
Abstract
Marxist scholarship has documented the implications of ‘neoliberal’ reforms to public services. This scholarship often considers these reforms as class projects which have disciplined working populations and created new opportunities for capitalist profit-making. But in this article, we shift emphasis to the internal dysfunction that shapes states’ pursuit of market-oriented policy agendas. We place closer focus on the specific levers through which marketising reforms are implemented, noting the conflicting pressures they unleash, and the cracks this may open through which a more democratic agenda can be advanced. Taking the French hospital sector as an example, we show how attempts to expand and intensify competition in public services have coincided with attempts to decentralise governance to the regional level. While ostensibly part of the same ‘reforming’ policy agenda, marketising policies have a strongly centralising logic which has in practice undermined efforts to develop meaningful regional planning. These institutional tensions have catalysed new political currents, as the relationship between public authorities and private sector actors has become more overtly conflictual. We argue that Marxist theorists of the state need to pay closer attention to the often dysfunctional relationship between different branches of the state, and that in the context of neoliberal public service reform, the tensions between central and regional states are particularly salient. We conclude that opponents of the marketisation of public services need to pay attention to the contested and ambiguous nature of ‘decentralisation’: while it is often a rhetorical cover for marketisation, there are opportunities for the left in demanding more meaningful and authentic forms of regional planning.
Introduction
An extensive critical social science literature has documented ‘neoliberal’ transformations of state institutions, including the changing role of state actors in restructuring vital public services. We know much about how public sector workforces have been disorganised and disciplined by market-oriented reforms (Carter & Kline 2017; Lethbridge 2009); how this ‘class discipline’ has been exercised on wider populations (Umney et al. 2018); and how reforms have created space for commodification of essential services and their subordination to private profit (Blomgren & Sundén 2008; Moody 2011; Ruane 2001). We also have a growing understanding of how workers and publics may try to fight against these trends (Krachler & Greer 2015). This article, however, examines these transformations from a different angle. We want to study the kinds of organisational and institutional dysfunctions which can pervade ‘marketising’ policy packages. Specifically, our concern is with the ingrained tensions between the desire to ratchet up competition in service delivery, and concurrent moves to decentralise the administration of public services. While the latter has been identified as a rhetorical justification for marketisation, and indeed as a market mechanism in itself (Krachler et al. 2021), the objectives of marketisation and decentralisation can also be profoundly contradictory.
Hence, while decentralisation has frequently been presented as an urgent priority of public service reform, the position of regional actors within wider processes of public service marketisation is complex and contested. The role of regional state actors, while arguably under-examined in Marxist scholarship, is important for Marxist theorists of the state. This is because it points to the contradictions between different institutional branches of neoliberal state apparatuses (i.e. its local and central levels) which both shape the way in which marketising policy agendas play out in practice, and point towards tensions within them that are of strategic relevance to their opponents on the left.
Some evidence suggests that decentralisation and marketisation may be mutually complementary. For instance, in Germany, regional authorities have proven a vital enforcer for central government in ensuring closures and privatisations of public hospitals (André & Hermann 2009). Regional public authorities may be given new impetus by marketisation, where they are charged with stimulating competition between providers of public services (Hefetz & Warner 2004; Smith & Smyth 1996), shifting from a ‘steering’ to a ‘facilitative’ role (Galland 2012). Indeed, breaking up ‘monolithic’ central state organisations and ‘empowering’ local actors in public services has been a key rhetorical claim used in support of market-centric policymaking (Stewart & Walsh 1992).
By contrast, other studies show regional actors using their autonomy to frustrate rather than facilitate marketisation (Fredriksson & Winblad 2008; Schulte et al. 2018). They may have a more qualitative view on service delivery (Guerrero et al. 2009; Hughes et al. 2011), prioritising long-standing networks above market ‘openness’ (Christiansen 1998; Rhodes 1998; Schulte et al. 2018), and can be more susceptible to public mobilisations against marketisation (Krachler & Greer 2015). Marketisation may thus unleash tensions between regions and the centre, which in turn can result in further central intervention: for instance, to devise and enforce the frameworks through which organisational-level competition takes place (Bach 2000); to negotiate politically problematic outcomes of marketising policies (Cumming & Mays 2002; Tediosi et al. 2009); or to discipline regional actors that implement market-oriented policies unenthusiastically (Guerrero et al. 2009).
Hence, there is evidence that, particularly regarding public service functions, the neoliberal state features some significant internal tensions that require further investigation, and which may be important in understanding wider processes of liberalisation and market-centric reforms in developed capitalist states. Certainly, examining the contradictions and dysfunctions shaping political agency at the regional level has long been a priority within the policy literature (Atkinson 2002; Fredriksson & Winblad 2008; Krachler & Greer 2015). However, this is also a profoundly relevant question for left critics of marketisation. As Krachler and Greer (2015) have convincingly argued with regard to the British health system, marketisation is a politically fragile process which thrives on technocratic isolation, and when excessive political scrutiny (such as from unions or campaigning groups) is placed on it, it can prove surprisingly brittle. Hence, it is vital to study, understand and engage with the kinds of political and administrative tensions that are frequently thrown up between the centre and the regional in the wake of market-centric reform packages. Yet, while various analyses have critically evaluated the consequences of centrally driven marketisation policies in sectors such as healthcare (Castiel & Bréchat 2009; Izambert 2016; Moody 2011), the specific and sensitive question of centre–regional politics has been neglected.
We examine this issue through a case study of French hospital policy. This case is instructive because both decentralisation and marketisation have been important features of French hospital governance over the past 15 years. There has been increasing emphasis on ‘regionalisation’ or ‘territorialisation’ in French policy discourse (Codefy Lucas- & Gabrielli 2011; Tabuteau 2012). Concurrently, far-reaching measures have been taken to increase market competition within the sector (Albert-Cromarias & Dos Santos 2020; Izambert 2016). While some Francophone practitioner literature has identified a developing ‘paradox’ whereby the competitive logic imposed on hospitals has coincided with increasing supervision by the central government (Couty 2012; Romatet 2012), there has been little academic research examining how these dynamics intersect; still less so with a view to understanding the tensions between decentralisation and marketisation more generally.
In our case study, pressures towards marketisation corroded the ability of regional actors to meaningfully organise and coordinate public service delivery. Our data show two developments which help explain this. First, marketisation required various centralising measures that weakened regional-level institutional tools. For instance, where new frameworks for orchestrating competition were developed which needed to be designed and implemented centrally, thus preventing regional actors from initiating their own fiscal interventions. Second, the process of marketisation exacerbated tensions between regional planners and the large French private health sector, weakening the coherence of regional systems and generating conflict between actors within them. In examining these tensions, we develop the idea of ‘regional planning agency’. By this, we mean the ability of regional political authorities to coordinate the activities of organisational-level actors within their territory. We show how meaningful regional planning agency is threatened by the centralising impetus of marketisation, but we also suggest that making demands for meaningful regional planning is potentially a powerful way of opposing the market in healthcare. Hence, while the Marxist literature has generally prioritised focusing on ‘neoliberal’ reforms as a means of disciplining workers (Umney et al. 2018) or creating opportunities for profit extraction, there is strategically much to gain from focusing closely on its internal administrative and institutional frailties.
The article proceeds as follows. Our literature review examines international trends in hospital policy, placing particular focus on tensions between decentralisation and marketisation, and introducing the French context. After discussing the methods, the empirical material is organised into three sections. The first argues that regional planning, despite the creation of new actors with supposed augmented planning powers, remains stunted in France. The second shows how this partly reflects new centralising pressures unleashed by marketisation. The third examines shifts in the French private sector in response to marketization, which also undermines the role of public authorities at the regional level. Our conclusion reflects on lessons which can be drawn beyond the French case.
Regional planning agency and the neoliberal state
The existing literature shows that both marketisation and decentralisation have been important trends in ‘neoliberal’ public service restructuring across many countries, while also suggesting the need to disentangle the relationship between them. In this article we use the concept of regional planning agency to decipher this issue. In this section, we define this concept, and explain why we believe it is important for Marxist analyses of the neoliberal state. Our starting point is that while the empowerment of regional actors has often been presented as a complementary part of wider market-oriented policy packages (e.g. LeGrand 2006) (indeed, one ideological selling point of marketisation is its supposed reform of the ‘monolithic’ central state) the connection between these concepts is in fact often rather conflictual.
Marxist research has to date concentrated more heavily on one of these aspects (marketisation) than the other (decentralisation). There is much Marxist discussion of market-centric reforms to public services. Various aspects have been underlined. For some, market-centric reforms are part of a wider process of class discipline; in other words, attempts to disempower workers and render them more malleable at the hands of capital (Umney et al. 2018). For others, market reforms have been presented as an important way of creating new opportunities for capitalist profit (e.g. Moody 2011). Marxist theories of the state help explain why and how the interests of private healthcare enterprises and public healthcare managers have generally won out over the demands of healthcare workers in recent rounds of reform (Umney 2018). However, the tensions between region and centre in this context have been less frequently examined. As we will show, this is often a source of complexity and dysfunction which reveals fragilities in the attempts of neoliberal states to unleash and wield market forces.
With this article, we want to open up a line of inquiry into region–centre tensions, and their role in shaping the empirical trajectory of neoliberal states and their public service functions. While Marxists have often examined the imperatives which act on states, it is also important to consider that these imperatives play out differently across different branches of the state, and that these variations merit finer-grained analysis. Specifically, when it comes to public service delivery, evidence suggests that tensions between central and regional state actors are particularly salient. This is important for Marxists to consider conceptually (since it provides a new angle through which to consider the tensions which lie within that broad category of ‘the state’), but also strategically, because where these tensions emerge it can lead to institutional fragilities and hence opportunities for left campaigners. In the section which follows, we will pick apart these tensions in more detail.
To understand region–centre tensions, we must start by considering the ambiguity of terms like ‘decentralisation’; often serving an ideological purpose as a justificatory principle for marketising reforms (Krachler et al. 2021). Decentralisation has various aspects in the policy literature, often distinguished between ‘administrative’, ‘political’ and ‘fiscal’ types (Alonso et al. 2015). Here, we also use the term ‘regional planning agency’, as a separate but closely related concept. By this term, we mean the capacity of regional-level policy actors to orient the behaviour of organisational-level actors (such as, in our case study, hospital management) within their territories according to their own defined objectives.
Defined thus, regional planning agency has an ambivalent relationship with different forms of decentralisation. It is clearly different from (and arguably mutually exclusive with) ‘administrative decentralisation’, which describes the increased power of organisational-level managers vis-à-vis regional and national-level authorities (Bach 2000). It bears more resemblance to political decentralisation (i.e. the devolution of policy decision-making) but does not necessarily imply a local electoral mandate. Meanwhile fiscal decentralisation (Saltman & Bankauskaite 2006), denoting the ability of regional actors to raise revenue and devise expenditure plans independently, is not synonymous with regional planning but may conceivably be a necessary condition for it. Regional planning also differs from ‘deconcentration’, where regional actors serve merely as local branches of the central government.
The concept of regional planning agency is something which, we argue, should be more prominent in Marxist analyses of the state and public services. It provides a useful lens through which to examine ongoing processes of neoliberal restructuring. Central governments have played an increasingly aggressive role in restructuring public services, and the regional level has often been interpellated as a lever for enforcing this agenda, which in turn makes it an important subject for Marxists. One example of this principle in healthcare is the UK Health and Social Care Act implemented by the 2010–2015 Coalition government, which established local commissioning institutions as a key mechanism for the outsourcing of many services. However, while Marxist analyses of the neoliberal state provide an explanation for the ‘why’ of this development (for instance, the imperative to reduce public expenditure; create opportunities for profitable investment; and discipline public sector workers), a focus on regional planning agency is necessary for understanding the empirical reality of the process. For Marxist state theory, the most important insight we want to underline is that regional actors cannot simply be used as institutional mechanisms in this way. They are subject to their own imperatives and pressures which often conflict with those of the centre. Consequently, attempts by neoliberal central states to drive through reforms via the regional level are both increasingly common and often very troubled and incoherent in practice. Hence a Marxist analysis of the neoliberal state is incomplete without some attention to regional planning agency.
The concept of regional planning agency is also important for Marxists because it may help diagnose fractures within state edifices. Indeed, with this in mind, could it be a source of left optimism, or at least a rallying point for the radical left? Increasingly, radical left politics has identified local planning initiatives as potential sources of hope in an unremittingly hostile political climate. This is evident, for instance, in discussion of innovations like anchor institutions, as an alternative means of organising service provision at the local level (and a pillar of the Corbynite intellectual and policy agenda in the United Kingdom) (O’Neill 2016). Clearly, such experiments are rare. More often, as in our case study, regional authorities are not radical or transformatory forces. However, it is important to recognise that the demand for meaningful regional planning agency can act as a rebuke to marketisation, and as a potentially effective lightning rod for popular opposition to it. But realising this requires the intellectual task of examining the tensions between marketisation and regional planning in finer detail. This is the aim of the next section, and the empirical material which follows.
Decentralisation, regional planning and marketisation
By ‘marketisation’, we refer to transnational trends towards stimulating increased competition in the delivery of public services (Greer & Umney forthcoming). Marketisation is in part driven by the desire to cut public spending and to retrench the influence of centralised public service providers (André & Hermann 2009; Klenk 2016). Private sector consolidation has intensified this impetus, with emerging multinationals viewing public services as an attractive receptacle for investment (André & Hermann 2009; Greer et al. 2017; Ruane 2001). A marketisation-oriented policy agenda implies that policymakers should seek to facilitate this process by defining new frameworks for organising competition between public and private actors. This has been an influential approach across many European countries over the past 20 years, in various social policy domains (Greer et al. 2017; Krachler & Greer 2015; Umney et al. 2018).
Having defined marketisation and regional planning agency, we ask our central question: how do these two phenomena interact? Put more specifically, what happens to regional planning agency in a context of radical shifts towards marketisation? This is a complex question, where conflicting evidence emerges.
Regional planning agency might, in some cases, facilitate marketisation. Indeed, the notion of local empowerment has sometimes been recruited as a rhetorical justification for marketisation, especially when juxtaposed with ‘monolithic’ (thus inefficient) public service providers (Stewart & Walsh 1992). For instance, in Germany, the empowerment of regional actors has encouraged them to act as frontline enforcers of privatisations (André & Hermann 2009). The creation of local commissioning institutions, as in the United Kingdom, supposedly combines the goals of bringing decision-making closer to the local level and expanding market competition in service delivery (Arrowsmith & Sisson 2002; LeGrand 2006; Moody 2011). Within this, contracting is a particularly important tool, ostensibly giving regional actors the means to design specifications reflecting their own objectives which can then constitute the basis for competitive markets (Hefetz & Warner 2004; Smith & Smyth 1996). This idea was particularly pronounced in initiatives like the UK government’s National Health Service (NHS) reforms of 2011, which sought to use local commissioning as the main lever through which to increase competition and encourage private sector involvement in service delivery (Krachler & Greer 2015; Moody 2011). These instances can be set in a context where theoretical understandings of regional state actors have shifted substantially, in which facilitating economic competitiveness is prioritised over social welfare functions (Galland 2012). This suggests that, at least from one perspective, decentralisation and marketisation could be viewed as interlinked aspects of a more diffuse agenda for public services; one of neoliberal class discipline (Greer & Umney forthcoming).
By contrast, other research casts doubt on this co-development of marketisation and regional planning agency. Some evidence suggests that marketisation advances a primarily ‘administrative’ form of decentralisation which could marginalise regional policy actors. This evidence is particularly sharp in the literature on healthcare policy. Many hospital systems have implemented Diagnosis-Related Group (DRG) financing, whereby conditions and procedures are sorted into standardised categories with defined costs attached. These systems incentivise individual hospitals to increase patient turnaround (O’Reilly et al. 2012), at the risk of falling into deficit (Antioch & Walsh 2004; Castiel & Bréchat 2009). Such changes encourage organisational-level managers to take charge over their own budgets (O’Reilly et al. 2012), empowering them to introduce new performance management techniques (Bach & Kolins Givan 2011) and compete against other establishments. In such cases, the centre defines a framework to enshrine organisational-level competition, threatening to squeeze out planning agency at the regional level (Bach 2000). Böhm et al. (2013) argue that market and central state actors often expand in tandem in healthcare systems, as governments lose confidence in non-profit actors to contain costs.
Hence, while much Marxist and other critical literature has criticised the deleterious consequences of marketising public service reforms for workers and service users (Carter & Kline 2017; Greer et al. 2017; Lethbridge 2009), or underlined the class character of such reforms (Moody 2011; Umney et al. 2018), we should also pay attention to the tensions, even dysfunctions, these developments unleash in the relationship between the central and regional state. The former may exert influence to compensate for local political sensitivities caused by marketisation’s inegalitarian consequences (Cumming & Mays 2002; Tediosi et al. 2009). The centre’s role may also be more explicitly directive, asserting authority over regional actors who appear insufficiently enthusiastic in encouraging private provision (Guerrero et al. 2009; Hughes et al. 2011), or through developing competitive contracting arrangements independently of regions (Smith & Smyth 1996). Mandates to develop competitive contracting can thus constrain regional actors’ political role (Armingeon 2007; Smith 2000), and disrupt the embedded relationships and networks upon which they may draw (Rhodes 1998). Conversely, reasserting the autonomy of regional actors to implement policy as they see fit can constitute a powerful brake on centrally driven marketisation (Schulte et al. 2018).
Hence regional planning agency might be enlisted to drive through marketisation policies, but may also be menaced by them, making it a contested and politicised terrain (Atkinson 2002; Fredriksson & Winblad 2008; Krachler & Greer 2015). This is particularly so where there is fuzziness surrounding regional authorities’ role. Ambiguities in centrally imposed marketising frameworks may be a means through which regional planners can assert their own priorities and support their own networks (Fredriksson & Winblad 2008; Guerrero et al. 2009; Hughes et al. 2011; Schulte et al. 2018). Hence areas of indeterminacy within marketising policy packages can enable continued local agency, a point which is likely to be important in understanding the relationship between central and regional state actors.
What, then, happens to regional planning agency in a context of the marketisation of public services? Hospital policy is an instructive lens through which to address this question. This is because marketising trends in hospital policy have been concurrent with important debates around decentralisation. The latter are often connected to evolving public health needs. Ageing populations necessitate continuous and coordinated care encompassing multiple types of health provision, rather than relying on discrete episodes of hospitalisation (Bodenheimer et al. 2009; Epping-Jordan et al. 2004). Moreover, the danger of fragmentation between different parts of health systems is also underlined by the COVID-19 pandemic (Chandra & Chandra 2020). The need for care to be coordinated more responsively at the local level has therefore engendered growing concern with decentralisation and regional planning in hospital systems. Hence, in healthcare, the theoretical tensions between marketisation and regional agency as competing state imperatives are rendered particularly vividly. In the next section, we briefly contextualise our case study.
The French hospital system
France’s hospital system is not always well understood in Anglophone literature, but offers an interesting case for examining the relationship between regional planning and marketisation. This is because of the intensity of marketising policy shifts dating back the Sarkozy presidency, and the way in which these coincided with a pronounced discourse around regionalisation. French public administration has been undergoing a protracted and uneven process of decentralisation since the 1980s (Genieys & Smyrl 2008), with the state shifting gradually towards a market-facilitating role (Schmidt 1999). However, the French hospital system has already had a comparatively large private sector since World War Two. There has historically been a relatively settled division of labour between the public and private sectors, with little direct competition for market segments. Much primary care is private, and private hospital provision predominates where discrete procedures are more appropriate than ongoing hospitalisation (Morel 2019). The post-War private sector was dominated by an artisanal model, with small, independent clinics typically run by owner-operator clinicians (Durousset 2010).
Hence central governance in the French hospital system is fragmented. It has extensive oversight over public hospitals, but few institutional tools in relation to the private sector. Consequently, it is sometimes accused of hospitalocentrism (Bourret & Salzano 2006), a pejorative term implying weak coordination between different components of the system; particularly between public and private branches (Delas 2011). This has made it difficult for regional authorities to effectively plan the supply of healthcare, particularly in terms of ensuring effective coordination between different actors within health systems who may be more apt to compete than cooperate. More broadly, this point is an important component of the Marxist critique of capitalist healthcare (Chandra & Chandra 2020). The intensifying policy preoccupation with ‘régionalisation’ or ‘territorialisation’ (Codefy & Lucas-Gabrielli 2011; Tabuteau 2012) reflects concern about this lack of coordination (though of course rarely informed by Marxist theory!), and the hope that more unified leadership can be fostered through regional actors. New institutions have been created to further this regionalisation, which are examined below.
France is an important case because over the same period it has also rapidly marketised hospital financing. DRG methods were pushed strongly under the Sarkozy presidency: as of 2007, the (near) entirety of French hospital budgets are determined under the Tarification à l’Activité (T2A) system. In international perspective, this was a comparatively sudden and radical extension of DRG financing (Castiel & Bréchat 2009; Izambert 2016), though the Macron government has proposed reducing this in future (we return to this point in the conclusion). Like DRG systems elsewhere, T2A implies a market-facing hospital, responsible for increasing revenue by accelerating patient turnaround. It has been accompanied by an intensifying discourse of the ‘entrepreneurial hospital’ (Couty 2010; Minvielle 2006) and the ‘patient as consumer’ (Batifoulier et al. 2008). Other marketising shifts include the Loi Bachelot of 2009, which sought to enable certain public service missions to be undertaken by private actors (Couty 2010), though these measures were diluted under the Hollande Presidency.
Finally, marketisation has also been pushed through public budget reductions which have ostensibly bolstered the private sector. While France retains comparatively high levels of health spending (OECD 2015), significant cost constraints have been imposed, particularly through measures like the non-replacement of hospital staff (Audier et al. 2012). Cost pressures have driven the closure of many small public hospitals and their consolidation into larger units (Dupont 2012). Regional state actors have been intimately involved in this process, but in a sometimes ambiguous way.
Hence, in France, attempts to foster regional planning coincide with strong marketising shifts, making it a good lens through which to view our theoretical questions. In our data, we consider what the French case can tell us about the institutional dysfunctions of public service marketisation.
Method
Our case study data are drawn from qualitative semi-structured interviews, following a key informant approach. Rather than attempting to gather a representative selection of a target group, key informant interviewing emphasises the pursuit of specialised knowledge (Marshall 1996). This suits a study which attempts to understand a broad policy landscape such as French hospitals, featuring complex and changing developments. Selecting a particular occupational group within the sector – such as managers, staff or public administrators – risked a more limited and partial perspective. Instead, our objective was to locate respondents occupying diverse positions in the French hospital system, who were well-placed to provide credible testimony. Documentary evidence, collated via Internet searches, was used to corroborate what interviewees had stated and to complete case data (Taylor et al. 2015). These included local news articles, trade union pamphlets, minutes of local meetings and government official reports and publications.
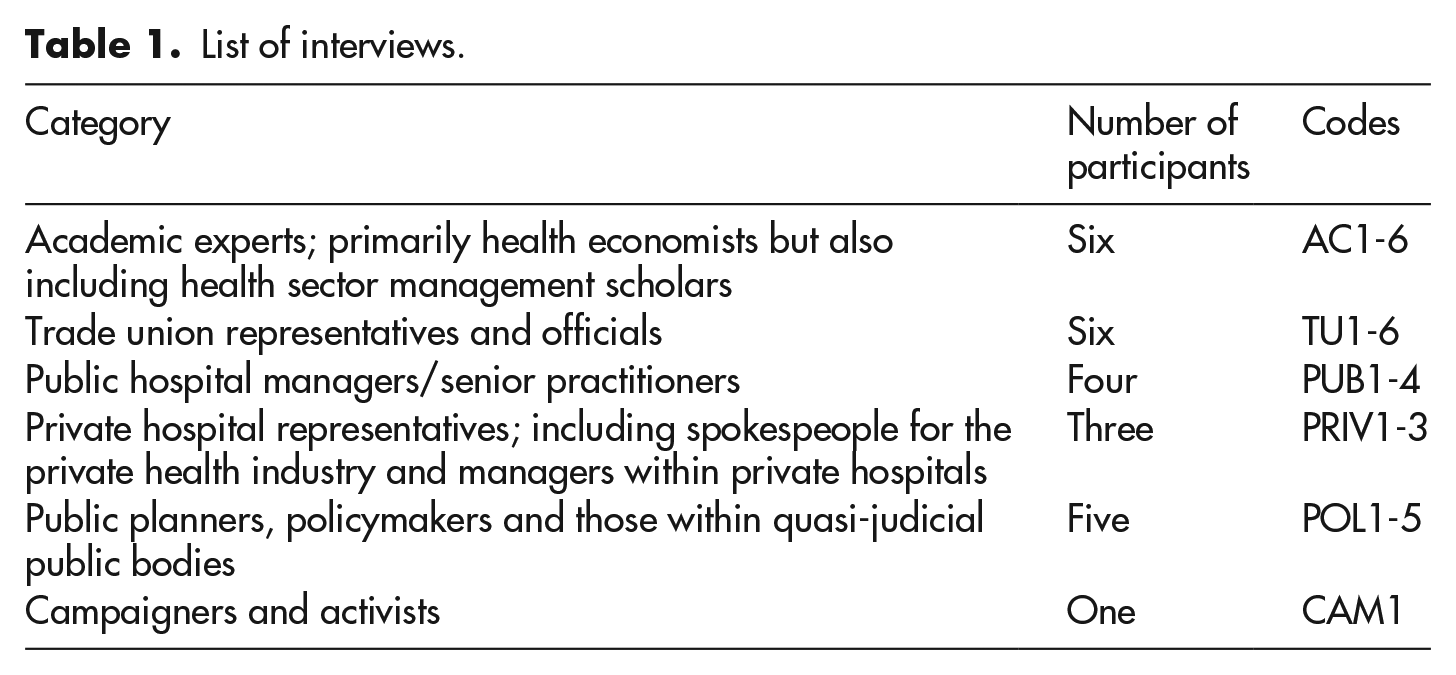
A range of key informants were contacted and 25 participants took part (Table 1). Interviews with French academic experts were first sought as a means of contextualising the sector and gaining a basic understanding of key developments. Introductory conversations with academic colleagues enabled us to ask foundational questions and seek clarification on empirical issues in a way that could side-track practitioner interviewees. Initially, our focus was primarily on ‘marketisation’: specifically, understanding the types of market-centric policy that had been introduced in France, and their implications for work and service provision in hospitals. Initial interviews were therefore only loosely structured, oriented towards gaining an up-to-date understanding of macro-level policy developments.
List of interviews.
Interviews were conducted and transcribed in French, before being coded using qualitative data analysis software, and detailed memos were written summarising the key points. These memos were in English and included the authors’ own English-language translations of key quotes. They were shared around the research team that would discuss each interview as they were accrued. During this process, we identified decentralisation and regional planning as an important emerging theme from initial interviews, particularly their complex interaction with our central topic, marketisation. Following this, we agreed that future interviews would include specific questions prompting participants to speak about this topic from various aspects, such as their perception of their interactions with regional agencies, and their perception of the changing role of regional planning. Where participants were officials within regional agencies themselves, we asked them in-depth questions about the evolution of their organisations and their role within them.
Hence, as data gathering developed, we progressed to interviewing a diverse set of participants from different professional backgrounds within the French hospital system. The underlying thread guiding sampling was participants’ concrete professional experience and knowledge of French hospitals. This included participants from policymaking circles, in hospital management (both in public and private sectors), from trade unionists and with representatives from private healthcare trade bodies (see Table 1).
As the theme of regional planning became more prominent, we moved beyond our initial concentration on Paris to examine cities in South-Eastern France, notably Marseille, Nice and Corsica. Paris was an inevitable starting point given its clustering of policymakers and researchers. However, it became apparent from documentary searches and interviews that these Southern regions were seeing more ‘experimentation’ with marketising policies at the regional level.
Because of the situation of the participants, many of whom held senior positions within organisation providing vital functions often under intense time pressure, access was challenging. Moreover, owing to the diverse occupations and locations of interviewees sought, strategies such as snowball sampling were impractical. We relied on using various ‘cold’ approaches. We would use our developing knowledge of the French hospital system to identify the kinds of position that would yield reliable and valid information, and use telephone, email or post to secure introductions leading to scheduled interviews. Interviews were conducted by the authors between 2015 and 2016 and normally lasted 1–2 hours. This process continued until saturation was reached: in other words, when our coding and detailed memos stopped yielding new themes and instead corroborated existing insights. The research received ethical approval from the University Research ethics committee. Participants were advised of the aim of the research and written consent was obtained prior to the interviews.
Data analysis in key informant research can be complex, particularly when interviewees are likely to have contrasting views and experiences. Moreover, in a diverse list of key informants, any given participant is likely to have areas of stronger and weaker understanding (Poggie 1972). The key informant interviewer must consider whose testimony is more reliable on a given topic. As such, as well as prompting interviewees to reflect on the central themes of the research, we also asked many specific questions in order to clarify and corroborate points of detail. We would then compare notes among ourselves to check our grasp of technical concepts and policy changes, making notes to raise further points of clarification in future where necessary. Moreover, in a politically contested setting such as the French hospitals sector, it is also likely that key informants may have differing normative interpretations of key developments. Extensive note-taking and coding of interview transcriptions identified key areas of disagreement between participants, and looking across the sample we constructed a nuanced picture, finding common empirical ground between different ideological perspectives. We also draw on Francophone scholarship and practitioner-oriented texts at various points to corroborate and contextualise our arguments.
Regional planning agency in the context of marketisation
In this section, we examine the creation of new regional agencies in the French hospital system, evaluating the powers they possessed and constraints on them. We will argue that regional planning agency remained stunted, despite a growing policy interest in ‘regionalisation’.
There was widespread agreement among interviewees that increased regional planning was desirable, even urgent, in order to overcome ‘hospitalocentrism’. Diverse interviewees argued that the fragmentation of the French hospital system was ill-adapted to meeting evolving public health needs, lacking coordination between heterogeneous local actors. The key institutional innovation of the Loi Bachelot was the Agences Régionales de Santé (ARS), which sought to address this problem. The ARSs were intended to have an extended regional planning mandate, with an emphasis on developing new cooperative links between organisational-level health providers, both public and private. They replaced the previous Agences Régionales de l’Hospitalisation, with the terminological change implying more extensive powers, including over private and charitable actors. Indeed, as we will show below, private sector actors portrayed the ARSs as ‘Jacobin’ assertions of French state power over private enterprise.
ARSs are charged with coordinating regional health supply. Aside from stimulating cooperation, they are also required to develop a schéma régional d’organisation des soins (SROS). This specifies objectives for regional health provision, which, in theory, should apply to all health providers. Such tools supposedly extend the reach of regional planning (though they are not ‘democratic’, since they have no electoral accountability to local populations). They amalgamate public and private health providers into a regional regulatory framework under the leadership of the ARS (interview, AC6). To pursue this objective, ARSs have hard and soft tools. The hardest tools are authorisations: they can approve or rescind any actor’s right to provide services in their territory. Softer tools relate to ‘contractualisation’: ARSs establish contrats pluriannuels d’objectifs et de moyennes (CPOMs), which are applied to every health provider, public or private. These are not contracts in the ‘Anglo-Saxon’ sense, but fuzzier agreements listing reciprocal commitments around various medical, financial and social indicators linked to wider regional objectives (interviews, POL2; POL3). Below, the nature and implications of this ‘contractualisation’ will be examined.
Despite these tools, we found that ARSs remain examples of deconcentration rather than regional planning. They are upwardly accountable to the central Ministry (interview, AC5). Their directors are named and dismissed by the centre, and tend to turnover rapidly (interview, POL2). They were often perceived by interviewees as subordinate to central priorities. More than one respondent described them as the ‘armed wing’ of the Ministry, channelling strategic and spending priorities directly from the government. ARSs, in practice, are conceived primarily as a means of adapting state directives to regional conditions. As one participant puts it, ‘the state develops an overall national policy and next each region must apply the regulations while adapting them as well as possible. And next, depending on the difficulties in the region, the state can help more actively’ (interview, POL3). Sometimes, ARSs may be skipped entirely where financial concerns are seen as sufficiently urgent. For instance, the development of a ‘return to financial equilibrium contract’ for the vast and in-deficit public hospital system in Marseille was set directly by the Ministry (interview, PUB3).
New policy tools assigned to ARSs were intended to enable them to oversee new forms of cooperation between actors, like groupements hospitalier de territoire (GHT), where public hospitals are consolidated into a smaller number of territorial centres. While there is a widely recognised policy rationale for improving coordination between local nodes of health systems, we observed that this consolidation process is closely tied to public sector retrenchment. One academic observer characterised the purpose of the ARSs as that of local actors to oversee public hospital closures (interview, AC2). Thus, our data suggest that ‘regional planning’ often appears primarily as the frontline implementer of centrally driven budget restrictions. This feeling was particularly intense in cities like Marseille and Nice, where the ARS had promoted the emergence of large new private hospitals to fill voids left by declining public provision.
ARSs do appear to have significant powers which go far beyond the public hospital, influencing private actors in a region as well. However, our findings suggest that they exercise these not as genuine regional planning actors but as deconcentrated actors subordinate to central objectives. They can authorise, or withhold authorisations from, any actor in their territory, over services provided and equipment used. Here, an ARS official describes their approach to authorisations, which applies to all actors, public and private: Every five years we re-examine the dossier, we may prolong the authorisation, or we may find we no longer need the service . . . [Then] we can retract the service authorisation, and the service will close. And similarly, if establishments want to buy a new scanner or IRM, they must ask us and we either authorise or don’t. Because we wouldn’t want them to make an investment when there is no need . . . (Interview, POL3)
This may, theoretically, enable them to orient the behaviour of public and private actors within their territory in quite a precise way. However, these tools may be exercised in an ad hoc fashion. In Marseille, management at a large private-non-profit hospital had felt able to avoid requests to pool resources with other actors with little fear of repercussions, and had maintained a large emergency room for decades despite shifting central policy over whether or not this intrudes on a supposed public monopoly (interview, PRIV2). In such cases, local arrangements are left undisturbed for the convenience of each party.
Hence in the private sector, ARSs have new institutional tools but we found little evidence of them intervening independently to reshape local provision. Meanwhile in the public sector, ARSs are merely one link in a system where authority has shifted upwards at each level: from ARS to state, hospital management to ARS and hospital staff to hospital management (Couty 2010). The ARS directly appoints public hospital directors, in whose role is concentrated increased CEO-type power (Couty 2010). Institutional counterbalances to hospital management have weakened since 2005, medical staff committees having shifted from negotiation to consultative roles, reducing staff voice (interview, TU2). Hospital directorates have assumed greater authority over finances and staffing, including the outsourcing of services. Hospitals have also been required to form pôles de santé, regrouping various services into connected faculties overseen by a chef de pôle who acts as line manager. These actors are in turn ‘contractualised’, following CPOM objectives (Bréchat et al. 2010): So you have a pyramidal system where the government names the director of the ARS . . . It names the director of the hospital under the advice of the ARS, the director of the hospital reports to the ARS and is fired by the ARS . . . and the director will name chefs de pôle who will report to him and he can dismiss them. (Interview, POL1)
In this context, ARSs have relatively little scope for regional planning agency. While they have enhanced power over the organisational-level in relation to both public and private providers, this is primarily in their capacity as a deconcentrated branch of the central state. They are one link in a chain in this respect, and can even be overlooked in certain circumstances where the state intervenes directly. In the next section, we argue that these weaknesses on the part of regional state planning are exacerbated by marketisation driven from the centre.
The effect of marketisation on the relationship between regional actors and the centre
The previous section noted how central pressures towards budget reductions weakened the prospects of regional planning, requiring ARSs to assume the role of local enforcers of privatisation. The need for central direction in pushing through the retrenchment of local services is one sense in which marketisation undermined regional planning from the top-down.
Another reason is that marketisation imposed new means of determining hospital budgets, intended to stimulate competition, which were designed centrally and left little space for regions to develop their own incentive systems. T2A constitutes ‘administrative decentralisation’ because it incentivises organisational-level managers to compete for financing. In the process it closes-off potential avenues of influence for ARS regional planning agency. Certainly, there have been attempts to nuance the French DRG system. By international standards, France’s list of DRG classifications is long (interview, PUB1), reflecting the division of conditions into degrees of severity. This severity scale is an attempt to recognise the public sector’s challenging case-mix, which is assumed to encompass patients with more complex needs (interview, AC4). However, this is a highly centrally driven form of nuance with little sense of adaptation according to regional priorities.
Consequently, Vincent (2012) argues explicitly that T2A reflects the desire to prevent ARSs from developing tailored regional financing systems. This reflects the centre’s fear that such decisions may prioritise the public sector, counteracting the general impetus of marketisation. As a result, ARSs are generally left with negative, rather than positive, policy tools. They can provide or refuse authorisations as reward or punishment for the delivery of existing services, but have few resources to stimulate new provision in areas that need it (interview, POL1). Thus, orchestrating inter-hospital competition has involved a centralised financing framework which leaves little scope for regions to use financial incentives to reshape provision in under-served areas.
Moreover, the competitive logic of T2A also undermines ARS objectives to stimulate cooperation. A private sector manager (interview, PRIV2) identified a ‘paradoxical instruction’ between ARS requests to cooperate, and the pressure on individual providers to increase their own patient traffic due to T2A. At the time of interview, his hospital had pursued virtually no cooperative links with others despite requests from the ARS. Others saw T2A as encouraging buck-passing and boomerang patients (interview, TU1), as hospitals emphasised their own turnover above coordination. Policy researchers argued that hospital directors had approached T2A with a ‘bad attitude’, calculating how to specialise in ‘profitable’ areas of provision leaving gaps elsewhere (interview, AC1; AC5). Hence, our data suggest that the centrally imposed T2A framework encouraged a more atomised approach among hospital management, which undermined ARS attempts to stimulate cooperative networks. The State capacity to plan at the regional level deteriorates, due to an increasingly constricting market framework imposed by the centre.
Nonetheless, regional planning agency has not simply been suffocated by marketisation. ARSs have scope to wield agency, but this lies in the ‘fuzziness’ of the developing institutional framework, which enables leeway. Guerrero et al. (2009) found that ARSs had adopted their own criteria for dispersing previous rounds of additional hospital spending (i.e. which supplemented existing T2A-derived budgets). While the centre had encouraged the use of quantifiable outcomes-contingent expenditure, ARS directors found ways in which to prioritise agreements with public recipients based on more qualitative priorities. This, in turn, led to intensified state guidelines being reissued, as the centre took firmer control over regional institutional space in pursuit of a more market-facing framework (see also Inspection Générale des Affaires Sociales (IGAS), 2013). While Guerrero et al. (2009) were studying a particular spending initiative, our data suggest the wider applicability of these insights to day-to-day ARS functioning. Tools such as the CPOMs are particularly fuzzy. They are essentially ‘a reciprocal engagement’ (interview, PRIV2), where the ARS takes the following line: We tell you to do that, that, that, and we check that your engagement is respected. And if you respect your engagements, the ARS will look after you. It will make it easy for you to get authorisations. And sometimes it will give you money. Voilà the spirit of the contract.
Hence ‘contracts’ are not specific and binding commercial arrangements, but looser sets of reciprocal commitments. They indicate . . . a document on which we write down what we expect from an establishment . . . It’s a formalisation of what we expect from an establishment, and it’s reciprocated . . . when we say to them ‘we will finance for you a mobile team for such and such’, we do it. (Interview, PUB2)
To some extent, these are ‘soft’ planning tools. There would typically be little financial penalty if these commitments were not respected and authorisations are very rarely withdrawn, though the prospect of being refused future authorisations was sometimes used as a stick (interview, PRIV2; POL3). ARS directors saw the imposition of legal sanctions (such as fines) as against the spirit of the ‘contract’ and likely to jeopardise relationships with other actors in the region, upon which local services may depend (interviews, POL3; POL2). However, the ARS has the agency to change or withdraw monetary commitments in future (interview, POL3), and will sometimes take further steps to stimulate actors’ behaviour: If we want to allocate a mission . . . the different actors and different clinics who want to be candidates, we will see who is the most appropriate . . . Often it’s because they’re the best situated, the most central, or the cheapest . . . If the money is correct [private clinics] will often want to volunteer. If it’s just about covering costs they will be less motivated but there we can also impose. We can force a clinic to develop a public service activity . . . we have authority over them. We try to make it so that it is voluntary. If they aren’t volunteering, we try to see how to make it so that their vision of the mission is improved, and if that still doesn’t work, we can use more force.
Hence in the fuzziness of ARS-led contracting there is some scope for discretion from ARS directors. Private sector actors have characterised this as illiberal and ‘Jacobin’: Alas, it’s the Agency that has to contract with the producer, saying ‘I want a contract, I am [authorising] you for this mission but I am controlling you on the mission and if you don’t do it, I will withdraw everything’ . . . For the private clinic, there is no choice. For example if they say to me in my hospital ‘you will welcome everyone without distinction’ and I refuse people who don’t have cover at all, the Agency says to me ‘it’s not just that that you will lose [one mission], you will lose everything, I am withdrawing the thing from you. (Interview, PRIV1)
The same interviewee had experience of working on outsourced contracts for the British NHS: I loved it. I learned a lot that year when I did that, because we had a true contractualisation. They said to us it’s 250 patients, it’s not 249 nor 251, it’s 250. It’s for such and such a price, and for such and such a service. Everything was written . . . [In France] they tell us to invest in our hospital . . . I build my maternity ward, I put down 50m euros . . . I borrow a lot to be able to do it and I say to the State, ‘what will you give me in return?’ They tell me nothing.
In his view, the private sector could be used as an ‘adjustment variable’ for in-deficit public hospitals, citing cases where profitable private hospitals had had authorisations withdrawn so as to direct more traffic to public ones. Sources of discretionary spending at the disposal of ARSs, such as Missions d'Intérêt Général et d'Aide à la Contractualisation (MIGAC) are more likely to end up in the public sector than the private (Piliu 2014). This may reflect affinities between ARS planners and public hospital directors, given that it is from the latter’s ranks that the former tend to emerge and with whom they often liaise informally (interviews, PUB3; PUB1). ARSs may also distribute discretionary grants annually, as a means of counteracting budgetary pressures caused by T2A (interview, PRIV2). However, these financial resources were generally perceived as being very small and of limited utility by interviewees (interviews, PUB2; AC4).
Hence the evolution of the ARSs role in a context of marketisation is complex. Key aspects of the developing institutional framework remained relatively fuzzy and this enabled ARS officials to wield some discretion, which in turn could run counter to the thrust of marketisation. They had scope for limited discretionary spending, which were generally of little significance as a portion of the overall budgets. However, these are sources of regional planning agency that persist despite marketisation, where the emerging institutional framework left scope for leeway. Marketisation itself unleashed centralising tendencies. It has required ARSs to enforce public sector retrenchment despite local opposition, and it has imposed centralised financing systems which undermine the capacity of regional actors to stimulate provision in needed areas, or engineer new forms of cooperation between providers. We have already intimated that these stirred up conflictual political currents surrounding hospital governance, and we explore this more directly in the following section.
The political role of regional planners and tensions with the private sector
The preceding section showed that marketisation unleashed centralising pressures that weakened regional planning agency, while noting that regional planning agency could be found where the rapidly developing institutional framework left areas of indeterminacy. In this section, we show how it also caused an increasingly conflictual relationship between regional planners and the private sector. These shifts threatened the coherence of local health systems, but also underline the potential potency of demands for meaningful regional planning as a response to centrally imposed marketisation.
From a comparatively large base, the private sector has struggled to extend its market share in France despite marketising legislation. Profits in the sector remain low (interview, PRIV1), and various interviewees testified that in areas such as obstetrics the public sector is itself gaining ground, as T2A has spurred it to become more ‘cost effective’.
As noted, fuzziness in ARS contracting systems had given rise to complaints about illiberalism from private actors, directed at regional planners. Despite these critiques, the same private voices also sympathised with ARS directors, describing them as ‘diplomats in an impossible situation’ who usually, even if simply through pragmatism, ended up on good terms with the private sector (interview, PRIV1). Because, in practice, they act as local representatives of the centre, they often became the lightning rod for local protests against public sector retrenchment. Local politics therefore weigh heavily on ARSs, a recurrent complaint of private hospital representatives (interview, PRIV3; PUB3; POL3) and other private sector actors such as outsourcing service providers (Cany 2012). This politicisation was thus perceived as a major drag on marketisation, corroborating a key insight of Krachler and Greer (2015). It also underlines the importance of region–centre dynamics in forming the context for this, since regional actors were seen as more susceptible to this pressure than the centre.
While private sector interviewees felt personally sympathetic about the pressures acting on ARSs, there was a growing push to exert their own influence to counteract the political forces they saw as disrupting marketisation. Hence the private sector has been reconfiguring its operations in order to compete more fiercely with public hospitals. Private provision has expanded in certain specific areas which have strategic value, notably emergency services. While these functions are not profitable per se, they constitute ‘shop windows’ in which firms can recruit patients requiring more lucrative follow-ups (interviews, TU1; AC1; see also Durousset 2010). They may also vie with the public to recruit the highest-profile medical staff (interview, TU4), and for positions in newspaper-published league tables (interview, AC3).
As private actors have tried to expand, they have increasingly viewed ARSs as obstacles (interview, PRIV2), owing to the fuzziness of contracting tools which they perceived as enabling pro-public agendas. The political relationship between public and private providers has become more conflictual; Couty (2012) refers to an intensifying ‘communications war’ in French healthcare in the wake of marketisation.
One private sector response to this increasingly tense relationship with public authorities has been its own spatial reorganisation. The past decades have seen extensive structural consolidation in French private healthcare. Cost pressures, low profits and the need for heavy investment have seen large numbers of ‘artisanal’ owner-operator clinics bought up and amalgamated into larger networks by major investment funds. These networks have tended to delineate themselves territorially so as to avoid intense competition between private providers (interview, PRIV1). This process has had an important impact on regional planning in certain regions, especially where larger, more multidisciplinary private hospitals are emerging (interview, PRIV1; see also IGAS 2012).
In Nice and Marseille, for instance, such multidisciplinary hospitals have entered the lacunae left by the closure of smaller local public facilities (interview, TU2), meshing with centrally imposed marketisation strictures which advocate public sector retrenchment. Private actors also see this model as better-adapted to cope with perceived political volatility in government setting of T2A tariffs (because they can hedge against unexpected shifts in the value attributed to different procedures) (interview, PRIV1). Thus, private providers are seeking to capitalise on centrally imposed marketising pressures in the French system, while publicly criticising the fuzziness which exists at the regional level. Private sector respondents were hoping that the former would make ARSs more reliant on them over time. Hence a pincer movement emerges to squeeze regional state capacity: a centrally driven framework pushes the regional level to retrench, while the private sector emerges to plug the gaps. Neoliberal state transformation thus hollows out regional planning agency.
Ultimately, through increasingly assertive public advocacy, private sector actors aimed to strip away the qualitative fuzziness which still exists at the regional level. As we argued in the preceding section, this fuzziness is the main channel through which regional planning agency can be exercised. Hence, private sector reorientation in response to marketisation is another way in which marketisation has challenged regional planning agency. These changes are further evidenced by the way in which the Fédération de l'Hospitalisation Privée (FHP) has affiliated to the French employers’ federation (MEDEF). This is in order to support its role as a leading proponent of ‘sound finances’, and to gain allies against the perceived anti-private bias of public authorities (interview, PRIV1). Trade union respondents also saw this as a shift towards a more assertive and confrontational private sector (interview, TU1). The FHP has geared up its public advocacy of public sector budget restraint, and developed a more vocal critique of the supposed ‘immortality’ of the public sector (despite the closure of many hôpitaux de proximité (Dupont 2012)).
Hence marketisation in the French hospital system has overlapped with two important developments in the private sector. First, marketisation dovetails with a longer-running trend towards the consolidation of private healthcare into larger territorial monopolies offering more multifaceted facilities. In this sense, it is paving the way for further public retrenchment. Second, private actors have intensified their public critique of the political pressures acting on ARSs, and the fuzziness of the tools used in regional planning. Both of these developments tend to facilitate the more centrally dictated marketising operations of the ARSs, while seeking to delegitimise the fuzziness through which local state actors can exercise regional planning agency.
Conclusion
The aim of this article has been to examine the tensions between two important aspects of neoliberal public service restructuring: decentralisation and marketisation. While the notion of empowering regional actors and undermining the ‘monolithic’ centre has been a legitimising device for many neoliberal reformers, we examined what happens to the relationship between centre and regions in the context of public service marketisation.
Taking French hospitals as a case study, the data suggest that marketisation has hindered effective and autonomous regional planning. Despite growing discourse around ‘regionalisation’ in the hospitals sector, it remains stunted in France. We have identified various reasons for this. Most importantly, we argued that marketisation has unleashed centralising pressures. Regional actors have been required to act as the ‘armed wing’ of the central government in overseeing local hospital closures. Centrally imposed financing systems have undermined regional efforts to stimulate supply and improve coordination. However, we also showed how the fuzziness of key institutional tools left scope for regional planning agency. Finally, we examined how shifts in the French private sector, in the wake of marketisation, was also threatening regional planning agency, as it consolidated itself and sharpened its political voice as a proponent of ‘sound finances’.
What can this French case study tell us more widely? The dynamics we have identified here are by no means limited to France. DRG financing, for instance, has proliferated across many health systems (Krachler et al. 2021). Even beyond healthcare, similar mechanisms which tie the funding of public services to centrally determined outcomes designed to stimulate competition have become increasingly prominent (Greer & Umney forthcoming). Our study is of wider relevance, therefore, because it places attention on the region–centre tensions that marketising dynamics stir up. While Marxist scholarship in particular has insightfully commented on the implications of marketisation for dynamics of class exploitation and capital accumulation, these internal institutional tensions have, so far, attracted less interest.
Conceptually, regional planning agency is important for Marxist theorising on the state and has so far been under-examined. In this article, we have steered away from the broadest and most fundamental questions asked in Marxist state theory: that is, how the state should be conceptualised; what kinds of social and material forces act on it. Instead, we have taken a different tack which we hope can inform future Marxist scholarship. Namely, we have prioritised a detailed empirical understanding of the tensions and dysfunctions that emerge within the constellation of apparatuses that comprise the state, in the wake of neoliberal market reforms. We cannot understand the role of the state and the pressures acting on it without paying attention to these dysfunctions. Hence, while our data come from France, we make the more general argument that, where the state’s public service functions are concerned, tensions between regional and central state are especially salient. Various central states have repeatedly attempted to use local state actors to drive through reforms, but the state apparatus in its totality is rarely coherent enough to allow this process to run smoothly. In short, our contribution to Marxist theory is to advocate close focus on points of internal incoherence within neoliberal state configurations. This incoherence has real practical importance, but risks being overlooked when the neoliberal state is (quite understandably) analysed primarily as an instrument of class discipline or as the facilitator of capitalist accumulation.
Clearly, we cannot claim that the tensions between regional planning agency and marketisation will play out identically in other cases. Rather, the point is that there is a tension here which runs across different conjunctures where public service marketisation takes place, but manifests in different ways. This tension requires understanding, because it can potentially provide an important critical lever for opponents of marketisation. In British healthcare, for instance, the Health and Social Care Act created new local planning institutions which were to an extent beyond central control. In consequence, the centre found itself watching frustratedly as marketisation and privatisation did not make as rapid progress as hoped. This is not, clearly, to present CCGs as radical actors. They were a creation of the right-wing government whose intended purpose was to facilitate privatisation. But empirically, this did not run smoothly. As local actors, they were susceptible to local protest and hence local politics became a thorn in the side of the reform package (Krachler & Greer 2015). In the United Kingdom, the centre had weaker control over regions than in France. Consequently, in future reforms, we may see attempts by the British government to re-exert control over regions as we have detailed in France. The implication of this is that left critics of marketisation could make headway by framing their strategies around advancing demands for meaningful regional planning. Many ‘reforms’ take decentralisation and local responsiveness as a mantra, while delivering something quite different. Parsing the ambiguity of decentralisation, and politicising the question of local accountability, is thus an important intellectual task for socialists.
Finally, we also shed more light on the evolving role of the private sector, showing how private capitalists also intervened in shaping the tensions between marketisation and regional planning and thus between central and regional branches of the state. In our case study, the private sector was consolidating but remained frustrated by the perceived political role of the ARSs, even though, as we argue, these actors had little meaningful regional planning agency. While much of our discussion of the private sector is quite specific to French healthcare, this again alludes to a wider principle. It lends support to Krachler and Greer’s (2015) argument concerning the politicisation of health provision, which they see as a key barrier to the progress of marketising policy packages. While many smaller hospitals have been closed in France (Dupont 2012), political sensitivities clearly play heavily on the minds of ARS planners and have influenced their use of regional planning agency, just as Krachler and Greer show they did in the United Kingdom as well. This politicisation may explain why the tactic of using regional institutions to force through privatisations has been comparatively more successful in Germany (André & Hermann 2009). In France, a centralising private hospitals industry has arguably escalated the politicisation of the sector, which has catalysed public opposition to their role.
It is also worth considering how the questions examined here may be affected by the ongoing COVID-19 pandemic. There is an increasingly voiced argument that market-oriented policies, particularly those such as T2A, have not been optimal in preparing health systems for the pandemic. French public discussion around hospital funding has highlighted this point, arguing that market incentives led to excess capacity being (with a degree of short-sightedness) being redefined as wastage (e.g. Grimaldi et al. 2020). This argument is also made by other left authors about the United Kingdom (Leys 2020) and the United States (Davis 2020). In France, there is pressure on Macron to backtrack from T2A, though at time of writing this remains unpredictable, as the President remains ideologically predisposed to the model (Sicot 2020). Pandemics as simultaneously medical and social problems require extensive coordination and planning, involving links between different actors and close embedding of services in local networks (Chandra & Chandra 2020). Hence the issues we raise here are surely relevant to the pandemic context, but it remains too early to make pronouncements about what will or should happen.
Ultimately, our article argues for more attention to be placed on the conflict-laden and dysfunctional institutional processes which market-oriented reforms entail, rather than focusing only on their inequitable outcomes. While the latter have understandably attracted much criticism, the former help us identify fragilities in the way ‘neoliberal’ states have restructured public services. To grasp these fragilities, we need to understand the tensions that emerge between central and regional state in the wake of marketisation initiatives, and how this has ratcheted up political conflict within health systems. The actors who can win these political conflicts, however, remains an open question, and will be vital in shaping the future of public services more generally.
Footnotes
Acknowledgements
The authors would like to thank Alex Nunn and the anonymous reviewers at Capital and Class. Previous drafts of this paper have benefitted from comments from Ian Greer, Ana Manzano, and Mark Saunders.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research received support from the European Research Council-funded project “The Effects of Marketization on Societies” (#313613).