
Abstract
Case Description:
A 56-year-old man with persistent knee pain and poor physical functioning due to recurring loosening of a (revised) total knee arthroplasty, was treated with a modified Gritti-Stokes amputation.
Objectives:
to describe the modified Gritti-Stokes amputation technique as an ultimate therapy for failed total knee arthroplasty and to assess the functional outcome for one patient 1 year post-surgery.
Study design:
a single patient case study.
Treatment:
a modified Gritti-Stokes amputation, with removal of the overlying cartilage and subchondral surfaces of both the patella and femur after removing the total knee arthroplasty.
Outcomes:
After rehabilitation, the patient has a fully end-bearing residual limb, is able to walk without pain (with a prosthesis) and perform his daily activities.
Conclusions:
In cases of recurring loosening of a (revised) total knee arthroplasty, a modified Gritti-Stokes amputation can create an end-bearing residual limb without pain and with good functional outcome.
Background
When a patient is not able to function with a total knee arthroplasty (TKA), for example because of loosening of the arthroplasty, and revision of the TKA is no longer an option, amputation may be the solution. Either a transfemoral amputation (TFA) or a knee disarticulation (KD) with removal of the total knee, is possible. However, little is known about the outcome of a KD with removal of the total knee. Only one case study 1 has described a KD in which the proximal part of the total knee was also removed, and the patella was attached to the anterior cruciate ligaments. The patient, an 89-year-old woman, was left with a fully weight-bearing residual limb, but apart from mention of limited household walking, no functional outcome was reported.
Another way to modify a KD, and thereby retain the advantages of a KD, such as an end-bearing residual limb, is to place the patella intercondylar beneath the femur, similar to a Gritti-Stokes amputation (GSA). In a GSA, the end of the femur is sawn through at the level of the adductor tubercle with a traditional right angle cut or with a sloped cut (upward and backward from the anterior aspect) to prevent the patella from slipping forward. The articular surface of the patella is sawn off. 2 To keep the patella in place at the end of the femur, holes are bored through the edge of the patella and femur so that the patella can be stitched to it. 3 Alternatively, the patella is secured to the distal end of the femur by absorbable sutures through the joint capsule and into the soft tissues behind the femur, so there is no fixation through the bone itself. 2
GSA has varied in its popularity, and its use has been discussed among different surgeons and limb-fitting centers with concerns primarily about non-union of the patella, painful residual limb, and difficulties in fitting a satisfactory prosthesis.2,4,5 However, the results for patients have been mainly positive,3,4,6 –8 raising questions as to why this technique has fallen out of favor.
The aim of this case study was to describe the amputation technique and the functional outcome 1 year post-surgery in a young, still-working patient, who suffered from persistent knee pain and poor physical functioning due to recurring aseptic loosening of his revised TKA. A secondary aim was to evaluate if the residual limb resulting from GSA is indeed end-bearing.
Case description
Participant
A 56-year-old man who endured long-term (34 years) therapy-resistant knee problems on the right side received a TKA 4 years ago, after a failed salvage correction osteotomy 18 years ago for end-stage arthritis. Three years ago, he developed pain due to early aseptic loosening of this TKA. The arthroplasty was revised with the use of a stemmed revision implant. Over the next several months, the patient gradually developed a significant patellar tendon retraction which was complicated by an intramuscular quadriceps rupture, leading to significant impairment of his knee function and strength. Conservative therapy with a knee brace (bandage) and two crutches followed, but hydrops and pain in the knee remained. The patient had been an electrician, but because of his knee complaints he became a truck driver. Despite enrolling in a pain rehabilitation treatment program (to learn to deal with the pain) and being fit with a dynamic knee–ankle–foot orthosis for walking, he continued to complain of progressive pain during axial loading.
A bone scan showed recurrence of aseptic loosening of both the tibial and femoral implants. The orthopedic surgeon suggested surgery, either a knee arthrodesis or a renewed revision procedure. Due to the combination of severe functional impairment with knee flexion of less than 85°, which also led to psychosocial problems, the patient preferred an amputation in order to regain more optimal function with a prosthesis. Normal functioning could not be reached with a renewed revision procedure. The patient wanted to be able to walk without pain (for at least 10 min) and cycle again. He also wanted to return to work and regain his social life. After considering the pros and cons, the patient and his orthopedic surgeon came to a shared decision to amputate the lower limb. For this case report, written informed consent was obtained from the patient.
Treatment surgery technique
The surgery technique consisted of removing the TKA (both the tibial and femoral implants), automatically leading to shortening of the amputation level and a slight angulation of the femoral condyle transection in order to prevent the patella from slipping forward. Also, the overlying cartilage and subchondral surfaces of both the patella and femur were removed to create a well-perfused bony surface. Because of the emerged central intercondylar cavity and weakened remaining condyles, the patella was placed intercondylar, beneath the femur. While in the normal GSA, the patella itself is sutured to the distal end of the femur, we stitched the patella tendon to the posterior knee capsule to create an end-bearing distal surface. We defined this as a modified GSA (Figure 1).
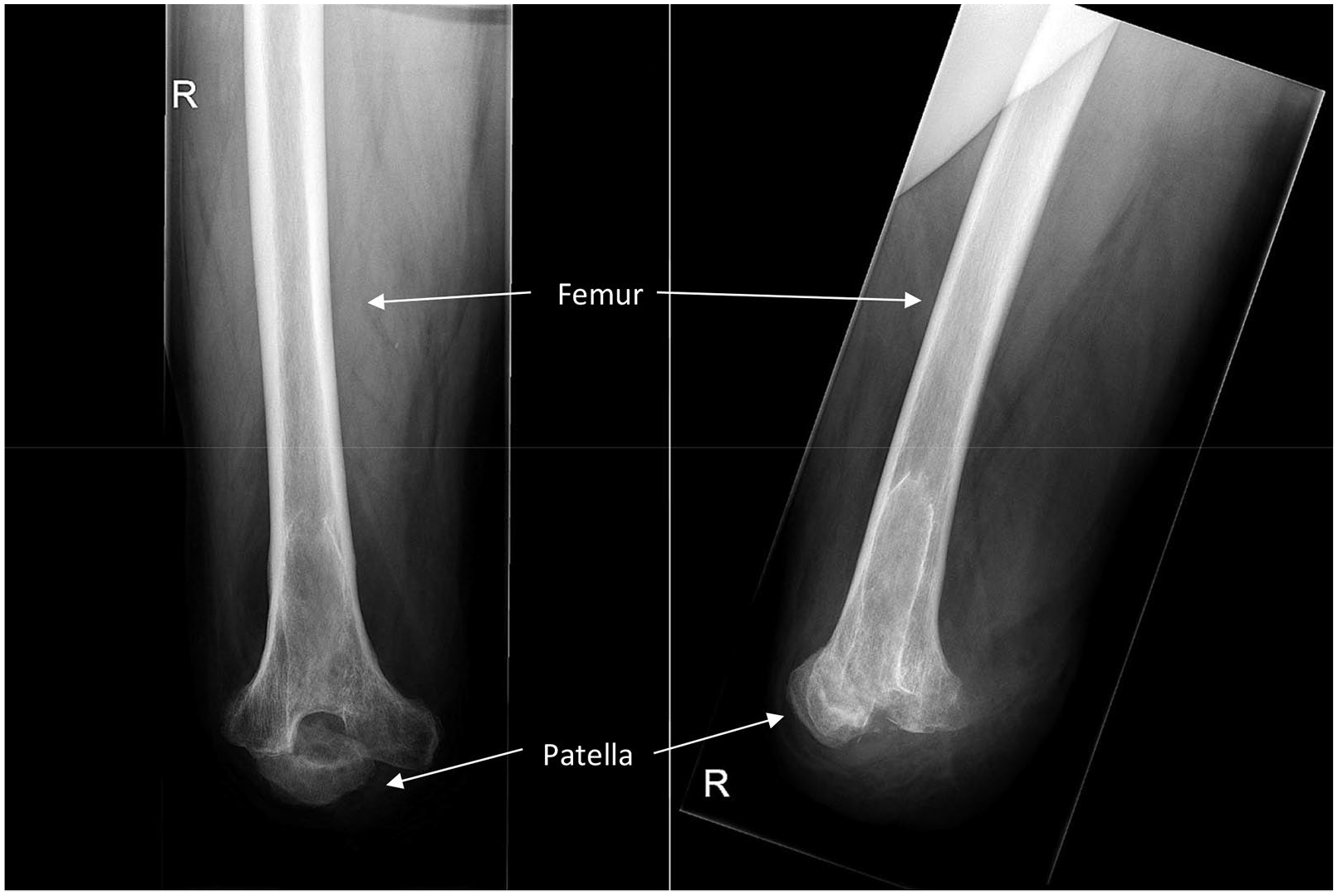
X-ray of the residual limb, with the patella placed intercondylar, beneath the femur. On the left the anterior–posterior image, on the right the lateral image.
Fitting of the prosthesis
Because of the rarity of this modified GSA, we carefully began (2 months after the amputation) with a total contact surface-bearing socket, with minimal end-bearing on the patella. We were doubtful whether the patella could bear high peak loads. In a “normal” KD, the patella is placed in front of the condyles with the apex not reaching below the condylar level, creating a better force distribution with a triangular residual limb profile. In this way, weight-bearing is mostly on the condyles and not on the patella. However, fitting the prosthesis was complicated because the soft tissue and skin tucked up above the socket, resulted in pain. Therefore, we decided to make the prosthetic socket full end-bearing on the patella. This was done 4 months after amputation.
Outcomes
Data were collected retrospectively by analysis of the patient records. The prosthesis consisted of the following components: seal in liner X5, rigid closed outer socket (without ischial weight-bearing), 3R80 knee (Otto Bock), and Vari-Flex foot (Össur). In this way, the residual limb was fully end-bearing. After 3 weeks of inpatient and 4 months of outpatient rehabilitation, the patient was able to walk with his prosthesis on level surfaces without a walking aid and at longer distances outside with a cane. Functional outcome measurements at the end of the rehabilitation phase were as follows: 6 minute walking test 326.4 m, L-test 24.09 s, and Four Square Step Test 11.7 s. 9
At 1-year post-surgery, the patient had no residual limb pain with the full end-bearing socket, no residual limb problems, and no signs of patella fusion failure. He wore his prosthesis during the entire day. He could walk without pain for distances up to 2 km outside without using a walking aid, was able to climb stairs step by step (i.e. a typical community ambulator: able to walk at a variable cadence and to traverse most environmental barriers) and to cycle (<6 km) on a regular grandma bike with adaptation of the pedal (toeclip). He also engaged in exercise, walking on a treadmill (6 km) and handbiking, three times a week. He was independent in daily life and household activities such as taking a shower, getting dressed, vacuum cleaning, setting the table, and cooking while standing. He was satisfied with these activities. For his driver’s license, he needed a new medical examination and the accelerator pedal needed to be transposed to the left side. His next focus was work reintegration, and he was pursuing a different line of work.
Conclusion
This case report describes a modified GSA for a patient who experienced recurring loosening of a TKA. The procedure resulted in a pain-free and fully end-bearing residual limb with good functional outcome at 1-year follow-up.
Opinion on the GSA is divided in the literature. Some surgeons recommend it, others strongly condemn it. In this single-patient case study, in which a KD was no longer an option, we compared the GSA with the TFA. For both amputation techniques, a longer residual limb length is preferred because thigh muscle function is better preserved, which reduces the risk of hip flexion 3 and abduction contractures, especially when amputating at or below the Hunter’s canal level, to preserve the function of the proximal part of the adductor. 10 Greater leverage results in reduced metabolic expenditure during ambulation and more stability for sitting and facilitating transfers.3,7
Specific advantages and disadvantages of the GSA, mentioned in the literature, are shown in Table 1. Despite the majority of these arguments being in favor of a GSA, the GSA is not widely performed anymore. 3 Surgeons became unfamiliar with this amputation technique. Its disuse partly stems from its poor reputation of painful non-union of the patella with poor prosthetic fitting.2,3,5
Specific advantages and disadvantages of the Gritti-Stokes amputation.
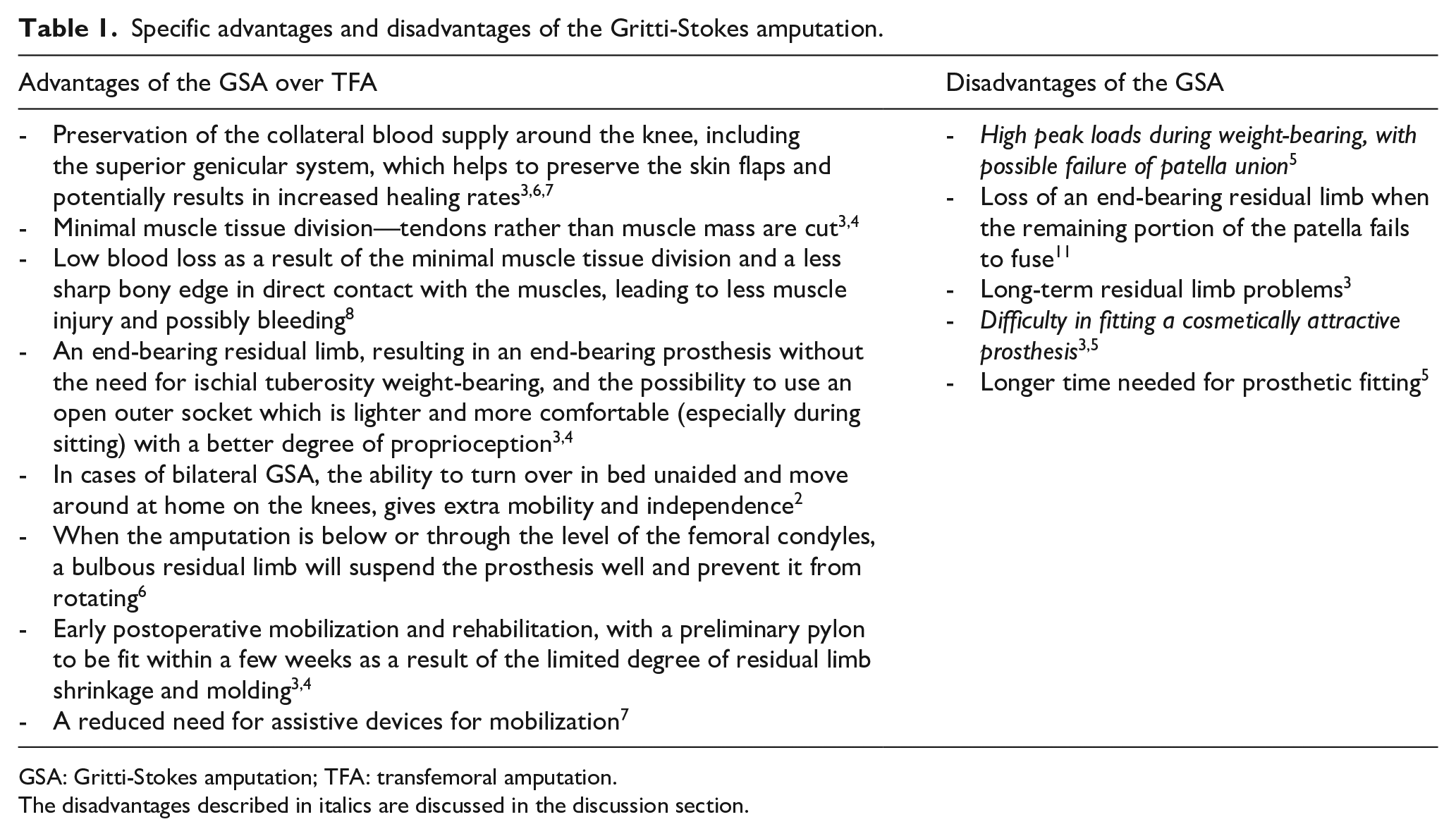
GSA: Gritti-Stokes amputation; TFA: transfemoral amputation.
The disadvantages described in italics are discussed in the discussion section.
To overcome the disadvantages of the GSA, it is important to achieve a fusion between the patella and the femoral condyles. Fusion can only be achieved by (1) complete removal of the overlying cartilage and subchondral surfaces of both the patella and femur and (2) creating a stable patella fixation by tensioning the patella over the distal femoral surface. If there is any doubt, consolidation/non-union can best be determined by a computed tomography (CT) scan. Once there is union, high peak loads on the patella during weight-bearing should not be a problem, as the patella is already the most loaded surface within the human body, capable of withstanding cyclic loading up to three to five times body weight during normal stair climbing and running. 12 The prosthetic fitting problems and cosmetic issues have become less important with the development of modern prosthetic knee mechanisms. 5
A limitation of this single-patient case study is that we did not have functional outcome measurement data before the amputation to compare between pre- and post-amputation, and we were unable to compare our results to an alternative therapy, such as a knee arthrodesis. Our patient had no peripheral vascular disease, which is, in general, the main cause for amputation. It should be investigated whether a vascular patient could also benefit from a modified GSA. In the future, we recommend measuring mobility and psychosocial outcomes for persons with a lower limb amputation, before and after amputation in a case series of TKA failure leading to a modified GSA. Because of the many important advantages of the GSA, we suggest this technique might be reintroduced and given more consideration as an alternative to the TFA.
In conclusion, a modified GSA was earlier only described as an ultimate therapy for an older patient with limited walking ability and loosening of a TKA and is now for the first time described in a young and working patient suffering from recurring loosening of a (revised) TKA. The modified GSA technique created a pain-free and end-bearing residual limb, and good functional outcome, by achieving functional rehabilitation goals to the patient’s satisfaction. We hope that this case report will highlight the modified GSA as option for treatment.
Footnotes
Author contributions
The authors made the following contributions to the present manuscript: KM and RK designed the study; RK performed the surgical procedure; WR and FL drafted the manuscript; and WR, KM, RK, FL and JG contributed in critical revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.