
Abstract
Background:
Lateral epicondylitis is one of the most common causes of elbow pain. It is generally observed in people between the ages of 40 and 50 years, and the dominant extremity is more frequently affected. Various noninvasive methods are frequently used; however, studies investigating the effectiveness of the orthoses are limited and with controversial outcomes.
Objective:
To investigate the effectiveness of a hand-wrist resting orthosis and an epicondylitis bandage in lateral epicondylitis.
Study design:
Randomized controlled trial.
Methods:
In total, 82 patients diagnosed with unilateral lateral epicondylitis were enrolled into the study. Hand-wrist resting orthosis was applied to 45 patients and epicondylitis bandage was applied to 41 patients. Patients were evaluated before treatment and at 6 weeks after treatment with a Visual Analogue Scale; Disabilities of the Arm, Shoulder, and Hand questionnaire; the Short Form 36; and a determination of hand grasping force.
Results:
Both groups were similar in terms of age, body mass index, gender, frequency of lateral epicondylitis on the dominant side, dominant extremity, and duration of complaints (p > 0.05). A statistically significant recovery was detected in both groups between the pre-therapy values and the values at the sixth week in terms of Visual Analogue Scale scores; Disabilities of the Arm, Shoulder, and Hand questionnarie scores; hand grasping forces; and the Short Form 36 mental and physical component scores (p < 0.05). However, there were no significant differences detected between the two therapy methods before the therapy and at the sixth week of treatment in all parameter values (p > 0.05).
Conclusion:
Our results suggest that both epicondylitis bandage and hand-wrist resting orthosis are effective treatment options for lateral epicondylitis–induced pain, functional status, muscle strength, and quality of life. Furthermore, neither treatment option was superior to the other. Large, randomized studies are necessary for more clear statements.
Clinical relevance
Epicondylitis bandage and hand-wrist resting orthosis are equally effective treatment options for lateral epicondylitis–induced pain, functional status, muscle strength, and quality of life.
Lateral epicondylitis (LE) is one of the most common causes of elbow pain. It is generally observed in people between the ages of 40 and 50 years, and the dominant extremity is more frequently affected.1–3 The pathophysiology of LE is still controversial. However, overuse of wrist extensor muscles, especially the extensor carpi radialis brevis (ECRB) muscle, which adheres to the lateral epicondyle of the humerus, is considered as an etiological factor.4–6
Clinical improvements have been reported in 75%–90% of LE patients with appropriate conservative treatments. Surgical procedures may be required for 10% of the cases that do not respond to conservative treatments. Many treatment modalities have been tested for conservative treatment. Hand-wrist resting orthosis (HWRO) and epicondylitis bandage (EB) are splinting methods frequently used for treatment of LE.1,7,8
Although such methods are frequently used, studies investigating the effectiveness of the orthoses are limited, and their outcomes are controversial. In this study, we aimed to compare the effectiveness of HWROs and EBs in patients with LE to enable health professionals to make conscious choices regarding LE treatment and orthosis preferences taking patients’ views into consideration.
Materials and methods
We enrolled 100 patients into this study who had applied to the Physical Medicine and Rehabilitation polyclinic with complaints of pain on the lateral side of the elbow. These complaints had continued for at least the past 12 weeks, and the patients were ultimately diagnosed as having unilateral LE after a clinical examination and ultrasonography (USG).
Detailed medical histories were taken, and physical examinations were performed in all patients. The patients were randomly divided into two groups that included the HWRO and EB groups. This study was approved by the local medical ethics committee. Informed consent was provided by all patients.
Patients with a history of elbow surgery, elbow injection, or any elbow treatment within the previous 3 months were excluded from the study. In addition, those with a chronic, rheumatologic, or psychiatric disease were excluded. Furthermore, patients were excluded if they had other factors that could lead to elbow pain, other than LE, including shoulder and wrist problems, cervical radiculopathy, cervical myelopathy, and entrapment neuropathy of the upper extremity.
Patients were divided into two groups: group 1 had 50 patients who were given the HWRO, and group 2 had 50 patients who were given the EB.
The HWRO is an orthosis that includes a polyethylene bar holding the wrist at 15–20° extension. The splint wraps the wrist and distal side of the forearm without wrapping and limiting finger movements. Since keeping the wrist at 15–20° extension is the most suitable position for hand function, the HWRO was used while the wrist was at this position (Figure 1).

Hand-wrist resting orthosis (HWRO).
The EB consists of a pad and strap that applies pressure on the forearm muscles. The size of the EB was determined by the physician who examined the patient. The EB was applied 5 cm distal to the lateral epicondyle to allow elbow flexion (Figure 2). After the EB was applied, patients were asked to make a fist and, at that point, the belt on the EB was compressed. If the pressure applied to the forearm was comfortable after the fist was opened, the EB was considered suitable. Patients were taught to use the EB in this way. 9

Epicondylitis bandage (EB).
Patients in both groups were told to use their respective devices during daily activities for 6 weeks and to avoid activities causing pain. They were also asked to put the devices on during the day, to perform wrist extensor stretching exercises, and to apply any standard treatment suggestions (e.g. ice application). Patients were also told to remove the devices when they were performing stretching exercises, bathing, and sleeping. 10
In group 1, 7 of the 50, and in group 2, 11 of the 50 patients were excluded because they had not used their devices or had not come to the control examination after the therapy. Consequently, 43 patients in group 1 and 39 patients in group 2 were assessed statistically. All cases were assessed before treatment and at the sixth week of treatment.
Maximum hand grasping force (HGF) was evaluated with a Jamar® dynamometer. Pain levels during a maximum hand grasp and during rest were evaluated with a Visual Analogue Scale (VAS; range of 1–10). The functional and disability level of the upper extremity was determined with the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire. Health-related quality of life was determined with the Medical Outcomes Study 36-item Short Form 36 (SF-36) Health Survey.
The DASH is a questionnaire developed to assess functional cases and symptoms in musculoskeletal disorders of the upper extremities. Furthermore, the Turkish reliability for this questionnaire has been confirmed.11,12
The DASH consists of three sections. The first section consists of 30 questions: 21 questions evaluate the degree of patient struggling during daily activities, five questions evaluate symptoms (pain, activity-induced pain, sexual activities, hardness, weakness), and the remaining four questions evaluate social functions, work, sleep, and self-confidence. The first section determined the function/symptom (DASH-FS) score of the patient. Patients marked suitable responses based on a 5-point Likert-type scale (1: no difficulty, 2: slight difficulty, 3: intermediate difficulty, 4: severe difficulty, and 5: unable to perform). According to the DASH questionnaire outcomes, results between 0 and 100 are obtained from each section (0: no disability and 100: maximum disability).
Measurements for HGF were performed with the Jamar hand dynamometer while the subjects were at a standing position and the elbow and wrist joints were at full extension. HGF measurements have shown reliable results with the Jamar hand dynamometer.13,14
Measurements were performed between 10:00 and 12:00 in the morning and 1-min rests were given between the measurements to reduce the effects of muscular fatigue. Measurements were repeated three times, and an average value was calculated and recorded in kilograms. Patients were also asked to avoid the use of any analgesic agents within the last 24 h before the evaluation.
The SF-36 is a scale that includes 36 items and may be completed by the patient. Both the validity and reliability of this scale for musculoskeletal disorder patients have been confirmed. 15 This scale is used to determine the patient’s quality of life. The SF-36 includes eight different parts related to health. These parts include physical function, social function, role restrictions dependent on physical problems, role restrictions dependent on emotional problems, mental health, healthiness, pain, and general health. Scores for each part were coded and converted into a scale between 0 (the worst) and 100 (the best). The physical and mental health subsection scores were calculated according to the results obtained from the subscales. There are two summary scales, including the Physical Component Scale (PCS) and the Mental Component Scale (MCS).
Statistical analysis
The Statistical Package for the Social Sciences (SPSS), version 20, was used for statistical analysis. Descriptive statistical results are shown as the mean ± standard deviation (SD). Baseline characteristics of both groups were compared with chi-square tests or t tests depending on which test was appropriate. Before and after treatment results were evaluated through paired-sample t tests. The percentage change of both groups before and after the treatment was evaluated by using analysis of variance (ANOVA). Statistical significance and confidence intervals (CIs) were determined as p < 0.05 and 95% CI, respectively.
Results
There was dominant side involvement in 88.4% and 79.5% of patients in groups 1 and 2, respectively. There were no significant differences between groups in terms of dominant side involvement
There was no difference between the two groups in terms of age, body mass index (BMI), work status, education levels, duration of the complaint, or gender (p > 0.05; Table 1). In group 1, 18.6% of the patients were male and 81.4% were female. In group 2, 33.3% of the patients were male and 66.7% were female. LE was detected on the right side in 35 patients and on the left side in 10 patients in group 1. In group 2, 32 patients had LE on the right side and 9 had LE on the left side. The dominant side was affected in 88.4% of patients in group 1 and 79.5% of patients in group 2. There was no difference between groups with respect to dominant side involvement.
Demographic data of the groups.
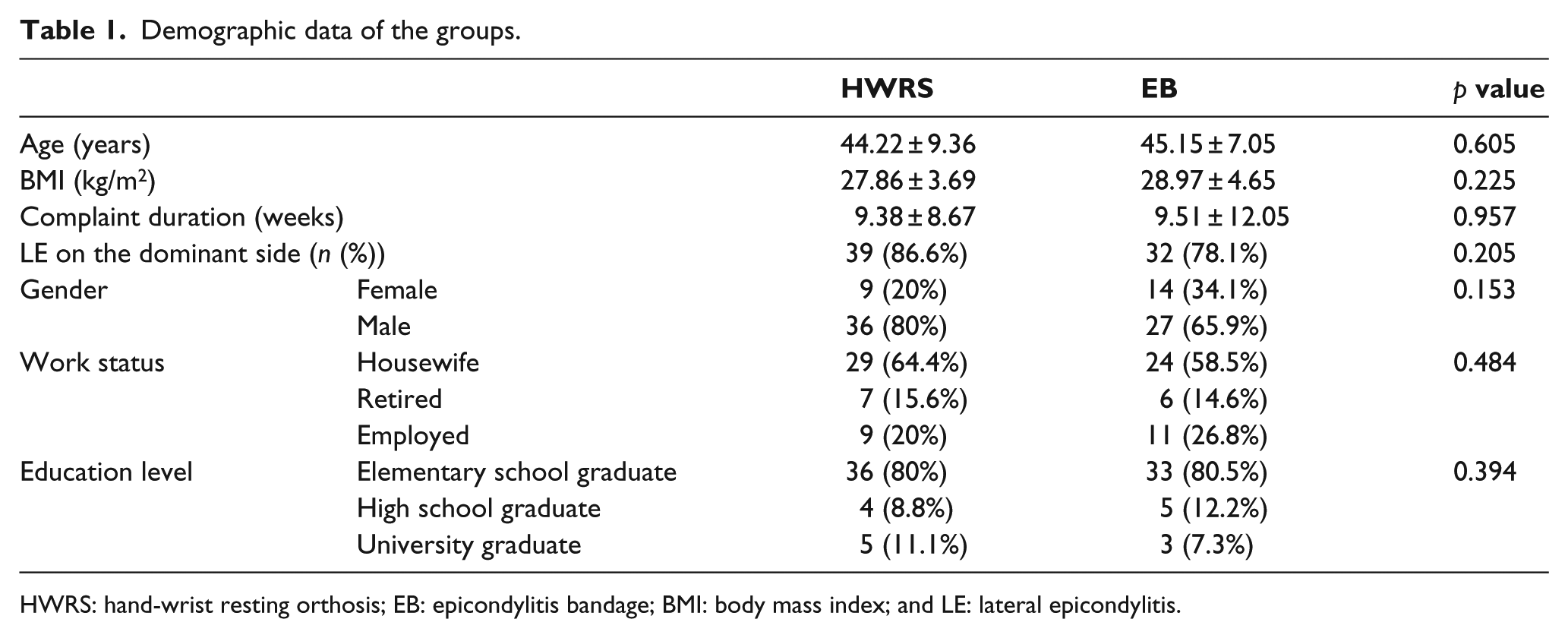
HWRS: hand-wrist resting orthosis; EB: epicondylitis bandage; BMI: body mass index; and LE: lateral epicondylitis.
A statistically significant recovery was detected in both groups when compared with the basal values after the therapy for all parameters (Tables 2 and 3). However, there was no significant difference between the percentage change scores of HGF, VAS levels during resting and maximum hand grasping, function and disability levels determined by DASH, and health-associated quality-of-life scores as determined by the SF-36 in both groups before therapy and at the sixth week of therapy (Table 4).
Pain and functional capacity, HGF, and quality-of-life measurements for group EB.
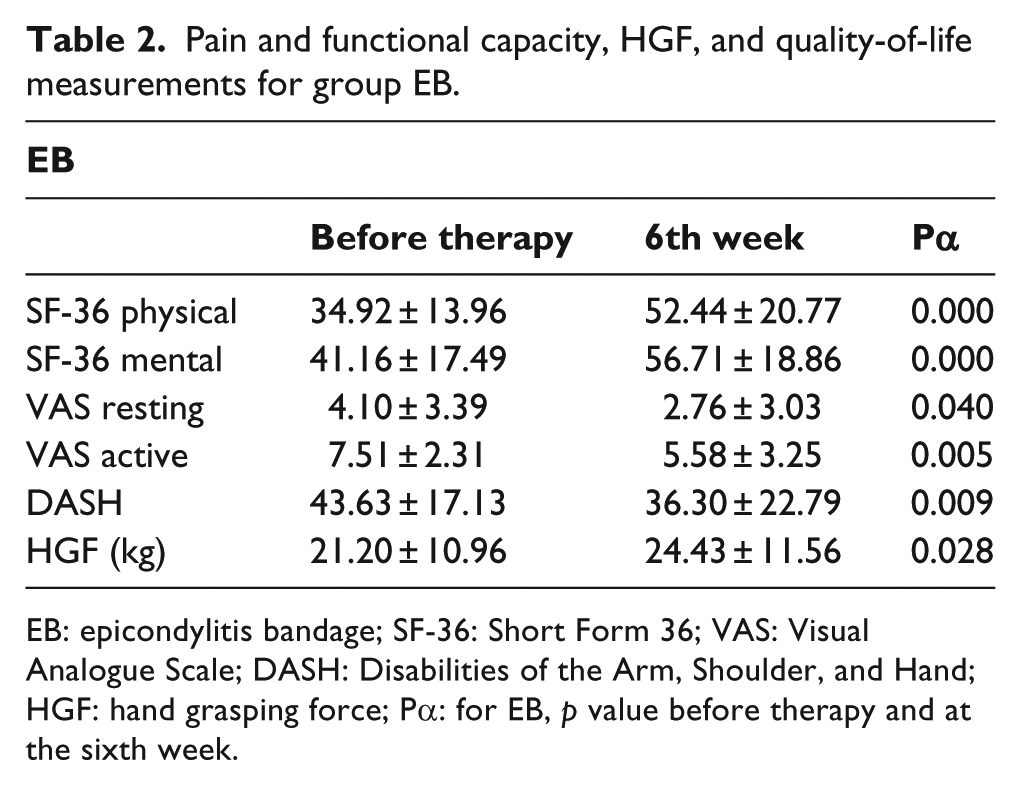
EB: epicondylitis bandage; SF-36: Short Form 36; VAS: Visual Analogue Scale; DASH: Disabilities of the Arm, Shoulder, and Hand; HGF: hand grasping force; Pα: for EB, p value before therapy and at the sixth week.
Pain and functional capacity, HGF, and quality-of-life measurements for group HWBO.
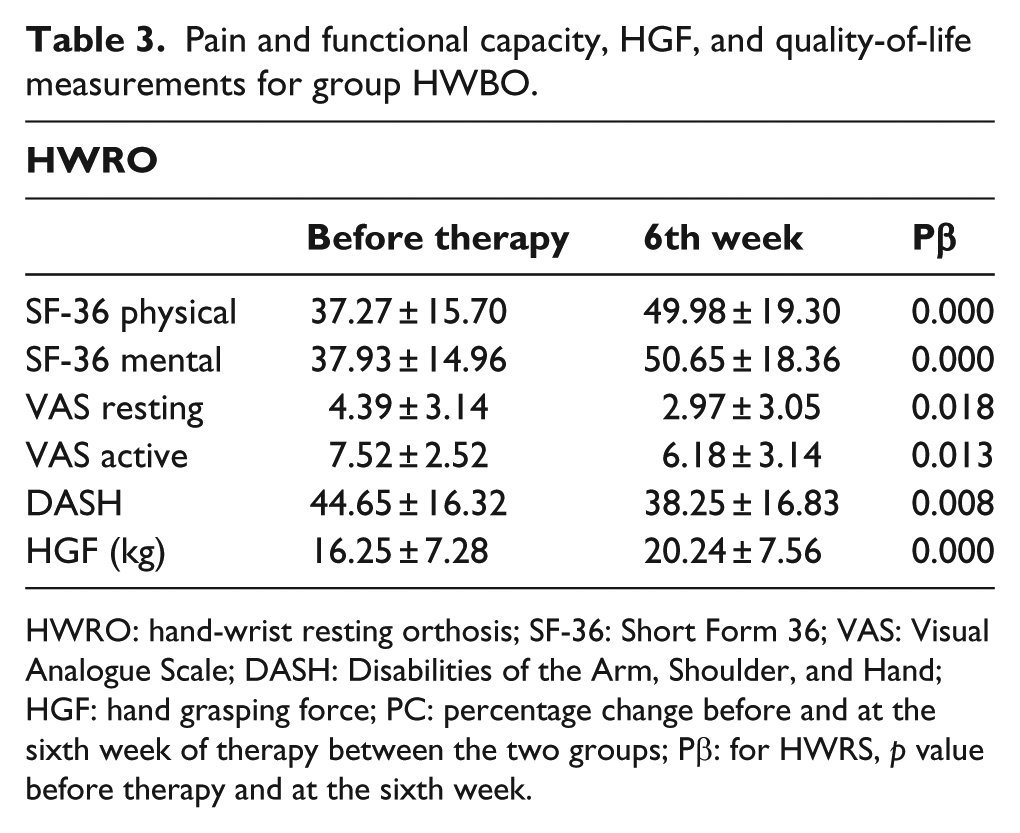
HWRO: hand-wrist resting orthosis; SF-36: Short Form 36; VAS: Visual Analogue Scale; DASH: Disabilities of the Arm, Shoulder, and Hand; HGF: hand grasping force; PC: percentage change before and at the sixth week of therapy between the two groups; Pβ: for HWRS, p value before therapy and at the sixth week.
Percentage change of both groups before and after the treatment.
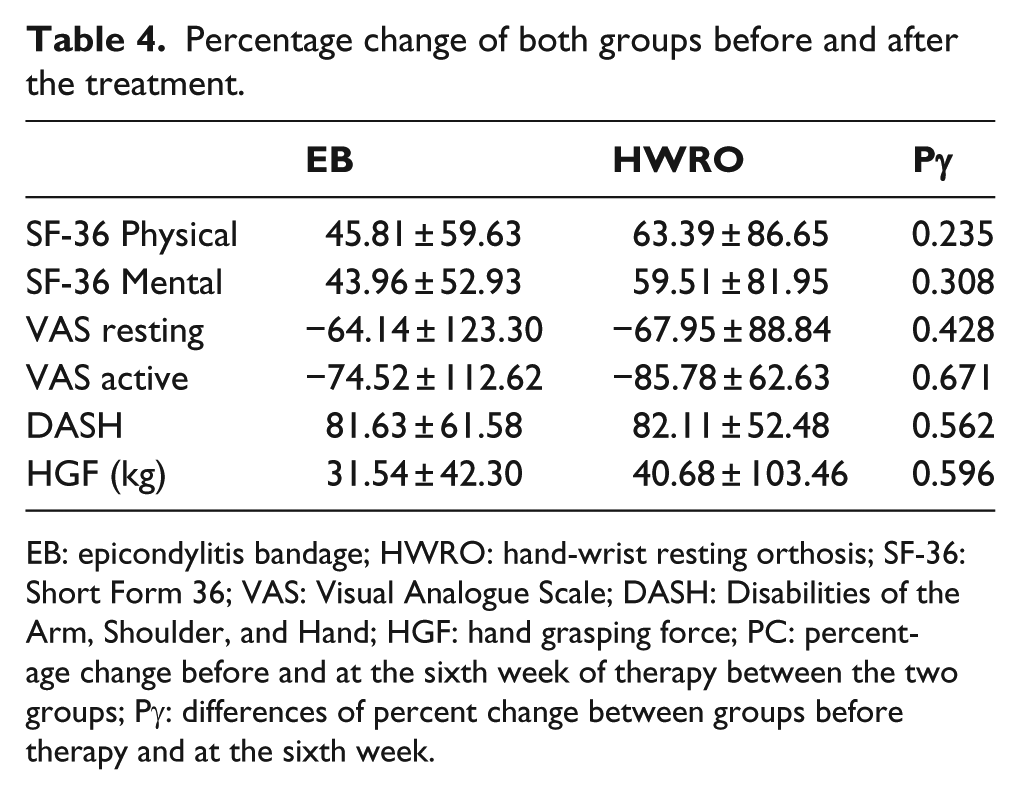
EB: epicondylitis bandage; HWRO: hand-wrist resting orthosis; SF-36: Short Form 36; VAS: Visual Analogue Scale; DASH: Disabilities of the Arm, Shoulder, and Hand; HGF: hand grasping force; PC: percentage change before and at the sixth week of therapy between the two groups; Pγ: differences of percent change between groups before therapy and at the sixth week.
Discussion
LE is one of the most common pathologies of the musculoskeletal system. The aim of LE treatment is to relieve pain, improve function, and increase functional capacity to normal, if possible.14,16 Prevention and preservation are essential for treatment. First, the patient should avoid repetitive heavy wrist activities. There are various therapy options for LE. The most common treatment methods are non-surgical options. Conservative methods suggested for LE include the resting cast—orthosis, other types of orthoses, 8 physiotherapy, electrotherapeutic therapy (laser, extracorporeal shock wave therapy (ESWT), electromagnetic area and ionization, ultrasound (US), and phonophoresis),8,17,18 and methods except electrotherapy like acupuncture, botulinum toxin, non-steroidal anti-inflammatory drugs, local corticosteroid, and complete blood injection.8,19,20 Recovery rate was 75%–90% in patients with LE following conservative therapies. The majority of patients diagnosed with LE can be effectively managed without surgery. It is usually a self-limited process from which up to 90% of patients will recover by 1 year without surgical intervention. Surgical procedures can be performed in patients with chronic disease who cannot improve through conservative treatments and whose complaints persist over long periods. 1
Orthoses are frequently used for LE treatment and they are inexpensive. The main purpose of orthosis use in LE treatment is to decrease the overloading of impaired extensor muscles of the wrist. Orthoses can facilitate daily activities and be effective in improving functions by reducing pain and increasing the grasp strength. However, exact results could not be obtained on the effectiveness of orthoses in LE and it has been reported that further investigations are needed.16,2122–23
In the present study, we examined the effectiveness of two common splint types for LE treatment. The HWRO and EB were used to determine their effects on pain, functional status, HGF, and quality of life. We demonstrated that both splint types are effective and reliable options for LE-dependent pain, functional status, muscle strength, and quality of life. Furthermore, neither treatment is superior to the other in terms of these parameters.
An EB is a device that is placed below the elbow. It applies a compressive force close to the origin point of the wrist extensor muscles. It has been shown that an EB might reduce strength production and lengthening of the muscles. Synder-Mackler et al. used electroneuromyography (ENMG) on extensor muscles of the wrist and determined that there was a significant decrease in the muscle strength when comparing the strength of the muscle with and without EB. 17 In a study on cadavers and clinical cases by Meyer et al., this decrease was found to be 13%–15%. 24 An alternative orthosis strategy is to conserve the wrist. Wrist extensor muscles undertake a stabilizing task during hand functions. A hand bandage holds the wrist at an extension of 15–20° and supports stabilization. Thus, it reduces overloading and tension on the wrist extensor muscles and contributes to resting through fixing the wrist.10,25–27 Jansen et al. 28 detected a significant decrease in the electrical activity in the wrist extensor muscle group with a splint when compared with the group without a splint in ENMG measurements and lifting activities. It was assumed that the tension on the tendons decreased during these activities.
Although studies conducted on use of orthoses in LE treatment are limited, some of these studies have compared orthoses with other treatment methods, whereas others compared one type of orthosis with other orthoses. In the studies comparing orthosis applications with other treatment options, Erturk et al. 29 and Jensen et al. 30 both found no difference between steroid injections and an elbow splint on pain relief. However, Haker and Lundeberg 31 found that steroid injections were more effective than orthoses for relieving both short-term and medium-term pain. Dwars et al. 32 did not find any significant difference between a physiotherapy group and an elbow splint group for pain relief. Holdsworth and Anderson 33 did not find any significant difference between a therapeutic USG and an elbow orthosis on pain relief. Struijs et al. 34 did not find any difference in pain and function during at least a 1-year follow-up; however, they reported an improvement rate of 89% in the physiotherapy group, 86% in the splint group, and 87% in the combined group after a 12-month treatment period.
The functional and disability level of the upper extremity and patient’s quality of life were determined using DASH and SF-36 questionnaires. A statistically significant recovery was detected in both groups between the pre-therapy values and the values at the sixth week in terms of DASH scores and the SF-36 mental and physical component scores. However, no differences were found between the two splint types for these parameters. Therefore, while deciding for orthoses in LE treatment, patients’ preferences should come first since the outcomes indicate that both orthoses are equally effective. A recent study comparing orthoses with each other determined that an exact outcome could not be decided on splint effectiveness for LE treatment because of various problems associated with the control, types of the orthoses used, duration of complaints, the variety of prognostic factors, and low case counts. 16 In some studies, a wide variety of orthoses have been used. 22 In these studies comparing several orthoses, a conclusion as to which was more effective was not made. Garq et al. compared an epicondylitis brace with a wrist brace applied to the forearm and found that the wrist orthosis was more effective than the forearm orthosis in relieving pain. Although this result conflicts with our study, they also found that neither orthosis was superior to the other with respect to functional parameters. 10 Sadeghi-Demneh and Jafarian 9 determined that all elbow and wrist orthoses are effective and side-effect-free methods that should be included in therapy programs. Altan et al. compared an elbow splint with a wrist splint and concluded that both orthoses relieved pain in LE treatment. However, while the elbow splint relieved resting pain significantly more than the wrist splint during the second week, the two orthoses were no different during the 6-week follow-up examination; thus, they concluded that the elbow orthosis might be more cosmetic. 35 Similarly, Van De Streek et al. 36 did not find a significant difference in their study comparing pain during grasping, grasping force, daily activities, and the worst-experienced pain in two orthosis groups over a 6-week period. Wuori et al. 37 compared elbow and wrist orthoses and found no superiority for either orthosis when compared to each other. Although different opinions have been reported in previous studies, an improvement in pain and functional capacity through splint applications has been achieved.
In line with previous studies, we found that the two orthoses (EB and HWRO) compared in LE treatment are both easily accessible, are cost-effective, and provide effective therapies in the treatment of LE. We found no difference between splint methods on pain relief; rather, both orthoses were effective methods for LE-dependent pain, functional status, muscle strength, and factors affecting quality of life. However, neither of the methods was superior to the other.
From oral feedback obtained from patients in the present study, those who used the HWRO reported that they had difficulty using the splint during daily life; however, similar feedback was not reported by the patients from the EB group.
Therefore, we believe that, considering the patients’ life standards, whether they can use the orthoses or not and having them informed about orthoses and after taking their opinions, the orthosis selection may be made. Since housewives in our country repeat various activities such as child care, house cleaning, and washing, in which the wrists are frequently used and constrained, it is likely they may have LE. Therefore, housewives were not considered as an unemployed group or a group that never or rarely use their hands. Therefore, they were included in our study.
Limitations of our study include that it was carried out in a single city center and had a limited number of patients. We also did not have a control group had no an orthosis We used combined treatment methods including exercise treatment and orthosis; so ıt was difficult to define which treatment modality had effective, and finally due to short follow-up period we did’nt observed long term effects of treatment.
Conclusion
HWRO and EB used for LE treatment are effective therapy options for pain, functional status, HGF, and quality-of-life issues. However, no differences were found between the two orthosis types for these parameters. Therefore, we believe in deciding to give a splint for LE treatment, informing the patient about the orthoses, and considering the patient’s compliance and choice would contribute positively to the treatment outcomes.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by JPJS KAKENHI (grant/award number: 26350630).