
Abstract
Background:
Persons with transtibial amputation report curb negotiation is more challenging than negotiating stairs. It is unknown if amputation technique influences curb negotiation ability. Traditional transtibial amputation surgical techniques do not join the distal tibia and fibula (non-Ertl), whereas a transtibial osteomyoplastic amputation (Ertl) creates a “bone bridge” connection. The Ertl may facilitate ambulation through greater residual end load bearing.
Objectives:
To determine if ability to negotiate a curb differs between Ertl and non-Ertl groups.
Study design:
Cross-sectional study.
Methods:
Non-Ertl (n = 7) and Ertl (n = 5) participants ascended a 16-cm curb using their amputated and intact limb as the lead limb. Motion data and ground reaction forces were used to calculate ankle, knee, hip, and total limb work for ground and curb steps.
Results:
On the ground, the amputated limb of both groups produced less work than the intact limb. In contrast, on the curb step, the Ertl amputated limb generated more net hip work than the non-Ertl amputated limb. As a result, the net limb work of the Ertl amputated limb did not differ from the non-amputated limbs.
Conclusion:
Comparisons between the amputated limb of Ertl and non-Ertl groups suggest use of a different curb stepping pattern between groups.
Clinical relevance
These findings suggest that surgical technique may influence curb negotiation ability in individuals with transtibial amputation. Specifically, the Ertl group is able to produce more hip power than the non-Ertl group while negotiation a curb which may be attributed to the increased ability to end-load bear on the residual limb.
Background
Roughly, 25% of the estimated 2 million Americans living with limb loss resulting from dysvascular disease, trauma, or cancer 1 have undergone a transtibial amputation (TTA). These individuals must adapt to various challenges associated with limb loss. To avoid a slip, trip, or fall, the body must accommodate varying surface conditions during normal gait. However, this is especially difficult for those with lower extremity amputations. Relative to age-matched, able-bodied individuals, persons with TTA have an increased risk of falling and fear of falling.2,3 As a result, 60% of these individuals report falls affect their daily activities, work, and confidence. 4
During stair ascent, the intact limb of persons with TTA experiences higher vertical ground reaction forces (GRFs) than the amputated limb and limb of individuals without amputation 5 resulting in an asymmetric loading pattern between the limbs. This suggests that the intact limb is able to exert higher forces to move the body up the staircase. In individuals without amputation, vertical GRF impulse during double limb support decreased as a function of obstacle height which was attributed to contralateral knee flexion to aid in controlling limb elevation. 6 In addition, the anteroposterior impulse during the braking phase of obstacle negotiation increased, which coincided with the decrease in forward hip velocity. 6 All of the above adaptations allow the body to rapidly respond to changes in the environment and safely navigate obstacles in persons without amputation.
The evaluation of more challenging tasks is important to those caring for and those living with TTA. Persons with TTA report curb negotiation is more challenging than negotiating stairs even though they are encountered with the same frequency.7,8 However, the underlying mechanisms contributing to the challenge of curb negotiation are unclear. To date, we are aware of only one study that investigated curb negotiation in persons with TTA. Barnett et al. 9 found persistent asymmetries between the amputated and intact limbs for people with unilateral TTA at 1, 3, and 6 months after amputation. Specifically, the intact limb spent more time in stance, produced more power, and had a larger range of motion than the amputated limb while ascending a curb. Since the amount of literature for this task is limited, drawing on tasks similar to stepping up a curb such as obstacle negotiation, stair ascent, and curb negation in non-amputees may guide research in persons with TTA.
Furthermore, individuals without amputation have shown that while traversing a curb, the limb on the ground level is primarily responsible for pushing the body upward onto the curb, whereas the limb on the curb level was primarily used to stabilize the body during the height transition and then was responsible for propelling the body forward after the curb. 10 For those with TTA, this strategy could prove challenging. For example, if the amputated limb is on the ground level, the prosthetic foot/ankle is unable to generate energy to propel the body upward. As a result, they must compensate using other joints. The hypothesis is that the intact limb will use a knee predominant strategy to pull themselves upward, whereas the amputated limb will adopt a hip strategy, to push themselves upward. However, this strategy may change due to the individual’s ability to effectively use the amputated limb to support the body during this task. This ability is dependent upon many factors, including amputation technique.
It is unknown that whether amputation surgical technique influences individuals with TTA’s ability to negotiate a curb. An uncommon amputation technique is the transtibial osteomyoplastic amputation (Ertl). For example, less than 20% of US soldiers underwent an Ertl TTA between 2001 and 2011. 11 This technique has been suggested to improve the overall physiology of the residual limb by maintaining the medullary canal pressures and improving vascularization of the remaining tissues.12,13 Unlike a non-Ertl amputation, the Ertl creates a “bone bridge” to connect the tibia and fibula, seals the medullary canal, and sutures the anterior and posterior residual musculatures together. 12 The Ertl has been suggested to tolerate greater direct load bearing of the distal end of the residual limb (standing directly on the stump without a prosthetic socket) than the non-Ertl procedure.12,14 Greater residual limb load bearing has the potential to positively impact long-term outcomes by increasing symmetrical loading between limbs, thereby reducing the increased risk of osteoarthritis in joint proximal to the site of amputation and the intact limb joints.15,16 Other factors may influence symmetrical loading such as rehabilitation, socket fit, and prosthetic foot design. Despite the possible benefits of the Ertl procedure, non-Ertl procedures are more common since the procedure is not complicated with the creation of the bone bridge which is also associated with increased tourniquet time. 17 Thus, the Ertl procedure must be completed by a specialized surgeon.
Given the higher prevalence of non-Ertl procedures, limited data related to functional outcomes following Ertl amputations exist. One small study was inconclusive if differences exist between the groups during normal walking. 18 Other studies have relied solely on self-reported questionnaire data to determine if differences exist between amputation techniques and suggest no differences exist.19,20 However, more challenging tasks have not been investigated. By investigating a more challenging task, such as curb negotiation, it is more likely that any underlying functional differences between surgical techniques would be highlighted. As this task requires the amputated limb to solely support and balance the body while on the ground level and on the curb level, an increased ability to bear loads on the residual limb may improve curb negotiation ability.
Therefore, the purpose of this study was to determine whether Ertl amputations lead to a better functional ability to step up onto a curb compared to non-Ertl amputations. Since a suggested biomechanical advantage of the Ertl amputation is an increased capability to bear loads on the end of the residual limb, it was hypothesized that those with Ertl amputations would produce greater joint work at the ankle, knee, and hip with the amputated limb while negotiating a curb compared to the non-Ertl amputated limb. Joint work takes into account kinematic and kinetic variables and provides insight into each joint’s individual contribution to the motion. Furthermore, joint and net limb work can provide insight into limb asymmetries and differences between amputation techniques.
Methods
Participants
Two groups of people with TTA were recruited: non-Ertl (n = 7; 88.3 ± 16.0 kg, 1.78 ± 0.08 m; 55 ± 5 years) and Ertl (n = 5; 79.8 ± 15.5 kg, 1.79 ± 0.08 m; 55 ± 8 years). Inclusion criteria were amputation resulting from trauma, classified as Medicare Functional Classification Level (MFCL) levels K3–K4, wore energy storing and releasing (ESR) prosthetic feet, no concomitant musculoskeletal injuries, neurological, or visual impairments, able to understand directions and comprehend the requirements of the study in English. In addition, all participants had amputations for more than 6 months and had been using their prescribed socket for at least 6 months, were physically active 3 days a week including activities such as long walks, resistance training, and aerobic training. Participants were allowed to wear their prescribed socket and suspension system; these included lock and pin and vacuum systems. No participants had undergone revision surgery for their amputation. Institutional Review Board at University of Northern Colorado provided approval and oversight for the study.
Data collection
Retroreflective markers were placed on anatomical landmarks on the upper and lower body and trunk using the Plug-in-gait model. A 10-camera motion capture system (100 Hz) captured motion data (VICON, Oxford, UK).
To recreate a curb in the laboratory, a force plate (mounted on a steel frame) was placed over and in-line with two tandem force plates (AMTI, Watertown, MA, United States) in the floor of the regular walking surface of the laboratory (Figure 1). By placing the force plates in this manner, we were able to collect a step on the ground prior to the curb (GROUND) and the step up the curb (CURB). During each trial, GRFs from each force plate were collected (2000 Hz).
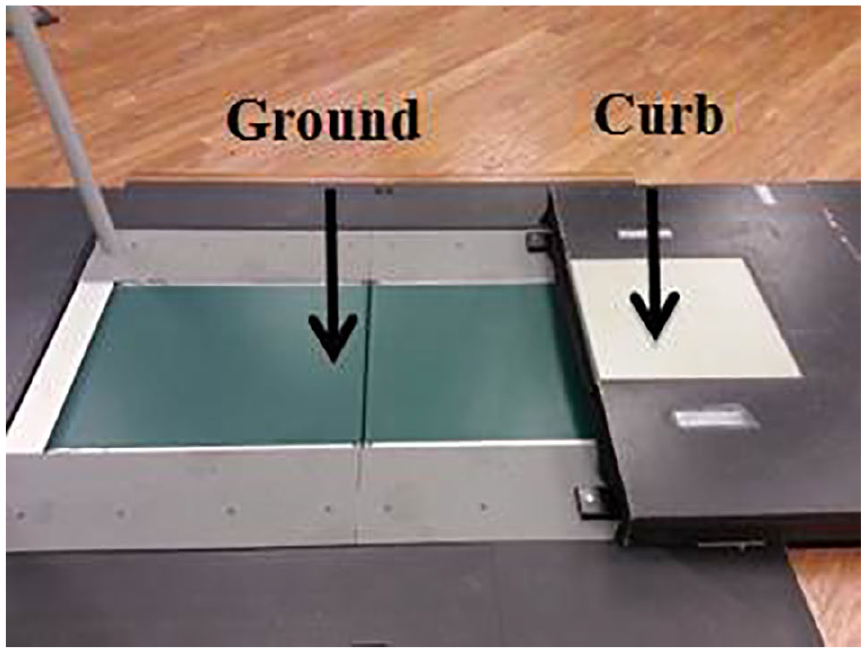
Illustration of the curb design. In this image, participants walked from left to right and ascended the curb. Participants were asked to strike the GROUND and CURB with each limb.
The top of the CURB was 16 cm higher than the GROUND level. A wooden skirt around the curb force plate extended the walking surface 3 m beyond the trailing edge of the curb. This simulated a curb similar to those encountered on a daily basis. According to the US Department of Transportation Federal Highway Admin-istration, curb heights can vary between 10 and 25 cm. 21 The height of 16 cm was based on the street curb height outside of the building where data collections occurred.
Participants walked up onto and past the curb for 3 m at their self-selected walking velocity and were allowed to practice prior to data collection. Three successful trials were captured with each leg (intact and amputated) striking the GROUND force plate and then CURB plate for a total of six successful trials. Walking velocity was measured using a timing system whose measurement zone (5 m) encompassed the curb. For a trial to be included for analysis, the walking velocity had to be within ±5% of the participant’s preferred walking velocity. Participants traversed ~3 m before they reached the data collection area ensuring steady state walking before reaching the curb.
Data analysis
The GROUND and CURB steps were analyzed separately. Subject-specific models were created using subject-specific anthropometrics. 22 These models were used to determine three-dimensional (3D) angular kinematics, which were combined with the GRFs using inverse dynamics to estimate ankle, knee, and hip and powers using Visual3D (C-motion, Germantown, MD, United States).
Ankle, knee, and hip joint work for the intact and amputated limbs was estimated as the integral of the power curve for each joint. The joint power curves were not rectified prior to integration in order to characterize both positive and negative joint work. The positive and negative work at each joint was summed to determine the net work performed at each joint. Furthermore, the total limb joint work was computed as the sum of the net joint work produced at each joint.
Statistical analysis
A two-sample t-test was used to test for significant differences in walking velocity between groups (α = 0.05, SAS 9.4, Cary, NC, United States). A single-factor multivariate analysis of variance (MANOVA) with α = 0.05 (SAS 9.4, Cary, NC, United States) was used to evaluate whether differences in joint work existed between the groups and limbs. Predetermined orthogonal contrasts were performed to assess if differences existed between limbs (intact vs amputated) and amputation techniques (Ertl vs non-Ertl). Effect size was calculated using Cohen’s d (d). 23
Results
All participants wore ESR feet such as Variflex®, Re-flex®, Flex-foot® and were able to walk up the curb safely (1.28 ± 0.20 m/s Ertl vs 1.28 ± 0.19 m/s non-Ertl) with each limb as the lead limb. No differences were observed in walking velocity between the groups (p = 0.999).
GROUND step results
A significant model effect was found for the GROUND step (p < 0.001). The intact limbs of the Ertl (p < 0.001, d = 6.01) and non-Ertl (p < 0.001, d = 3.97) groups produced significantly (p < 0.05) more positive ankle work than the respective amputated limbs during steps on the GROUND (Table 1). Negative ankle work (Table 1) of the Ertl amputated limb was significantly smaller than the Ertl intact limb (p = 0.049, d = 1.34). All other negative work performed was similar across groups and limbs.
Positive, negative, and net joint work (J/kg) on the GROUND step for both conditions and limbs. Data are shown as mean ± SD.
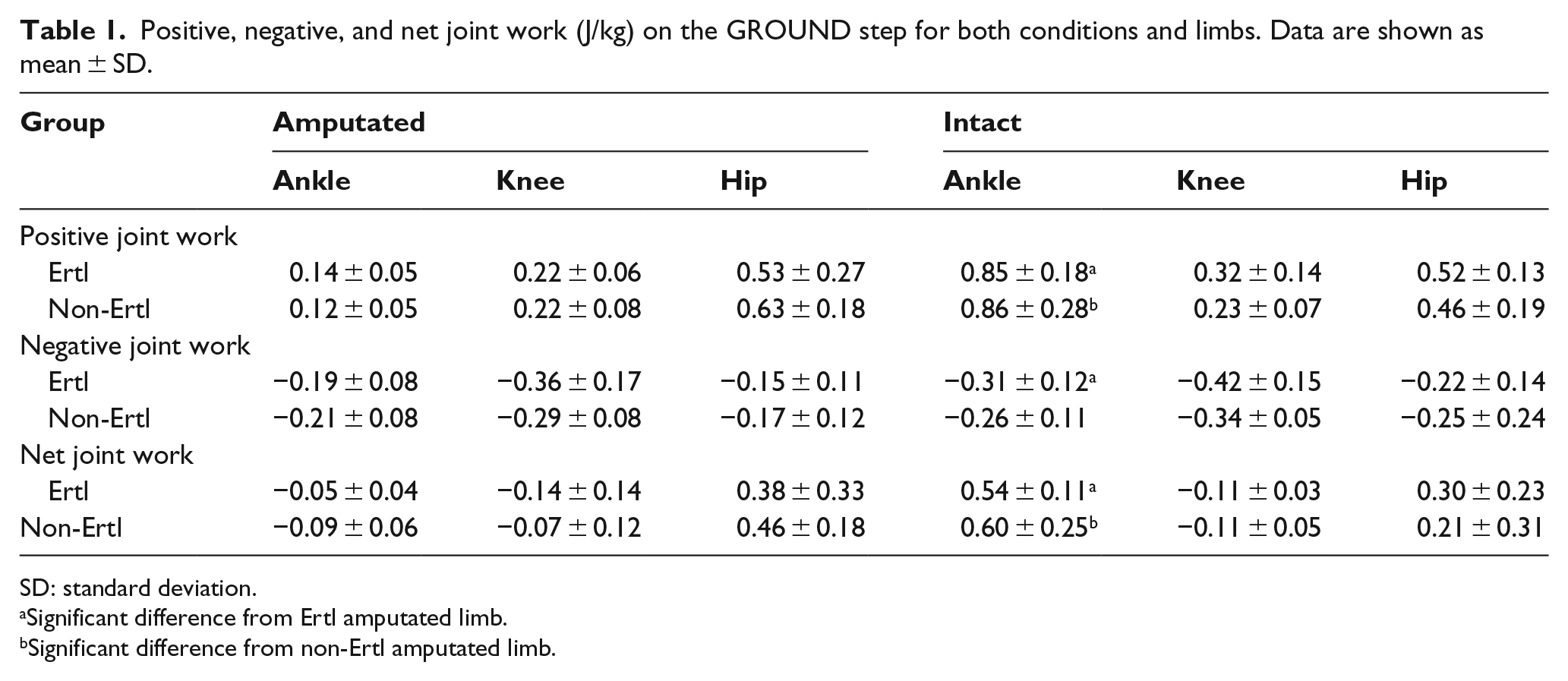
SD: standard deviation.
Significant difference from Ertl amputated limb.
Significant difference from non-Ertl amputated limb.
Ertl (p < 0.001, d = 7.97) and non-Ertl (p < 0.001, d = 4.1) intact limb net ankle joint work was significantly larger than the respective amputated limb during the GROUND step (Table 1). Total limb work (the sum of net joint work at the ankle, knee, and hip) was significantly larger for the Ertl (p < 0.001, d = 1.92) and non-Ertl (p < 0.001, d = 1.32) intact limbs compared to the respective amputated limbs (Figure 2).
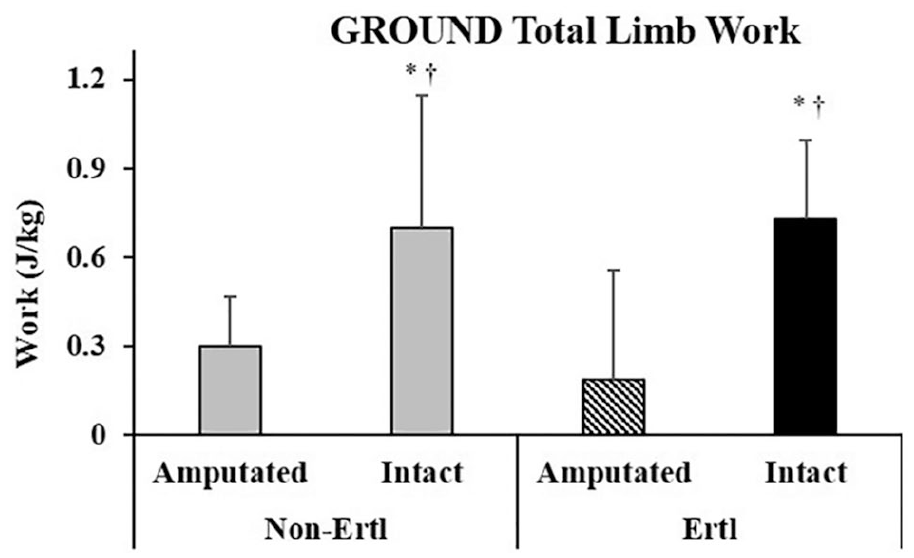
Net limb work for the GROUND step. †Significantly different from Non-Ertl amputated limb.
CURB step results
A significant model effect was found for the CURB step (p = 0.036). The Ertl (p = 0.013, d = 1.34) and non-Ertl (p = 0.002, d = 3.649) intact limbs produced significantly more positive ankle work than the respective amputated limbs during the CURB step. Ertl (p = 0.04, d = 1.28) and non-Ertl (p = 0.003, d = 2.45) amputated limbs produced significantly less positive knee work than the respective intact limb (Table 2).
Positive, negative, and net joint work (J/kg) on the CURB step. Data are shown as mean ± SD.
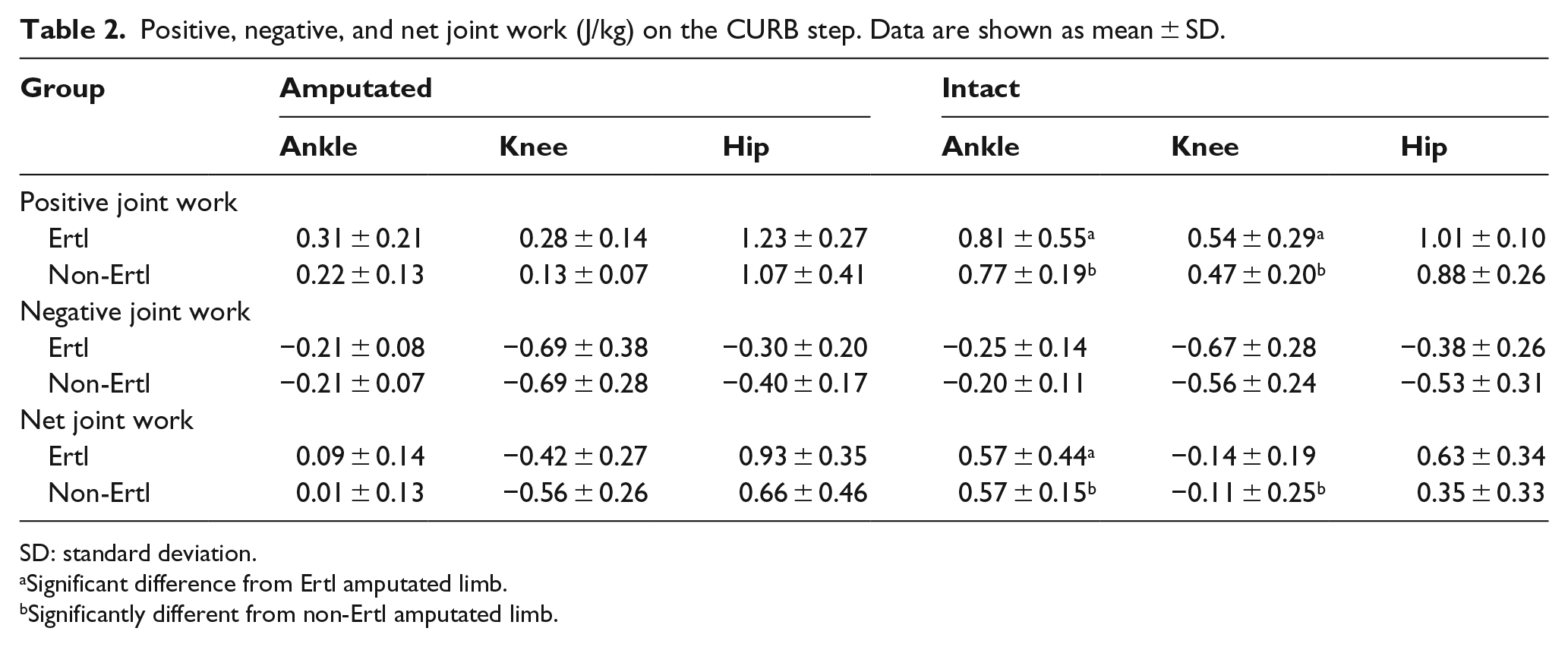
SD: standard deviation.
Significant difference from Ertl amputated limb.
Significantly different from non-Ertl amputated limb.
Net ankle work was significantly smaller for the Ertl (p = 0.005, d = 1.64) and non-Ertl (p < 0.001, d = 4.31) amputated limbs than the respective intact limbs (Table 2). Net knee work was significantly different between the non-Ertl (p = 0.002, d = 1.91) intact and amputated limbs.
Total limb work in the amputated non-Ertl limb was significantly smaller (p = 0.011, d = 1.68) than intact limb (Figure 3). However, no significant differences were found between the amputated Ertl limb and the intact limb. The contrast of net limb work between the amputated non-Ertl limb and amputated Ertl limb approached significance (p = 0.09, d = 1.07).
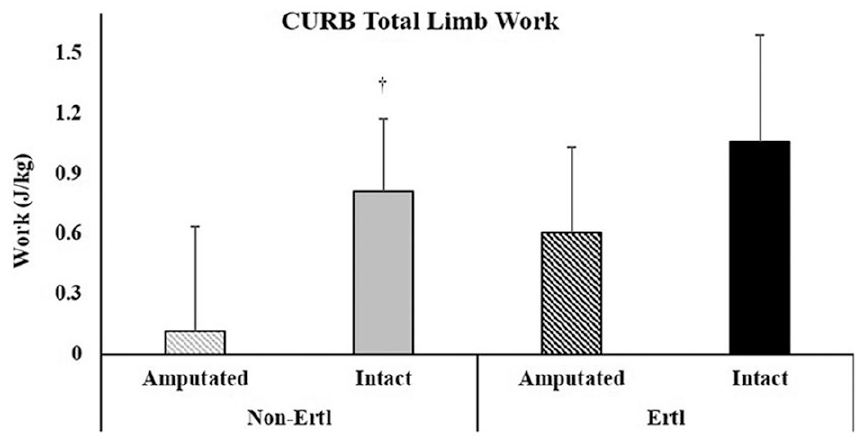
Net limb work for the CURB step.
Discussion
The main finding on the GROUND step was the amputated limb of both groups produced significantly less total limb work than the intact limb. While joint work did provide insight into individual limb contributions to the movement, work production timing during the gait cycle is unknown. To identify timing of work production, qualitative assessment of power profiles was performed post hoc; thus, these data are presented in the discussion.
The large amount of work produced by the intact limbs is primarily attributed to the power produced at the ankle (Figure 4) during the push-off phase of the gait cycle (~45%–60%). The amputated limbs produced ~78% less peak power than the intact limbs during this time. These observations are similar to those previously reported during a similar curb negotiation task in persons with TTA, even though the curb height was less than half of the current study. 9
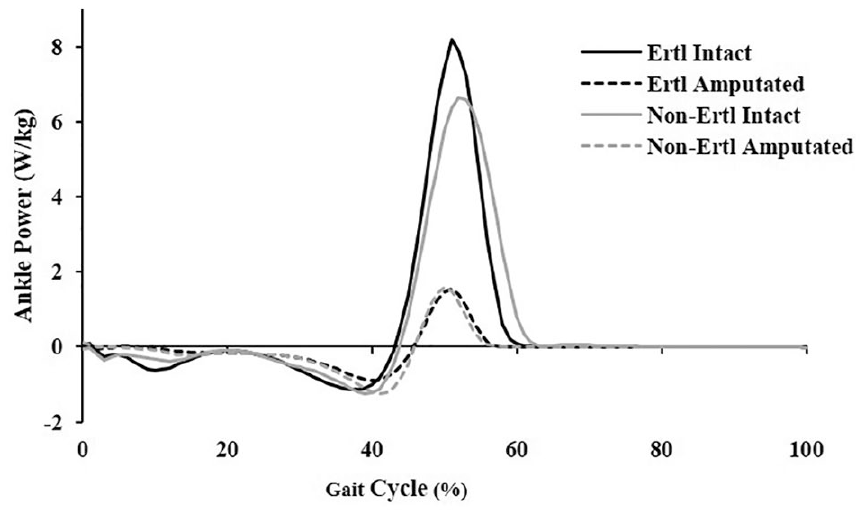
Ankle power for the GROUND step. Data series is from heel strike to heel strike.
Relative to level over-ground walking, the overall power patterns for the hip, knee, and ankle are similar to the GROUND step during curb negotiation for people with TTA.24–26 However, the magnitude (intact and amputated) of the ankle power is ~50% greater on the GROUND compared to published values of over-ground walking. This suggests that the initial stance phase of the GROUND step is similar to over-ground walking, whereas the push-off portion of the stance phase differs due to the transition from the GROUND to the CURB. The increase in push-off power assists with the translation of the body vertically onto the CURB step rather than a continuation of forward movement as in level over-ground walking. However, the intact limb positive work is still significantly larger than the amputated limb, regardless of amputation technique. This suggests that the intact limb is pushing the body up onto the CURB step with assistance from the intact ankle musculature. In contrast, the amputated limb is not capable of using the prosthetic foot/ankle to actively produce power to push up onto the CURB step from the GROUND. There is little evidence that positive work is produced at a more proximal joint to compensate for the loss of the ankle.
Results from the CURB again show the amputated limbs produced significantly less power at the ankle than the intact limbs which is consistent with previous literature showing the prosthetic foot/ankle is unable to actively generate energy. The large amount of positive knee work done by the intact limbs was consistent with the intact limb utilizing a knee strategy to traverse the CURB. When considering total limb work, the non-Ertl amputated limb produced significantly less work than the intact limb. In contrast, the Ertl amputated limb did not differ significantly from the Ertl intact limb; yet, the way in which the total limb work was produced differed. The Ertl intact limb produced a large amount of net ankle work and positive knee work; in contrast, the Ertl amputated limb produced larger net hip work and very little net ankle work. Thus, the Ertl intact limb primarily used the knee to propel the body onto and forward in the CURB, whereas the Ertl amputated limb relied heavily on the hip to traverse the CURB step. To further understand how and when this work was produced, joint powers were investigated post hoc.
Although both amputated limbs produced similar CURB ankle power profiles (Figure 5), the hip and knee power profiles showed different trends between the two amputated groups. The hip power profile (Figure 5(c)) shows the amputated Ertl limb produced larger peak hip power in early stance (~15% of gait cycle) compared to the amputated non-Ertl limb. This increase in hip power production of the Ertl amputated limb is consistent with results published for traversing a curb similar to the current task. 9 Although Barnett et al. used a lower height for curb height (7.5 cm vs 16 cm in the current study), there is a clear trend for the amputated limb (of both groups) hip joint to generate a larger peak power during early stance than the intact limb. In contrast, the intact limb of both groups generated more knee power during early stance (Figure 5). This clearly demonstrates the hip strategy used by the amputated limbs and the knee strategy used by the intact limbs.
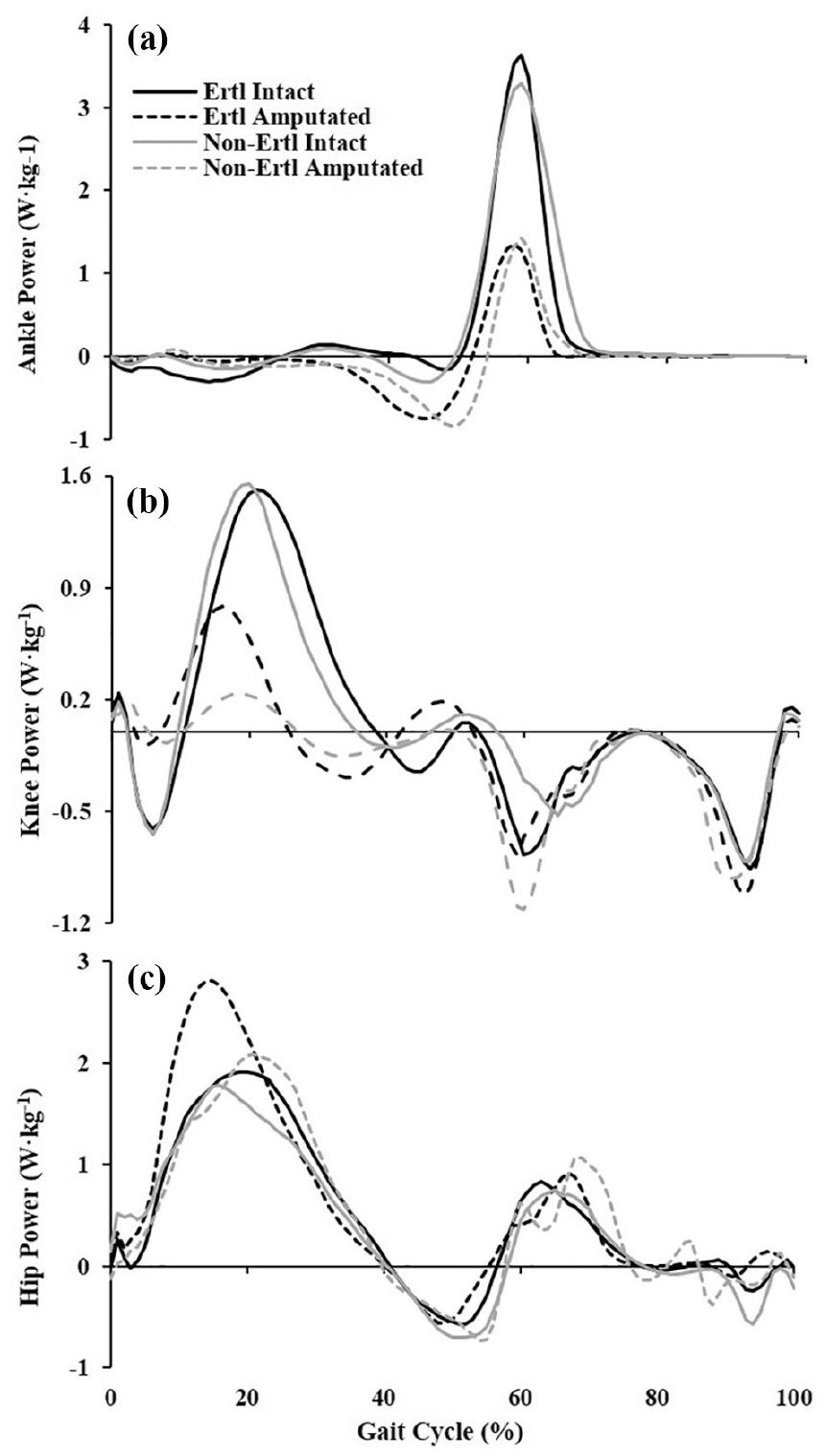
Joint powers for the (a) ankle, (b) knee, and (c) hip for the CURB step. Data are shown from heel strike to heel strike.
In comparison to Barnett et al., the peak power production at the hip is smaller than the Ertl amputated limb; however, the non-Ertl amputated limb was similar in magnitude. Two possible reasons for these differences are (1) there may be a surgical technique effect and (2) Barnett et al. included dysvascular amputees.
The hip and knee power profiles of the CURB step also resemble published hip and knee power profiles for stair ambulation.27–29 However, the overall magnitude of the hip power is lower during the CURB step than stair ambulation.27,30 This lower power production is also associated with less work produced on the CURB step than stair ambulation for all limbs. 30 Thus, these differences suggest that the demands of curb negotiation are different from stair ascent. Where stair ascent requires greater power generation to assist with vertical movement, the CURB only requires moderate power generation to ascend the single step and progress forward. Finally, curb negotiation differs further from stair negotiation due to the lack of a handrail to use for support. When participants are allowed to use a handrail for stair ascent, joint moments decrease 31 and dynamic stability increases in older adults. 32 This suggests that the presence and use of a handrail can influence how stairs are negotiated.
Although we were able to identify differences between limbs and groups, limitations existed in this current study. Socket type nor prosthetic foot type was not controlled, which may have influenced the way in which the amputated limb was used. The Ertl group was not prescribed sockets which would have allowed for the complete distal end of the residual limb to bear loads. Socket type and suspension system were not controlled to represent the general population of prosthetic users. Furthermore, the quantity of post-operative physical therapy was not controlled in this study. Although sample size was small for the study, all effect sizes were large suggesting that where significant differences were found, they were large differences.
Conclusion
This work contributes to the overall body of literature by investigating curb ascent for people with Ertl and non-Ertl TTA and evaluates biomechanical differences between the two groups. The amputated limbs of both groups have similar work and power profiles on the GROUND step and produced less work than the intact limb due to smaller ankle power production. Overall comparisons between functional outcomes of the Ertl and non-Ertl groups suggest that the Ertl amputated limb may behave differently than the non-Ertl limb by producing more total limb work on the CURB step than the non-Ertl amputated limb which was produced at the hip during early stance. The results suggest that people with Ertl amputations produce greater joint work at the hip with the amputated limb while negotiating a curb compared to the non-Ertl intact limb. However, Ertl and non-Ertl amputated limbs had similar trends of between limb work differences at the ankle and knee.
Footnotes
Author contributions
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The contents do not represent the views of the US Department of Veterans Affairs or the United States Government.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.