
Abstract
Background:
Foot orthoses have proven to be effective for conservative management of various pathologies. Pathologies of the lower limb can be caused by abnormal biomechanics such as irregular foot structure and alignment, leading to inadequate support.
Objectives:
To compare biomechanical effects of different foot orthoses on the medial longitudinal arch during dynamic gait using skeletal kinematics.
Study design:
This study follows a prospective, cross-sectional study design.
Methods:
The medial longitudinal arch angle was measured for 12 participants among three groups: pes planus, pes cavus and normal arch. Five conditions were compared: three orthotic devices (hard custom foot orthosis, soft custom foot orthosis and off-the-shelf Barefoot Science©), barefoot and shod. An innovative method, markerless fluoroscopic radiostereometric analysis, was used to measure the medial longitudinal arch angle.
Results:
Mean medial longitudinal arch angles for both custom foot orthosis conditions were significantly different from the barefoot and shod conditions (p < 0.05). There was no significant difference between the off-the-shelf device and the barefoot or shod conditions (p > 0.05). In addition, the differences between hard and soft custom foot orthoses were not statistically significant. All foot types showed a medial longitudinal arch angle decrease with both the hard and soft custom foot orthoses.
Conclusion:
These results suggest that custom foot orthoses can reduce motion of the medial longitudinal arch for a range of foot types during dynamic gait.
Level of evidence:
Therapeutic study, Level 2.
Clinical relevance
Custom foot orthoses support and alter the position of the foot during weightbearing. The goal is to eliminate compensation of the foot for a structural deformity or malalignment and redistribute abnormal plantar pressures. By optimizing the position of the foot, the medial longitudinal arch (MLA) will also change and quantifying this change is of interest to clinicians.
Background
Custom foot orthoses (CFOs) have proven to effectively manage various pathologies of the lower extremities.1–4 Pathologies associated with the lower back, upper and lower legs, as well as general foot pain can be a result of poor biomechanics, such as in altered foot alignment in pes planus (flat foot/low arch) and pes cavus (high arch).5,6 A pes cavus foot typically presents with an uneven distribution of weight along the metatarsal heads and lateral border of the foot and tends to have a more rigid medial longitudinal arch (MLA), whereas a pes planus foot often demonstrates a flat-footed gait with no toe-off, a large plantar weight-bearing surface with the most pressure on the first and second metatarsals and exaggerated pronation, keeping the foot in a flexible and unstable position. 5 Both foot abnormalities may lead to inadequate shock dissipation and place added stresses on the lower limb.5,7
CFOs are designed to place the foot into a different, more biomechanically advantageous position during gait to improve the body’s overall ability to weightbear. 5 Additional applications for orthotic devices are to provide relief by redistributing abnormal plantar pressures and provide support to the joints of the foot in the position most desirable for weight-bearing activities, eliminating the need for the foot to compensate for a structural deformity or malalignment.8,9 To achieve a more ideal weight-bearing position, CFOs are often casted in a subtalar joint (STJ) neutral position,10,11 and therefore, wearing CFOs will adjust foot posture closer to STJ neutral. Quantifying the kinematics of these changes is of interest to foot specialists.
Measuring the skeletal kinematics includes tracking the full 6 degrees of freedom of the foot bones using biplane x-ray fluoroscopy with markerless radiostereometric analysis (RSA). 12 This method avoids skin motion artefact error, typical of optical motion capture, and since the bones are tracked directly by creating three-dimensional (3D) models of each bone from a computed tomography (CT) scan, it can be used with different kinds of footwear. Dynamic studies using biplane fluoroscopy have been used to determine the effects of footwear on the motion of the tibiotalar and STJs 13 as well as the navicular drop and navicular drop rate in minimalist, stability and motion control shoes. 14 Markerless RSA has been previously used to quantify the angle of the MLA for barefoot and shod conditions 15 ; however, there is no current literature discussing the effects of foot orthoses on foot kinematics using this method.
There is a great deal of variability in the materials used during the process of constructing CFOs. Researchers have completed studies using insoles with varying degrees of customized support – from ready-to-wear, off-the-shelf (OTS) insoles that require no modification to heat mouldable insoles where the medial arch and heel cup become moulded to the shape of the foot, to completely custom-made orthotic devices that are created based on a 3D positive plaster cast of the foot.
The purpose of this study was to determine the effect of three different insoles on the MLA during dynamic gait including one hard CFO, one soft CFO, and an OTS device (Barefoot Science©). The MLA angle was measured using markerless RSA and then compared between five conditions including barefoot and shod, within three groups of participants: pes planus (low arch), pes cavus (high arch) and normal arch. First, it was hypothesized that the hard orthosis would have a greater effect on arch angle, showing a larger decrease MLA angle than the soft orthosis. In other words, the arch height would be more stable and higher compared to the soft orthosis. Second, we thought the OTS device would show a smaller effect on the MLA angle, measuring the smallest mean angle decrease compared to barefoot and shod walking.
Methods
Participants
A total of 18 participants (mean: 29.1 years, 68.6 kg) provided informed consent in accordance with the relevant ethics review board. Each participant was assessed by a foot specialist, a Canadian Certified Pedorthist (C.Ped(C)) trained in the profession for 8 years at the time of the study (C.D.). The foot specialist assigned participants to the proper group – six to each group of normally arched, pes cavus and pes planus feet, based on a sample size calculation performed prior to the research with an effect size estimate. The foot specialist completed visual and functional assessments including rearfoot inversion/eversion, forefoot adduction/abduction and ankle plantar and dorsiflexion during gait. The participants fit the same criteria as described by Balsdon et al. (2016): pes cavus participants exhibited a high navicular height combined with rearfoot inversion, forefoot adduction and an arch that tended to be more rigid, whereas pes planus participants exhibited low navicular height combined with rearfoot eversion and forefoot abduction. 15 Normal, asymptomatic participants were examined to make sure they possessed an average navicular height and no irregular foot and ankle movement during gait. Participants were excluded if they had foot abnormalities such as hallux valgus or previous surgery on the lower limbs. No pes planus participants had adult-acquired flatfoot deformity (AAFD), and none of the participants had a frontal plane forefoot deformity.
All participants were casted by the same foot specialist who completed their initial assessment (C.D.). The casting was done using the semi-weightbearing foam box casting method, with the patient in a relaxed standing position. CFOs were fabricated with 3 mm Plastazote (soft) or Subortholen (hard) (Figure 1) thermoplastic materials for the shell and 45D EVA posting, covered with a 3-mm multiform top cover. Barefoot Science© insoles claim to provide pain relief through rehabilitation and strengthening of the foot; specifically, they ‘work to build arch strength by stimulating the muscles in the foot, building strength over a short period of time’. 16 Each orthotic device was worn in neutral cushioning running shoes for testing (New Balance model #882).

(Top left) Custom-made soft (Plastazote) orthosis, top right) custom-made hard (Subortholen) orthosis and (bottom) Barefoot Science© off-the-shelf insole with four levels of support.
Data collection
Participants stepped beside the laterally placed fluoroscope at their preferred pace aligning their left heel with a mark on the platform, determined during static resting foot posture and subtalar neutral positions. 15 Two trials were collected for each condition to ensure proper gait and to make sure that the calcaneus, navicular and first metatarsal were visible in both fluoroscopic videos through stance phase. Participants wore a lead wrap-around vest, kilt and thyroid shield during all trials (Figure 2).
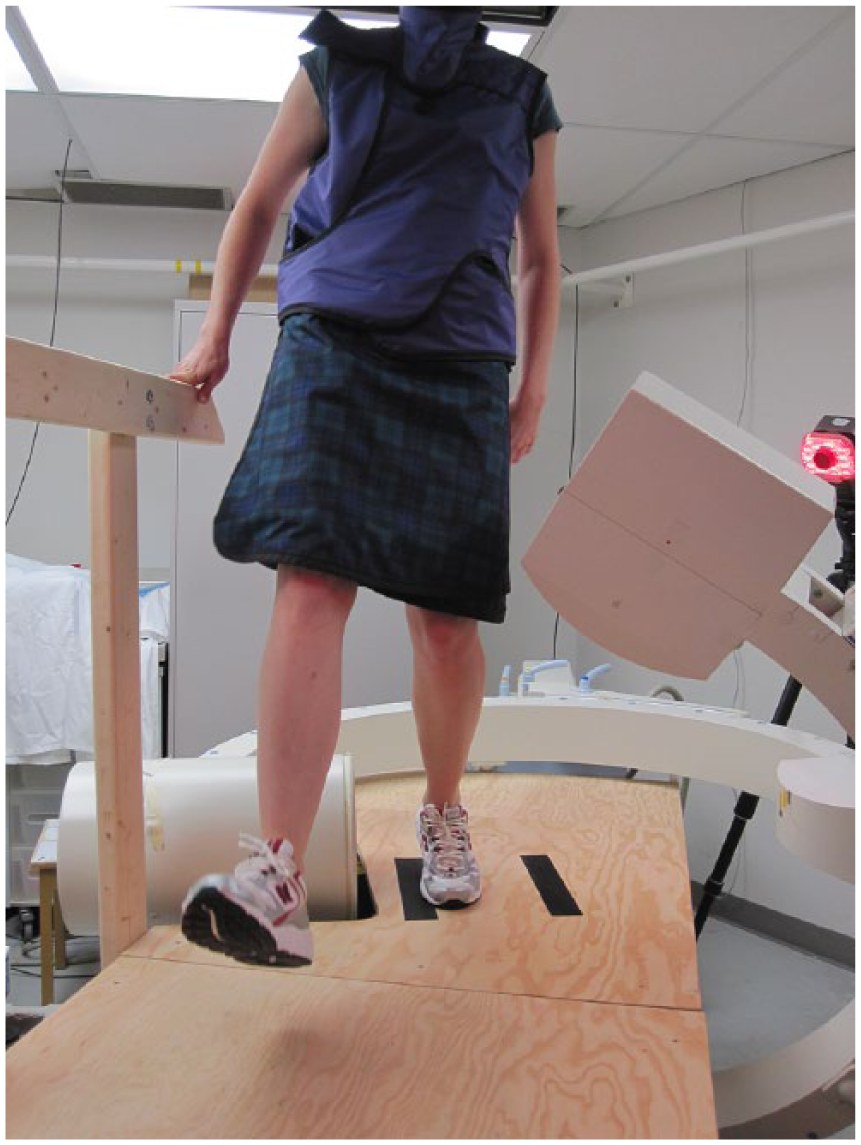
Participant walking on wooden platform during data collection.
Fluoroscopic x-ray videos were collected at 30 frames per second. All frames were extracted to tagged image file format (.TIFF) from the dynamic fluoroscopic videos and were of best quality during midstance as the foot supported the body’s weight (Figure 3). Two to four images at flatfoot of midstance were selected for each condition to quantify the arch angle when the left foot was directly under the body’s weight, and the largest angle within’ those frames was compared between barefoot, shod and orthosis conditions. Following data collection, participants were set up to get a CT scan of their left foot to create 3D models for post-processing.
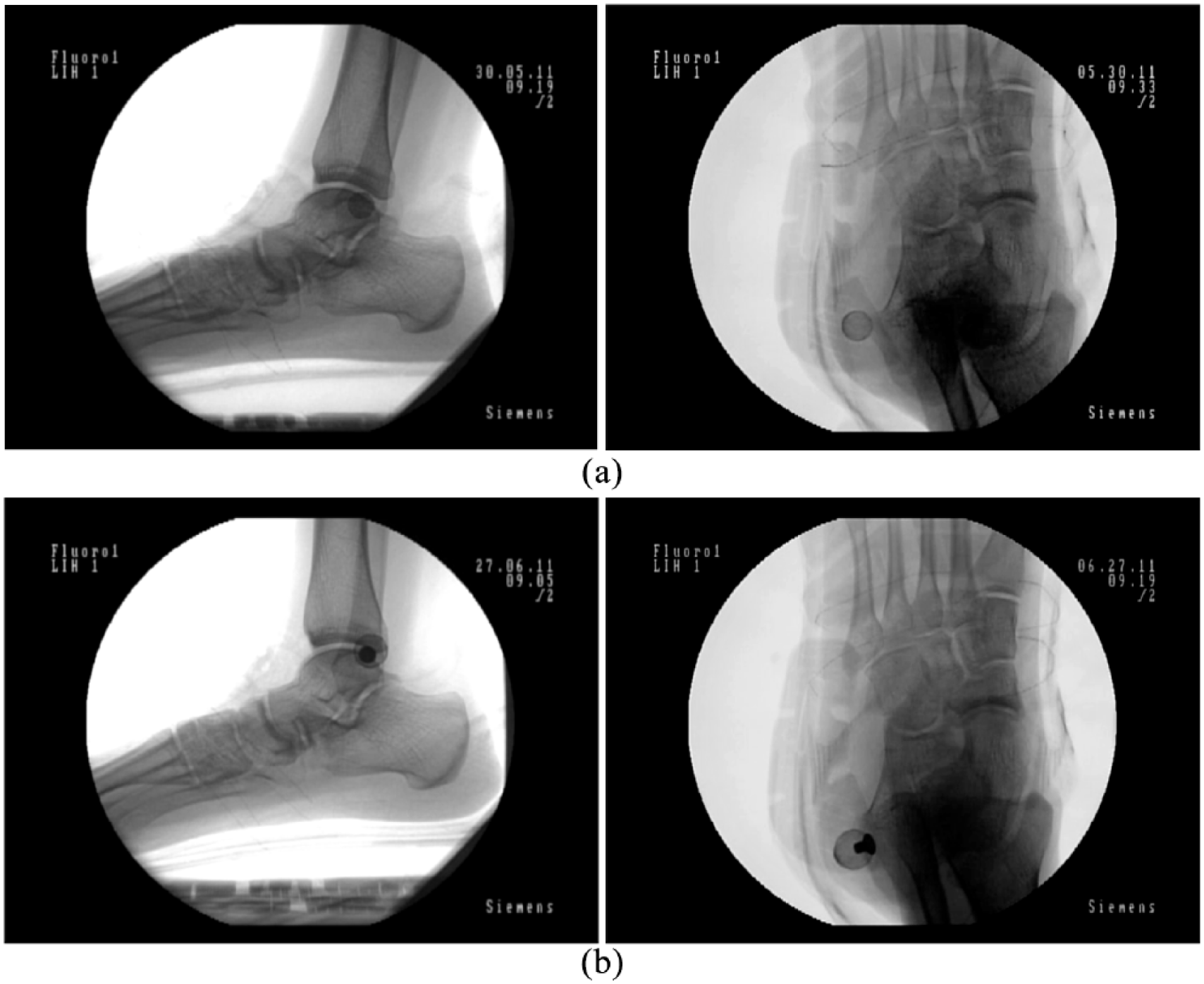
Pes planus participant images from the lateral view (fluoroscope A) and anterior–posterior oblique view (fluoroscope B): conditions are (a) neutral cushion running shoe and (b) soft orthosis in a neutral cushion running shoe.
Calibration
Two 9-inch fluoroscopes (SIREMOBIL Compact-L mobile C-arms; Siemens Medical Solutions Canada Inc., Mississauga, ON, Canada) were calibrated using a calibration frame with orthogonal fiducial and control planes and the relative angles of the fluoroscopes less than 135° (Figure 4). 17 A distortion grid was placed on the image intensifier of each fluoroscope following data collection to correct for pin cushion distortion.18,19 The position of the beads on both the calibration and distortion images was manually located using a custom written algorithm (MATLAB; The MathWorks, Natick, MA, USA), which established the laboratory coordinate system and the locations of the x-ray foci with respect to the lab.17,19 A series of custom written algorithms, developed and validated for markerless RSA were used to acquire the fluoroscope and image plane parameters to reconstruct the experimental setup. 12
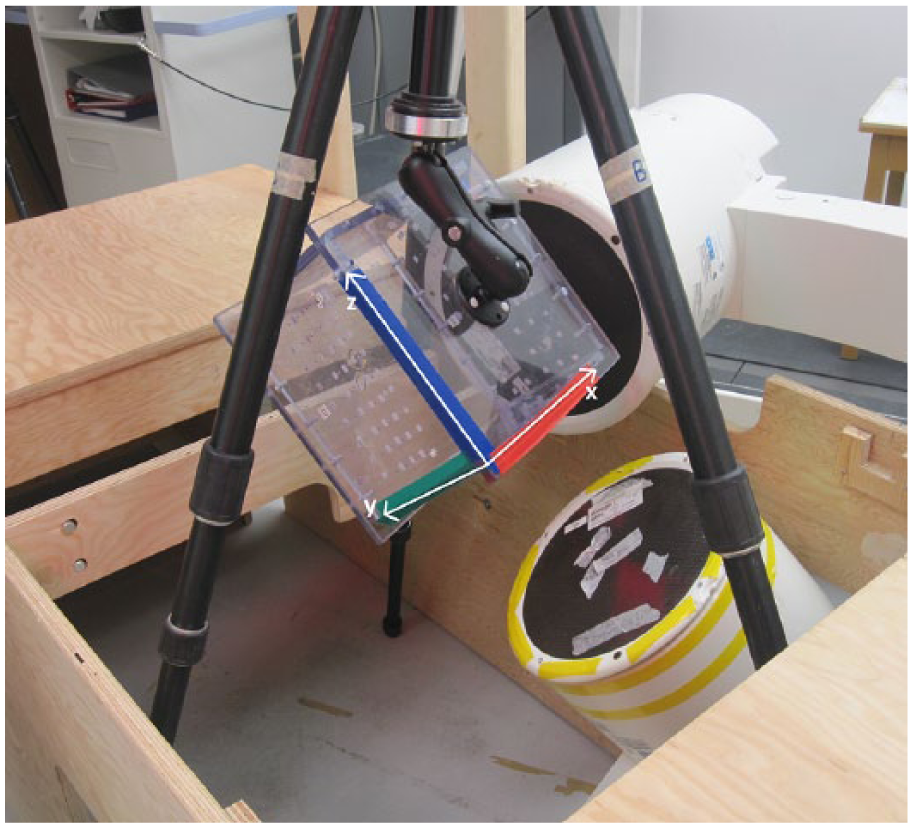
Calibration of both fluoroscopes with a calibration frame with axes x, y, z, indicated by white axes drawn on the image.
Data processing
The 3D models were created manually by segmenting the participants’ CT scan for the navicular, calcaneus and first metatarsal using open-source image processing and DICOM viewing software (OsiriX; Pixmeo, Geneva, Switzerland). The three bone models were exported as object files (.obj) and then imported into the virtual experimental setup in modelling software (Rhinoceros; Robert McNeel & Associates, Seattle, WA, USA). The bones were manually ‘matched’ to the two image planes, meaning their positions and orientations in three-space were manipulated in order to replicate the bone’s silhouette on both two-dimensional images. 15 Following matching, the locations of three bony landmarks were exported into a spreadsheet – the medial process of the calcaneus, the most medial point on the navicular tuberosity and the anterior position on the first metatarsal head.
Custom-written MATLAB software calculated the angle created by these three bony landmarks in the laboratory coordinate system using the dot product of two vectors, from the navicular tuberosity to the medial process of the calcaneus and the navicular tuberosity to the first metatarsal head. 15
Statistical analysis
Statistical analysis was performed using SPSS (IBM Corporation, Armonk, NY, USA). Multivariate and repeated measures general linear models were used to determine whether there were statistical significances between barefoot and orthosis conditions, for all participants as well as within foot type. Multivariate analyses of variance (MANOVAs) were completed for a similar analysis to determine differences between shell materials for CFOs. Statistical significance was set at p < 0.05 and a Bonferroni correction was used to compare both between-subjects and within-subjects’ factors, foot type and footwear condition, respectively. Within-subjects’ effects were corrected using Greenhouse–Geisser estimates of sphericity.
Results
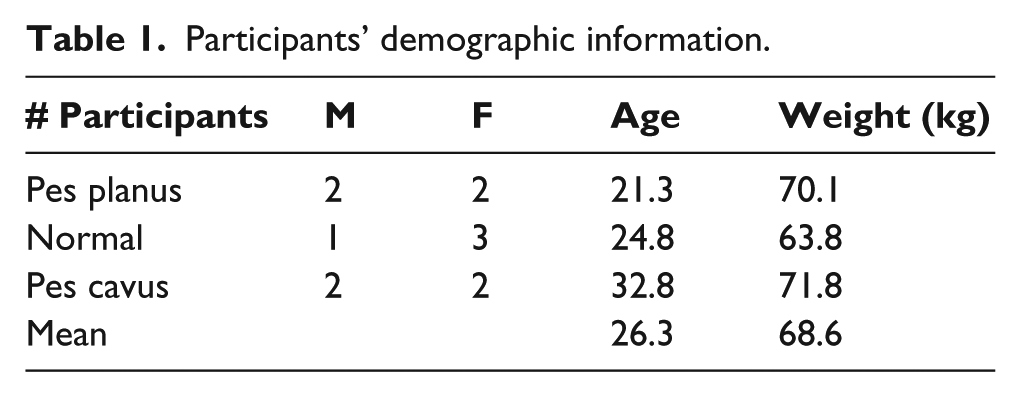
Of the eighteen participants, 6 were excluded from the analysis. Two participants did not complete the study, and four others were not included in the data analysis due to post-processing difficulties for one or more conditions. Therefore, data from 12 participants were included in the analysis (Table 1). Mean MLA angles for the five conditions including overall mean, as well as mean angles by foot type, are shown in Table 2, and graphically in Figure 5. Table 3 shows the differences in MLA angle and Cohen’s d effect sizes between the three insole conditions compared to both barefoot and shod walking for the three foot types, and the mean differences for all participants.
Participants’ demographic information.
Measured MLA angles with their standard deviations between barefoot and four footwear conditions during dynamic gait.
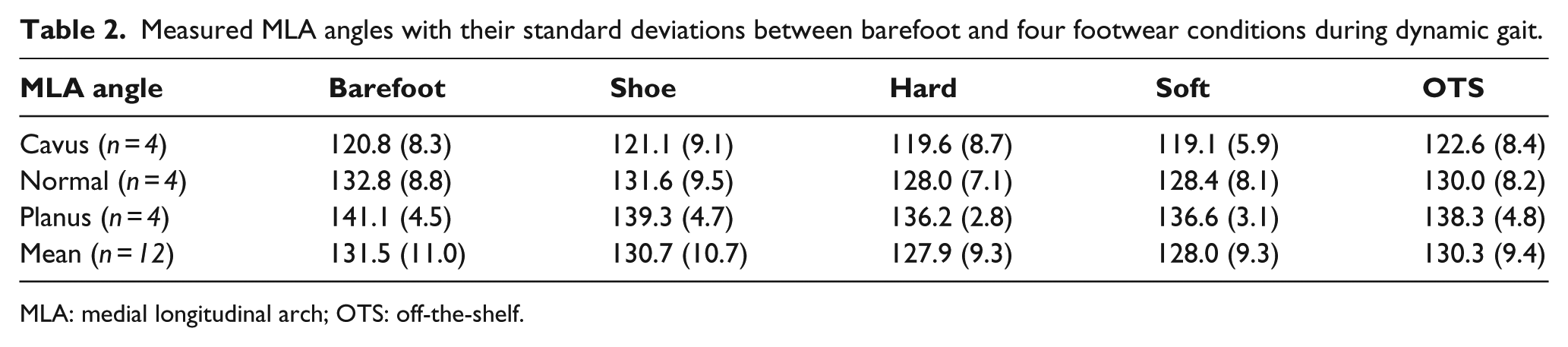
MLA: medial longitudinal arch; OTS: off-the-shelf.
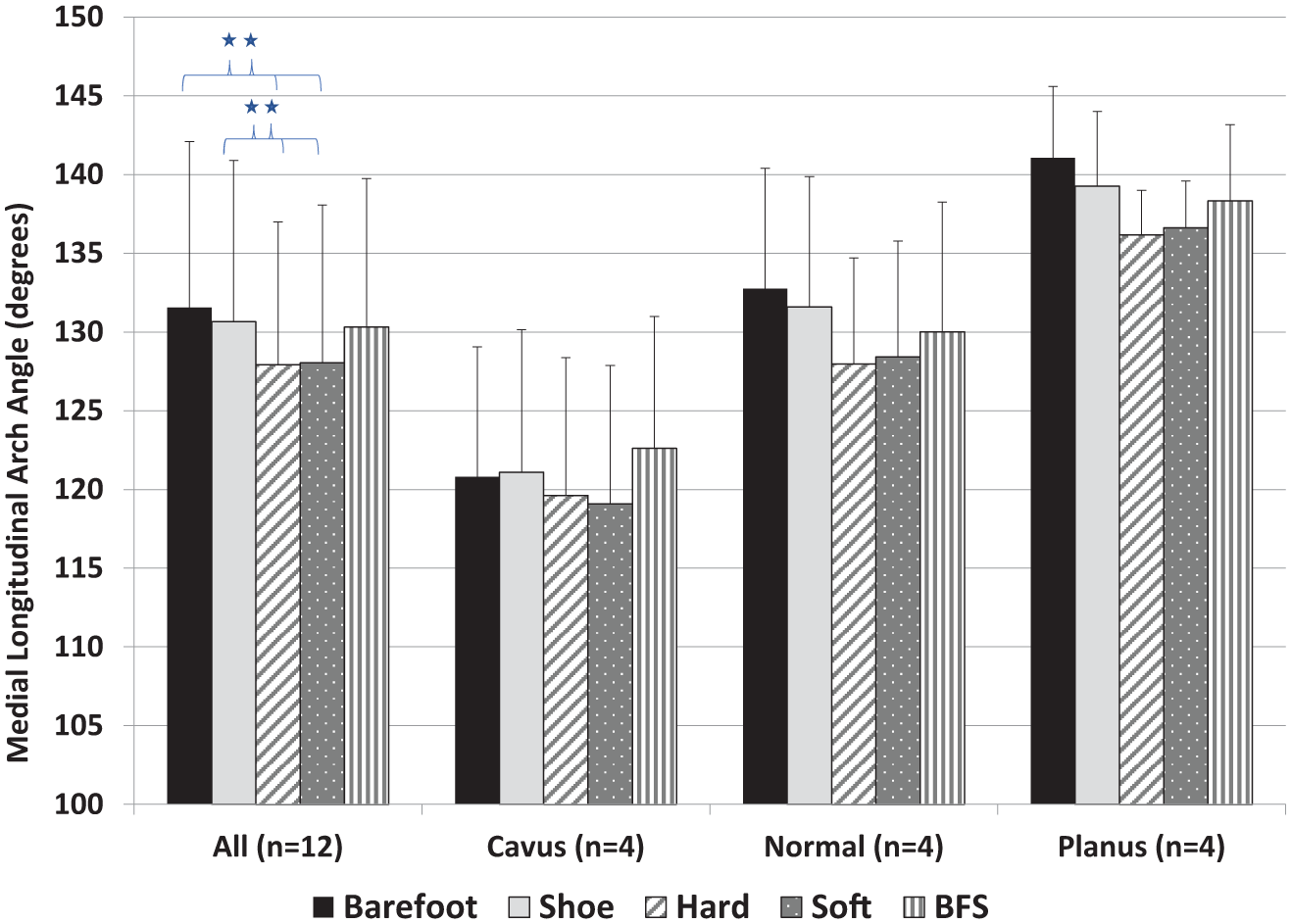
Average medial longitudinal angles of all participants. Conditions are comparing soft and hard shell materials of custom foot orthoses, an off-the-shelf device as well as barefoot and shod conditions. Error bars denote 1 standard deviation. Statistically significantly different conditions are indicated with an asterisk (*).
Mean MLA angle differences between three different insoles compared to both barefoot and shod conditions.
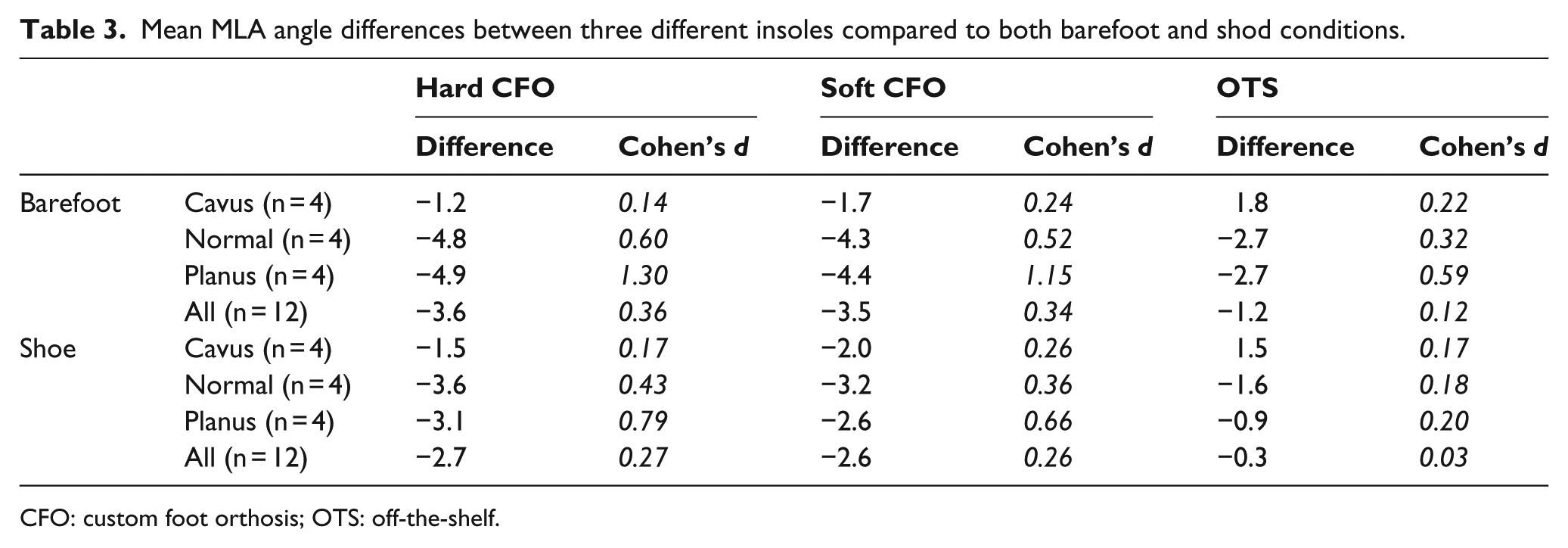
CFO: custom foot orthosis; OTS: off-the-shelf.
A statistically significant interaction was found for within-subjects effects with a Greenhouse–Geisser correction F(3.38,30.4) = 9.86, p < 0.001, η 2 = 0.523. Tests of within-subjects’ contrasts revealed that both the hard (p = 0.002) and soft (p < 0.001) orthoses were significantly different from the barefoot condition, whereas the shod and OTS conditions showed no differences to barefoot gait (p = 0.253 and p = 0.163, respectively). Post hoc analysis revealed statistically significant between-subjects effects F(2,9) = 6.44, p = 0.0184, η 2 = 0.588, between pes cavus and pes planus participants (p = 0.0177).
A statistical analysis was also executed without the barefoot condition, since custom orthotic and OTS devices are always worn in a shoe. For the four conditions – shod, hard CFO, soft CFO and OTS – a significant interaction was found for within-subjects effects with a Greenhouse–Geisser correction F(2.50,22.5) = 8.35, p = 0.001, η 2 = 0.481. Tests of within-subjects’ contrasts revealed that both the hard (p = 0.001) and soft (p = 0.003) orthotic conditions were significantly different from the shod condition, whereas the OTS insole showed no difference to shod gait (p = 0.712) (Table 4).
The p values (95% confidence intervals) from pairwise comparisons of four conditions – custom foot orthoses (hard and soft shell materials), an off-the-shelf orthosis and running shoe.
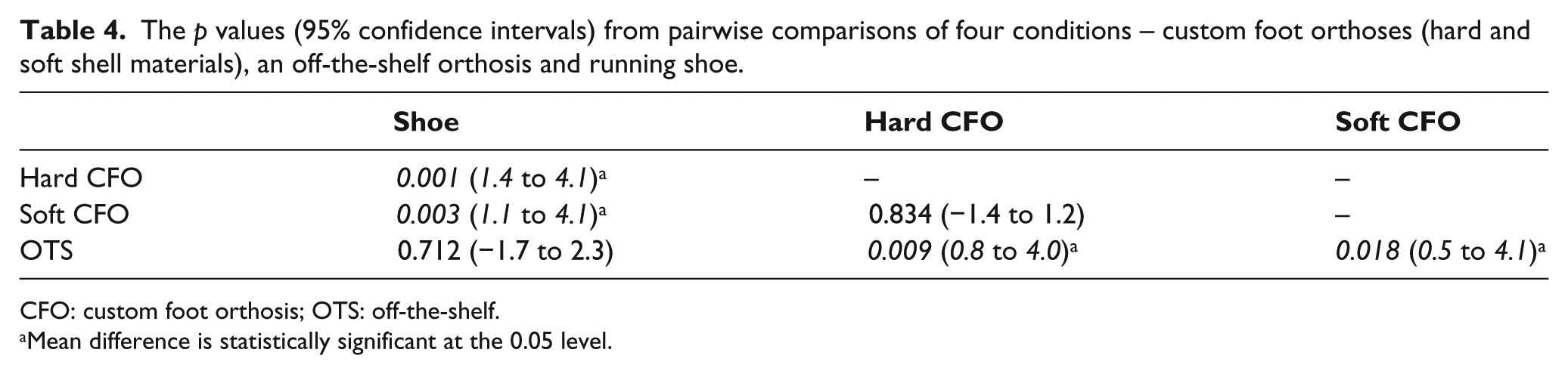
CFO: custom foot orthosis; OTS: off-the-shelf.
Mean difference is statistically significant at the 0.05 level.
Discussion
The objective of this research was to determine how the kinematics of the MLA are affected by different types of foot orthoses. Data were collected for three different groups and for five footwear conditions – barefoot, shod, two CFOs and one OTS insole. Results showed an average decrease in mean MLA angles with all orthotic devices compared to barefoot walking. Our first hypothesis was not proven as the hard CFO did not result in a smaller arch angle (higher arch height) compared to the soft CFO. Both CFOs resulted in an MLA angle decrease for every foot type (Table 3), and the differences between hard and soft CFOs were not statistically significant. Our second hypothesis was confirmed since the OTS insole had a smaller effect (smaller change in MLA angle) compared to both custom orthotic devices across all foot types.
The CFO findings were consistent with a cadaveric study that saw an increase in arch height in millimetres with two types of orthotic devices in flatfeet. 20 This comparison is made such that an increase in arch height in millimetres can be equated to a decrease in arch angle in degrees, as measured in this study.
Barefoot MLA angles have demonstrated differences between foot types, 15 which may have influenced the MLA changes within groups while wearing the orthoses. The pes cavus group demonstrated the smallest MLA angle change of the three groups while wearing orthoses, likely due to the nature of a pes cavus foot type which will tend to be more rigid and elongate less during loading. 5
The greatest differences with orthoses were expected in the pes planus participants since this foot type – low navicular height, an everted calcaneus and excessive pronation of the forefoot – requires the greatest correction to be in an ideal weight-bearing position. 5 By raising the arch in pes planus participants, orthotic devices support the plantar aspect of the foot while controlling maximum pronation. 21 A previous study used static dual-plane radiographs to investigate alignment in pes planus patients with and without CFOs in the participants’ shoes. 22 Investigators determined that the use of foot orthoses had a normalizing influence on the measured angles and that the improved alignment with the custom insoles was statistically significant. 22 A similar result was found in our study – an overall decrease in MLA angle for the pes planus group; however, this study measures the MLA angle under dynamic conditions rather than alignment during static standing.
In a normal foot structure, the lateral portion of the MLA rests on the ground, which provides absorption of forces across all five metatarsal heads and additional support to the foot. 5 Our study shows that a CFO raises the arch, relieving stress on the soft tissue of the plantar aspect of the foot; however, CFOs are not typically prescribed to asymptomatic individuals. The OTS device also showed a decrease in MLA angle for the normal foot type, but to a lesser degree than the CFO. This decrease was also not statistically significantly different for any foot type. Previous literature has reported on the multi-segment foot kinematics of healthy participants with a normal arch height while wearing three different over-the-counter orthoses, showing that MLA deformation was not reduced for any device. 23 There is no current literature reporting the efficacy of the Barefoot Science© insole which claims to strengthen the foot by stimulating the muscles of the foot. 16 However, a longitudinal study may be more appropriate to evaluate the correctness of this claim.
No differences in MLA angle were apparent between hard (Suborthlen) and soft (Plastazote) materials. These findings are in agreement with a previous study that compared hard, medium and soft prefabricated orthoses and found no significant differences in kinematics of the lower extremity between the orthoses conditions. 24 This study used optical motion capture on the lower extremity with only two markers to represent the foot and therefore did not measure the kinematics of the MLA specifically.
It was anticipated that a harder shell material would have supported the MLA more, due to increased rigidity, restricting the arch from elongating and thus leading to an overall smaller MLA angle. Rigid orthoses have previously shown to limit foot mobility and resulted in the highest static arch height index (AHI) measure during 90% weight-bearing compared to soft and semi-rigid orthoses. 21 Another study demonstrated soft-flat and contoured orthoses to be a priority over medium and hard orthoses with identical contouring, demonstrating a significantly greater comfort level during dynamic walking. 25
Although our study did not measure perceived comfort among participants, previous literature has shown that short-term comfort reduced the incidence of injury frequency while using insoles that were perceived as comfortable to study participants, suggesting comfort is a possible predictor of success with foot orthoses. 26
One limitation of this study is the small sample size analysed. There is limited literature on the measurement of the MLA angle, especially with the use of fluoroscopy; therefore, additional data may support more definite trends between conditions and foot types. A sample size calculation was performed in the planning stages of this research where six participants per group were recruited to meet anticipated statistical requirements. Further research should include a larger sample size, focusing on a single foot type and/or pathology, and correlate the objective results to the function and pain scales experienced by the study participants.
A second limitation is that the dynamic gait task performed during data collection cannot be considered typical walking gait. The first step from rest was collected for each condition, similar to a gait initiation task executed in a previous study. 15 The literature states that the first four strides show an increase in walking speed; thus, a person’s walking gait cannot be considered their average speed until the fifth stride. 27
Strengths of this study lie in the innovative method used to acquire the data. RSA and markerless RSA are very accurate methods to evaluate skeletal kinematics; approximately 0.1° and 0.5 mm error measurements were determined following markerless RSA validation on the shoulder joint. 12 Although the sample size is small, we are confident that the significant findings shown in this research represent the overall trend in changes of the MLA angle with foot orthoses compared to barefoot and shod walking.
Conclusion
This research is an objective study quantifying the effect that CFOs and OTS insoles have on the kinematics of the foot and the first of its kind to do so with bi-planar fluoroscopic RSA. Performing a dynamic task in both hard and soft CFOs resulted in a significantly higher MLA height compared to the shod condition, suggesting that foot orthotic devices can reduce motion of the MLA for a range of foot types.
Supplemental Material
825607_supp_mat_STROBE_checklist_POI_-_MBalsdon – Supplemental material for Hard, soft and off-the-shelf foot orthoses and their effect on the angle of the medial longitudinal arch: A biplane fluoroscopy study
Supplemental material, 825607_supp_mat_STROBE_checklist_POI_-_MBalsdon for Hard, soft and off-the-shelf foot orthoses and their effect on the angle of the medial longitudinal arch: A biplane fluoroscopy study by Megan Balsdon, Colin Dombroski, Kristen Bushey and Thomas R Jenkyn in Prosthetics and Orthotics International
Supplemental Material
Supplemental_Material_-_OsiriX_Segmentation – Supplemental material for Hard, soft and off-the-shelf foot orthoses and their effect on the angle of the medial longitudinal arch: A biplane fluoroscopy study
Supplemental material, Supplemental_Material_-_OsiriX_Segmentation for Hard, soft and off-the-shelf foot orthoses and their effect on the angle of the medial longitudinal arch: A biplane fluoroscopy study by Megan Balsdon, Colin Dombroski, Kristen Bushey and Thomas R Jenkyn in Prosthetics and Orthotics International
Footnotes
Acknowledgements
The authors would like to thank Angela Kedgley and Anne-Marie Fox (Allen) for their aid and guidance with the procedure and post-processing of the study. The authors would also like to thank Cheryl Beech for her assistance with the submission process.
Author contribution
Megan Balsdon wrote the initial draft of the manuscript, edited the manuscript, and took the photos included in the manuscript. Colin Dombroski was the Certified Pedorthist mentioned in the study, and assisted in the editing of the manuscript. Kristen Bushey assisted with data collection, the editing and taking of photos, as well as editing the manuscript. Thomas Jenkyn reviewed the manuscript and provided feedback.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a Discovery Grant from the Natural Sciences and Engineering Research Council (NSERC).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.