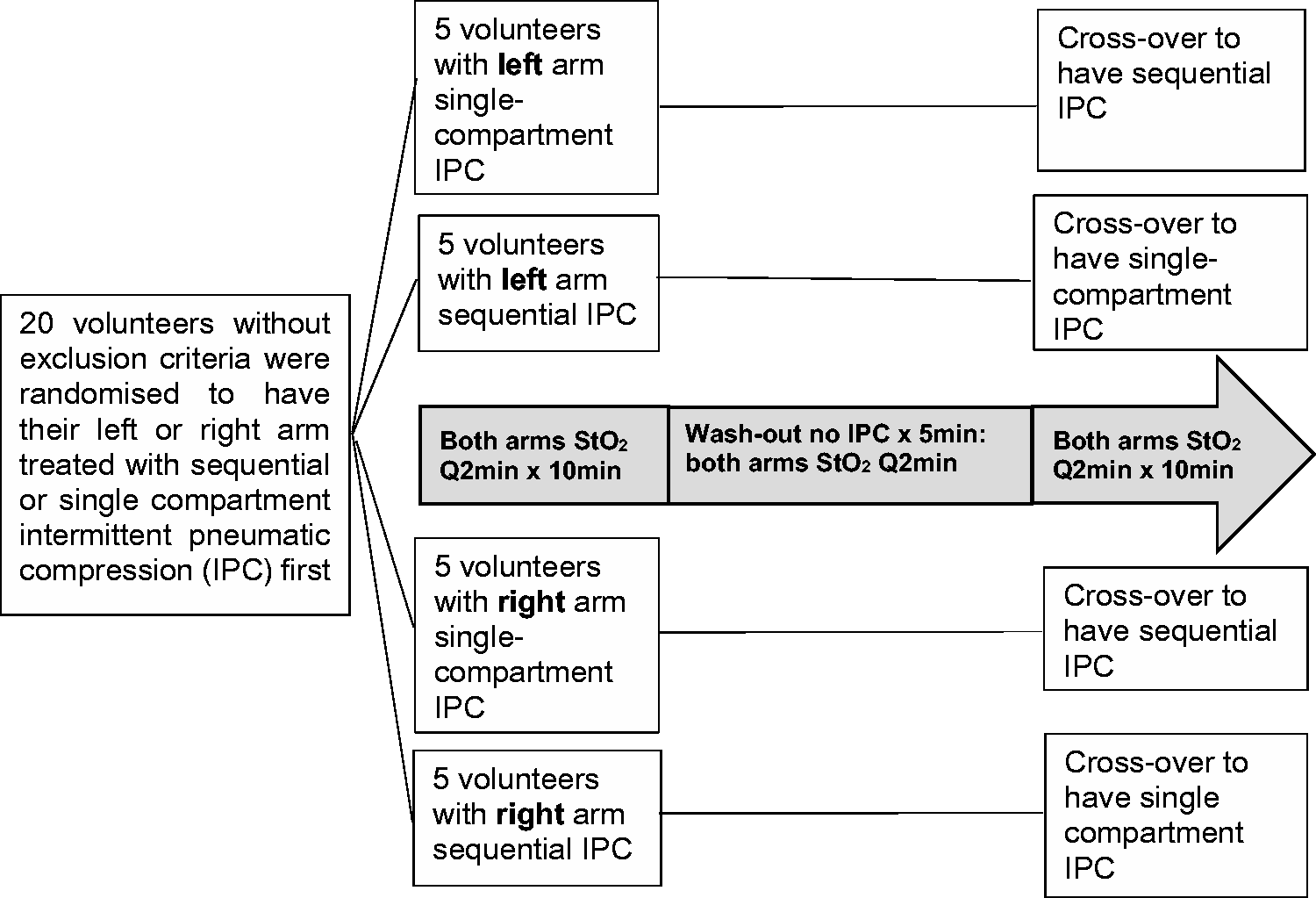
Flow chart showing the procedure of the randomised, controlled cross-over trial. min: minutes; StO2: tissue oxygenation.
IPC devices
The Kendall device and sleeves used for this study were provided by Cardinal Health, and the device uses a “Vascular Refill Detection” method to customise the therapy for each patient’s physiology. This system measures the time it takes for the veins in the limb to refill after having been compressed by the system. The time is then used in subsequent cycles as the time between compressions. Vascular Refill Detection occurs automatically and requires no operator interaction. The pressure inflated to the calf/leg sleeves is 30–45 mmHg and the inflation time is 12 seconds.
The intermittent pneumatic single-compartment compression device employed in this study is the standard IPC device used in the study centre. The single-compartment compression mode has a fixed 12-second inflation and 48-second deflation time with an inflation pressure of 40 mmHg. Both modes of IPC will keep running the inflating and deflating cycles indefinitely unless the device is turned off.
Sample size and statistical analysis plan
Using an intraparticipant design, our proposed sample size of 20 participants had >90% power to detect a 5% mean difference in StO2 between the IPC treated and untreated limbs and also between sequential and single-compartment IPC sleeves, assuming the standard deviation in StO2 is 2% 27 and correlation between left and right arm StO2 is 0.9 (derived from a trial run on four volunteers prior to commencement of the study).
Analysis of variance with repeated measures was used to compare StO2 values between IPC treated and untreated arms over time, and also between two types of IPC compression modes (similar to comparing the areas under the StO2 over time between the two treatment groups). Two-tailed paired t-test was also used to compare the differences between the baseline and the StO2 after 10 minutes of sequential and single-compartment IPC. Post hoc analysis for differences in StO2 at any other time points was not planned because of the small sample size of the study. All analyses were performed by MedCalc for Windows, version 17.9 (MedCalc Software, Ostend, Belgium) and an alpha-error <0.05 was taken as significant in this study. Raw data of the study will be provided on request to the authors.
Results
Twenty volunteers, five with some coexisting medical diseases, were recruited into the study (mean age = 31). The baseline THI (12.2, interquartile range 11.7–13.9) was satisfactory for all participants. The baseline blood pressure and THI were not significantly different between the left and right arms of the participants, and the StO2 between the two arms were highly correlated (Pearson correlation coefficient = 0.858). The mean baseline StO2 of the participants was 77.9%, which was slightly higher than previously reported on healthy volunteers (73.9%). 33 The characteristics of the 20 participants are described in detail in Table 1.
Characteristics of the participants (N = 20).
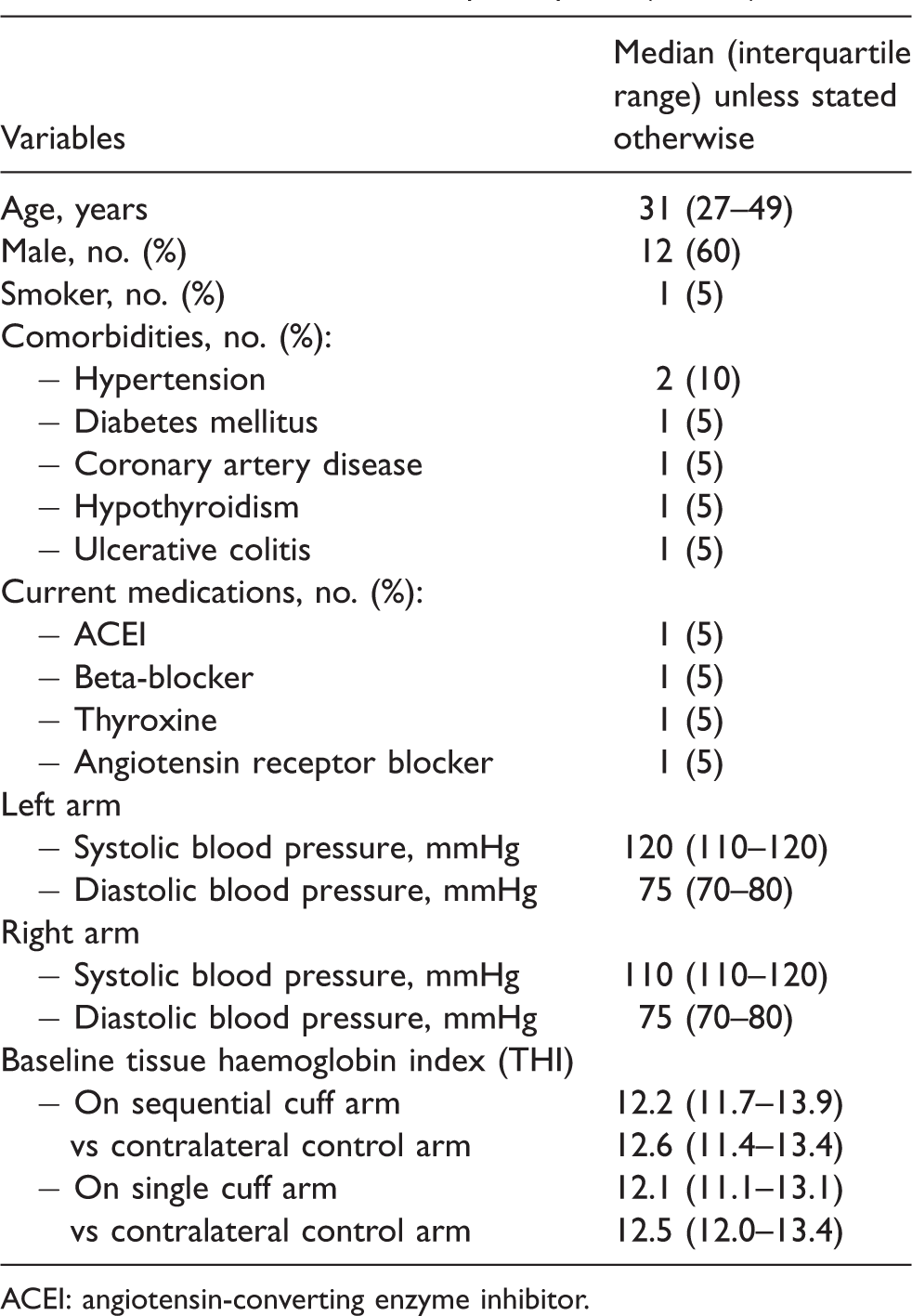
ACEI: angiotensin-converting enzyme inhibitor.
Muscle StO2 significantly improved within 10 minutes of both sequential compressions (3.5%, 95% confidence intervals (CI) 2.7–4.2; p < 0.001) (Figure 2) and single-compartment compressions (1.6%, 95% CI 0.4–2.8; p = 0.039) (Figure 3) compared to the contralateral upper limb without compression. Comparing to a single-compartment mode, the sequential compressions model was better both in its speed and magnitude of improvements in StO2 (2.1%, 95% CI 0.7–3.5; p = 0.023) (Table 2 and Figure 4).
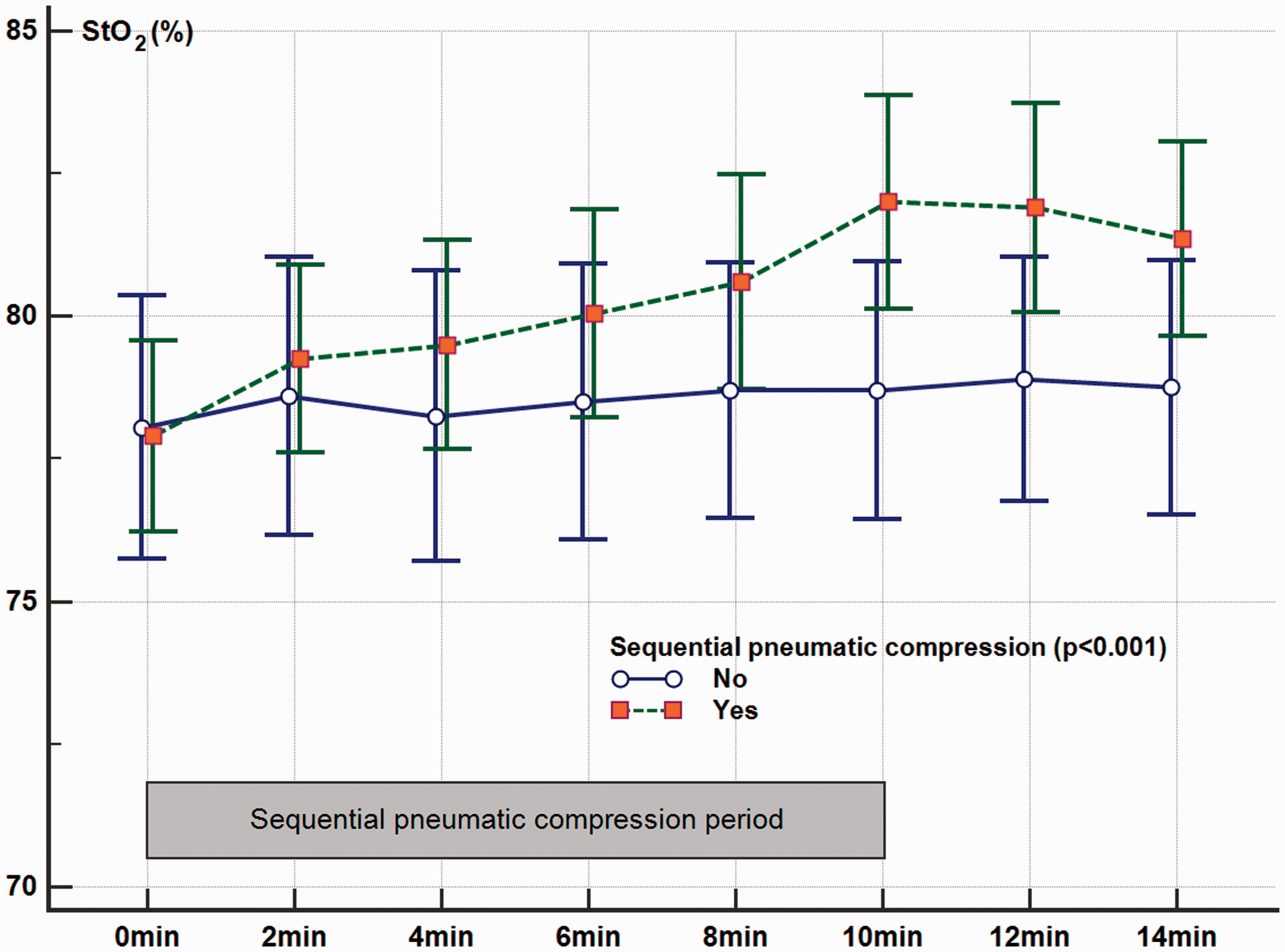
Changes in muscle tissue oxygenation (StO2) after 10 minutes (min) of intermittent pneumatic compressions using a sequential compressions mode.
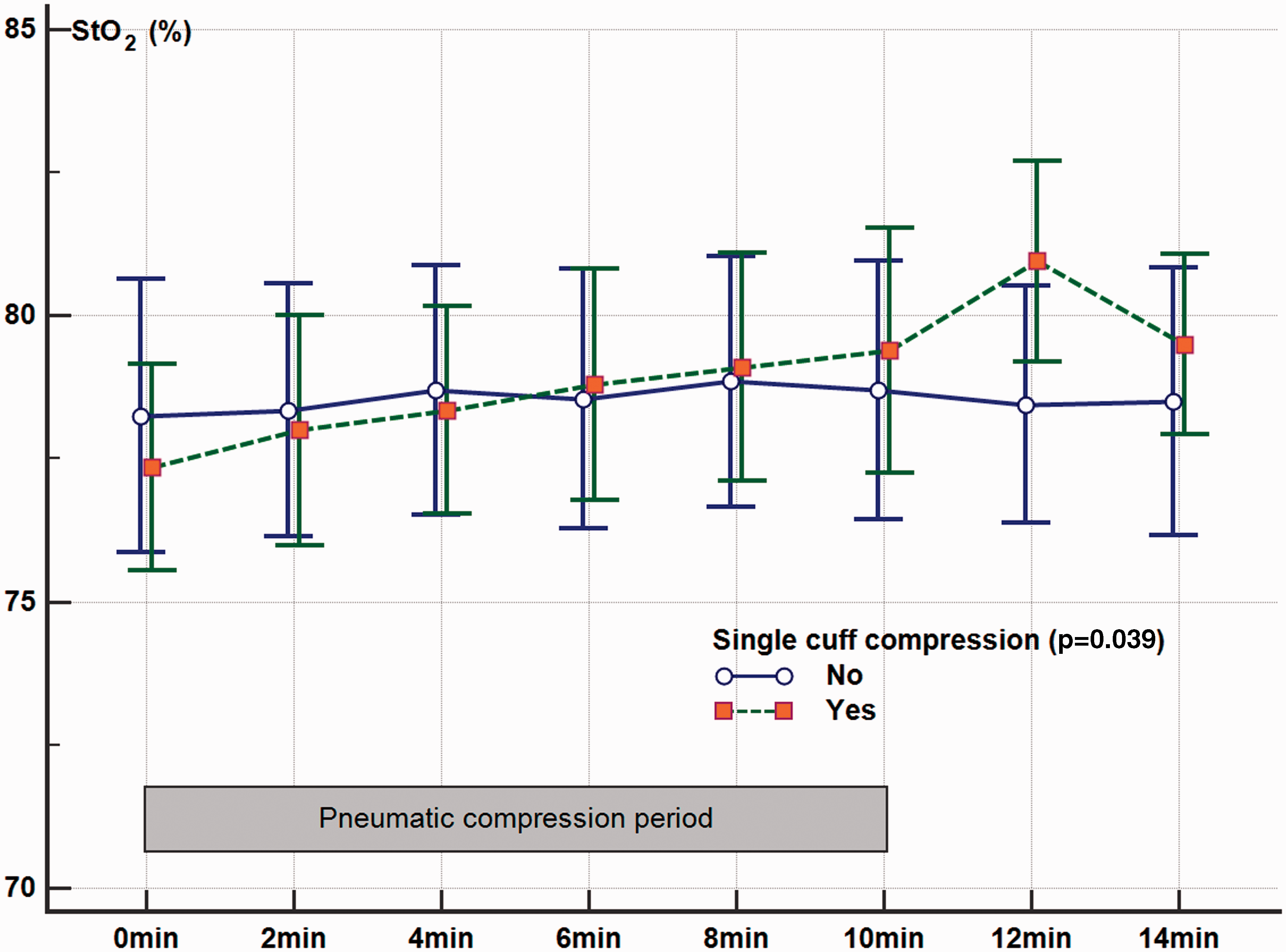
Changes in muscle tissue oxygenation (StO2) after 10 minutes (min) of intermittent pneumatic compressions using a single-compartment compression mode.
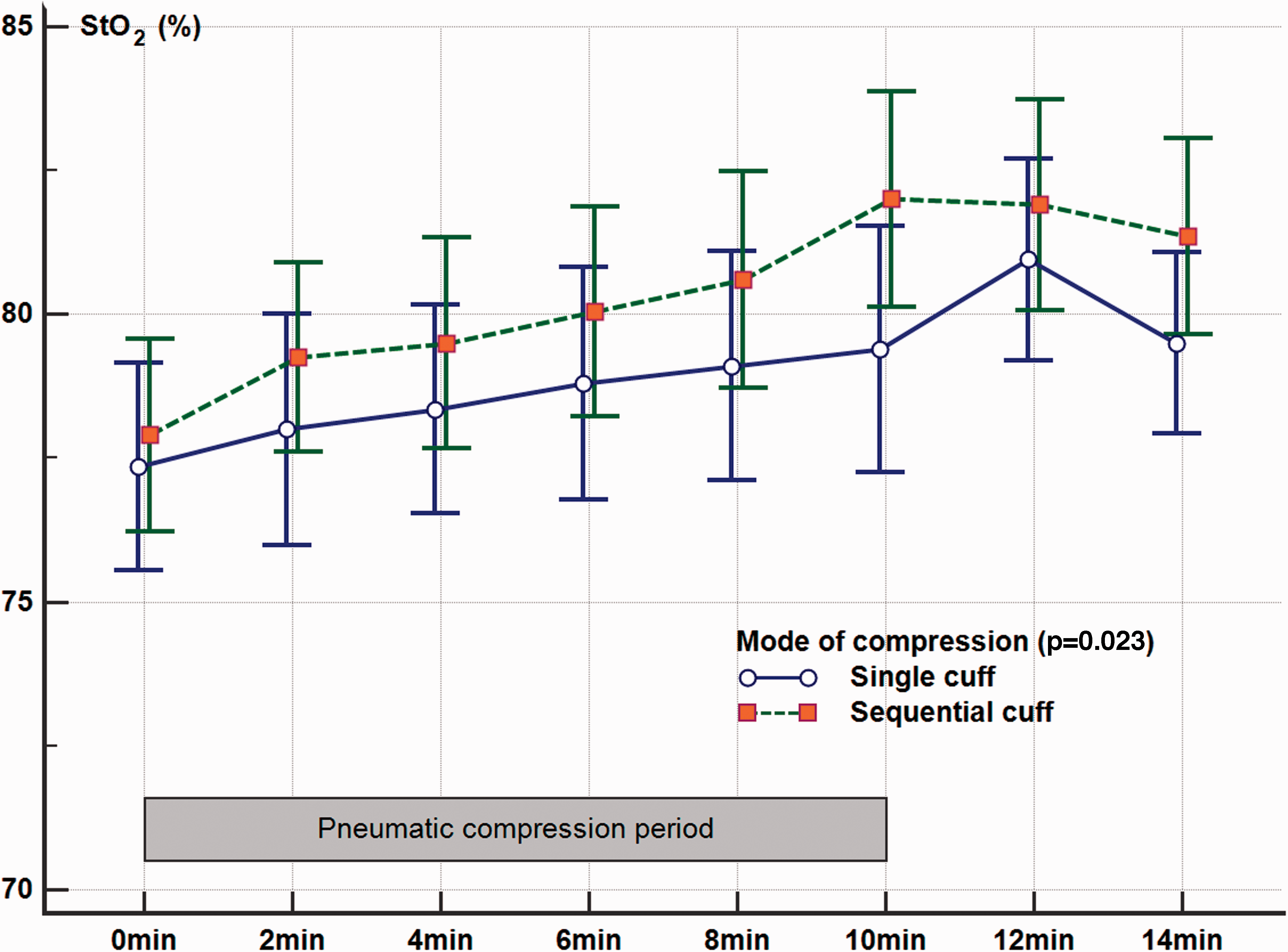
Changes in muscle tissue oxygenation (StO2) after 10 minutes (min) of intermittent pneumatic compressions single-compartment against the sequential compressions mode.
Comparing the differences in tissue oxygenation (%) between baseline and after 10 minutes of single-compartment, multiple-compartment sequential compressions or control with no compressions.
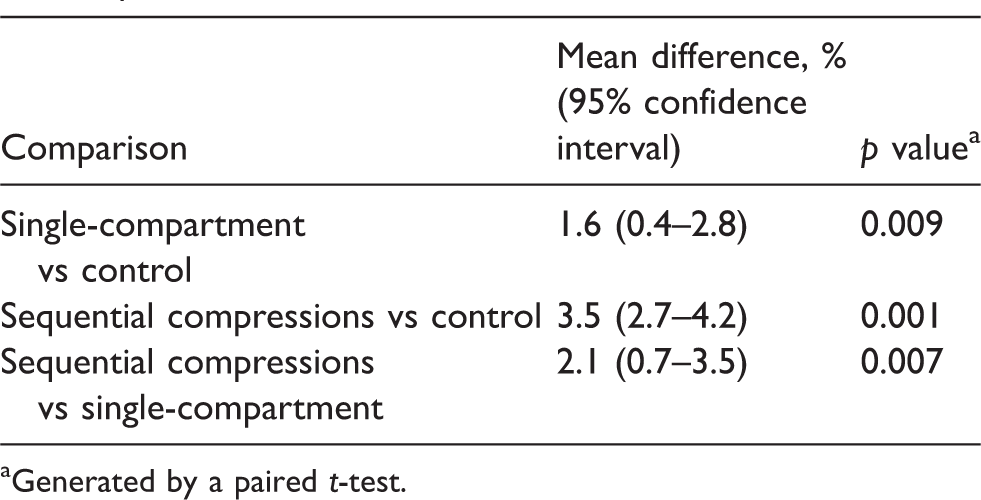
aGenerated by a paired t-test.
Discussion
This study showed that upper limb muscle StO2 improved significantly within 10 minutes of applying the IPC, and the sequential compressions mode improved the StO2 significantly more than the single-compartment IPC. These results have some clinical implications and require further discussion.
First, our study convincingly demonstrated that any improvement in the StO2 by IPC is confined to the limb where IPC is applied with little evidence on any improvement in the StO2 on the contralateral limb without the IPC treatment. Previous studies showed that StO2 was positively related to arterial blood flow and significantly reduced arm ischaemia when a tourniquet was applied.28,33,34 If there was an increase in the overall cardiac output state due to the use of IPC, we would expect that there would be StO2 improvements in the contralateral control limb during the study period. Second, although we studied the effect of IPC only on upper limb tissue oxygenation, we would expect the same responsiveness in the legs as in the arms. As such, our results are largely consistent with the reports of improvement in resting leg pain and healing of venous ulcers in patients with severe peripheral vascular diseases with IPC treatment.20–22
Third, multiple mechanical and biochemical mechanisms of IPC have been proposed. These include an increase in nitric oxide synthesis, prostacyclin, tissue plasminogen activator, tissue-factor pathway inhibitor as well as a simultaneous reduction in plasminogen activator inhibitor, venous pressure and interstitial tissue fluid. 35 Given the rapid changes in StO2 after the initiation of IPC, our findings suggest that the main mechanism of IPC to improve tissue oxygenation is most likely related to a mechanical effect on vascular tone and blood flow.29,36 Albeit still limited, our results provide a mechanistic reason to support the notion that IPC should not be, hypothetically, considered contraindicated in those with peripheral vascular disease or leg wounds, including those who have a great saphenous vein donor wound after CABG, 24 provided the IPC does not induce wound pain. Applying an IPC to the leg with a skin wound may indeed be beneficial in reducing DVT and possibly improving wound healing.20–22
Fourth, our results showed that sequential compressions would improve the StO2 better than single-compartment compressions. This may be because sequential compressions may empty the venous system more efficiently by compressing and emptying the veins distally first to fill the proximal venous system before this proximal part of the venous system is compressed and emptied. 28 In addition, the sequential compressions device customizes the compression cycle time by sensing the venous filling time and this may allow more venous compressions than the single-compartment device (which has a fixed cycling time of one minute) over the same period of time. Although IPC has a reasonably strong evidence base in reducing DVT and PE in a variety of hospitalised patients−either alone or in combination with anticoagulant prophylaxis−especially for patients at high risk of VTE,15,16,37,38 there is no high-level RCT evidence to suggest that a sequential compressions IPC device is more efficacious than a single-compartment device in reducing DVT/PE. 39 Because StO2 in the lower limbs had previously been demonstrated to correlate positively with regional blood flow measured by an ultrasound Doppler, 34 our results provide some rationale to support testing the hypothesis that a sequential compressions mode IPC is better than a single-compartment mode IPC in improving venous leg ulcers healing in patients with chronic leg ulcers 40 and reducing lower limb DVT.
Finally, we need to acknowledge the limitations of this study. Although we had recruited participants with cardiovascular diseases, none of them had confirmed peripheral vascular disease and hence the degree of improvements in StO2 by IPC in patients with established peripheral vascular disease may be different, and this requires further evaluation. Our results showed that the sequential compressions mode IPC improved StO2 better than the single-compartment IPC within 10 minutes, albeit the increments induced by both modes of IPC were small and of uncertain clinical significance. Because the inflation and deflation cycles in both modes of IPC will repeat indefinitely unless the device is turned off, it is uncertain whether the single-compartment IPC would eventually improve StO2 to the same extent as the sequential compressions mode after a long duration of IPC use. This is a mechanistic study; we made no attempt to assess patient-centred outcomes. Nonetheless, our results did provide a plausible mechanistic explanation for why IPC should not – at least hypothetically – be considered contraindicated as a mechanical means to prevent VTE in patients with peripheral vascular disease or leg wounds (unless it induces pain directly), and also why IPC may reduce VTE and improve leg ulcer healing in RCTs and observational studies.15,16,20–22,40,41
Conclusions
Contrary to the theoretical concern that IPC may impair peripheral limb tissue oxygenation, this mechanistic study showed that IPC increases limb muscle StO2 compared to no compression within 10 minutes, especially with the multiple-chamber sequential compressions. An adequately powered RCT is needed to confirm whether a sequential compressions mode will outperform a single-compartment mode IPC in improving patient-centred outcomes.
Footnotes
Acknowledgements
We would like to thank all the volunteers who participated in this study and Cardinal Health for providing the sequential compressions device for this study (Cardinal Health had no access to the study data or any role in the design of the study, analysis of the data or publication of the results).
This study was conducted at the Department of Intensive Care Medicine, Royal Perth Hospital. The results of this study were presented at the College of Intensive Care Medicine of Australia and New Zealand Annual Scientific Meeting in Hobart, Tasmania, 26 May 2018.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded internally by the Department of Intensive Care Medicine, Royal Perth Hospital. Dr Ho is funded by WA Health and Raine Medical Research Foundation through the Raine Clinical Research Fellowship. The InSpectra tissue spectrometer was funded by a research grant from the Medical Research Foundation of Royal Perth Hospital. The funding agencies played no role on initiation and design of the study or the interpretation of the results and the decision to publish. No funding was received from Cardinal Health or Flowtron Universal or other commercial companies for this study.