
Abstract
Background:
Challenges exist with the provision of appropriate mobility assistive devices in rural areas. The use of the direct manufacturing prosthetic socket system is a possible solution to these challenges.
Objectives:
The objective of this study was to test and explore the clients’ perspectives with the application of this device.
Study design:
Within a mixed-methods approach, a longitudinal sequential explanatory design was applied.
Methods:
The Orthotic and Prosthetic User’s Survey was administered to explore the use of the direct manufacturing prosthetic socket system in terms of function, health-related quality of life and client satisfaction. A conveniently selected sample of 21 individuals who suffered a unilateral trans-tibial amputation was included. Data were collected at 1, 3 and 6 months post fitting, and two focus group discussions were also administered.
Results:
Of the 21 participants recruited, 11 returned for follow up. Although participants reported favourably about the prosthesis, their scores were generally worse than the norms with regard to function and quality of life. Participants highlighted the need for improvement in the cosmetic appearance of the prosthesis.
Conclusion:
The direct manufacturing prosthetic socket system could be considered as an alternative technique of socket manufacturing for individuals living in rural areas due to the shorter manufacture time and promising initial results, but further research on this topic with a bigger sample is recommended.
Clinical relevance
The direct manufacturing prosthetic socket system may be considered as an alternative to the traditional prosthetic socket manufacturing technique used in South Africa. As this device requires only one visit and therefore decreased travel by the patients to the hospitals, it could be applicable to more amputees who cannot return to hospital post discharge.
Background
The provision of appropriate assistive technology and services in rural settings has become a matter of international interest and relevance. 1 South Africa has signed and ratified the Convention on the Rights for Persons with Disabilities (CRPD) committing to ‘facilitating access to persons with disabilities to quality mobility aids’. 2 Some of the challenges relating to fulfilling this commitment have been established in the literature and include difficulty in accessing services, a lack of trained prosthetists and availability of materials.3,4 Globally, researchers and scientists are attempting to address these challenges.
The patellar tendon bearing (PTB) plaster casting technique of socket fitting that is currently used in most developing countries, including rural areas in South Africa, is time consuming to manufacture. The fitting requires multiple visits from the patient, pre-fitting as well as post-fitting. 5 There is also still an immense shortage of trained prosthetic staff in most developing countries. 6 The solution to the challenge created by the lack of prosthetic manpower and the time-consuming technique currently used to manufacture and fit a socket for a prosthesis, is to either train more technicians or optimise the process of socket manufacturing for the fitting of a prosthesis.
The direct manufacturing prosthetic socket system (DS) offers a possible solution to the challenge highlighted above. The short time required for socket manufacturing can alleviate the burden on understaffed prosthetists servicing rural areas. It also provides a solution for the long waiting times for prostheses in the public sector in South Africa. Thus far, the use of DS has not been evaluated in a rural setting. It is currently being used in the private sector in many countries including the Scandinavian countries, United Kingdom, China and South Africa. 7
This pilot study aimed to evaluate the use of the DS as an alternative to the time-consuming PTB technique of socket manufacturing that is used in this rural setting.
Methods
The DS manufacturing process was developed and introduced by Össur®. The DS interface components of a prosthesis are in direct contact with the wearer. They are the means of achieving axial stabilisation, transverse stabilisation and suspension. 8 Interface components included in this study were the socket (referring here to the hard socket made from glass fibre and polyurethane under pressure), the suspensory components (referring here to a pin suspension that is attached to the distal part of the liner and locked with a shuttle lock in the distal part of the socket) and the liner (referring here to a silicone liner, selected from different sizes measured by the circumference 4 cm from the distal end and then rolled on to the residuum). The liner is held in place through the combination of vacuum and friction between the skin and the silicone material.
The DS interface is manufactured by applying resin (that hardens in 5–10 min under applied pressure) directly onto the protected residual limb and can be manufactured and fitted in one visit. In this study, the DS prosthesis that was provided to participants consisted also of a silicone liner, pin locking system, aluminium pylon and a solid-ankle cushion-heel ankle cushion heel (SACH) foot.
Ethical clearance was obtained from the University of the Western Cape’s Ethics committee (No. 11/4/3). Permission to conduct the study was obtained from the KwaZulu-Natal (KZN) Department of Health, hospital and therapy department managers. A mixed-methods approach, and a longitudinal sequential explanatory design, was utilised to evaluate the use of the DS in a rural setting. 9 The use of the DS was evaluated in terms of function, health-related quality of life (HRQoL) and satisfaction with prosthesis. The Orthotic and Prosthetic User’s Survey (OPUS) 10 was used to collect data at 1, 3 and 6 months post fitting and two focus group discussions (FGDs) were used to collect qualitative data.
Data for this study were collected in a rural district in the KZN province in South Africa. In the KZN province, 54% of the total population is rural and 83% of the people living in this particular health district live below the poverty line.11,12 Participants were recruited by Physiotherapists working at the district hospitals and accessed at the Physiotherapy department of the regional hospital that services this rural district. A total of 21 participants were recruited based on the inclusion criteria. Males and females aged 18–75 years who suffered a unilateral trans-tibial amputation more than 6 months ago, who never used a prosthesis before and had no pre-existing neurological or neuromuscular impairments that hamper gait, were included in the study.
The participants’ level of literacy was not considered as an inclusion criteria due to the high number of people who are illiterate in this area. To account for this and avoid inconsistency, all questionnaires were interviewer administered by the research assistant. If on inclusion in the study a participant stated that they were unable to return for follow up, they were excluded from the study.
Exclusion criteria were amputees who had a
Residual limb length longer that 25 cm or shorter than 12 cm;
Distal circumference larger than casting liner size 34 cm or smaller than size 16 cm;
Body weight of more than 100 kg (220 lbs).
The inclusion criteria used in this study were based on Össur’s® guidelines for fitting of the DS.
The DS was applied by two professional prosthetists working in the central prosthetic workshop that provides service to this area. Both prosthetists were trained by the manufacturer of the components in the technique of socket fitting and supervised by an expert prosthetist with experience in the DS for the first two fittings. The local prosthetists had little or no experience in this technique prior to participating in the study.
Once the potential participants were recruited into the study, they were screened by the local prosthetist to see if the stump was adequately shaped for prosthetic fitting. The local prosthetist then manufactured the socket and fitted the patient with the prosthesis. An isiZulu-speaking research assistant taught the patient how to don the prosthesis and educated them on how to take care of the silicone liner at home. The physiotherapist and the prosthetist would subsequently ensure that the patient was able to walk safely with the prosthesis and issue an appropriate assistive device when available. Follow-up appointments and a cash stipend were given to the participant in order to return to continue participating in the study in 1, 3 and 6 months’ time.
On the 1-month follow-up visit, the participant was interviewed regarding any complaints and then the research assistant verbally administered the OPUS follow-up survey (Figure 1). The OPUS consists of five constructs, namely, lower extremity functional status, upper extremity functional status (not included in this study), HRQoL, satisfaction with device and satisfaction with services (not included in this study due to the artificial nature of the ‘service’ provided). 10 The English version of the OPUS is a valid and reliable tool for data collection, and it was translated into the local language by a professional translator. The translated version was then translated back into English to ensure the quality of the translation, and no discrepancies were identified. However, the isiZulu version of the OPUS was not tested for validity and reliability after translation. The participants were then given a 3-month follow-up appointment that coincided with the prosthetic clinic date. The same procedure that was followed for the 1-month follow-up was followed for the 3- and 6-month follow-up. The FGDs that were conducted at 3 and 6 months post fittings were conducted in a private office at the regional hospital’s therapy department and lasted approximately 45 min. All participants who returned for the 3- and 6-month follow-up participated in the FGDs. Each focus group was started with the grand question: ‘Tell me more about your experience with your new false leg (prosthesis)’ and conducted with the assistance of an isiZulu-speaking translator. As participants responded, probing questions were used to obtain more information relating to their functioning in their home environment, some challenges experienced, quality of life and general satisfaction with the prosthesis. The FGDs were audio-recorded, transcribed verbatim and translated from isiZulu to English where necessary.
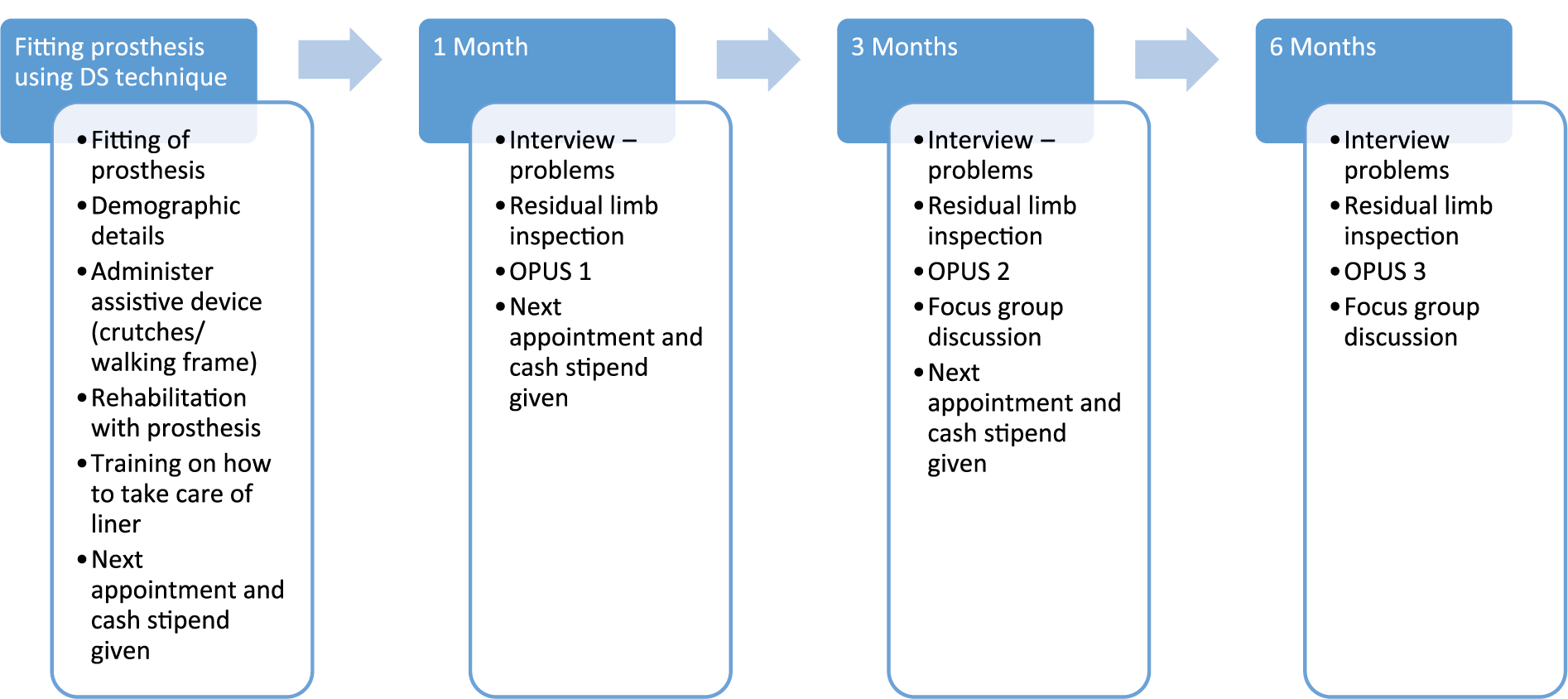
Process of data collection.
Analysis of data
Quantitative data
Owing to the small number and variability in the prosthetic users who returned for follow-up (Figures 2 and 3) after fitting of the prosthesis, only measures of central tendencies such as means and frequencies were used to analyse the data obtained from the OPUS. 13
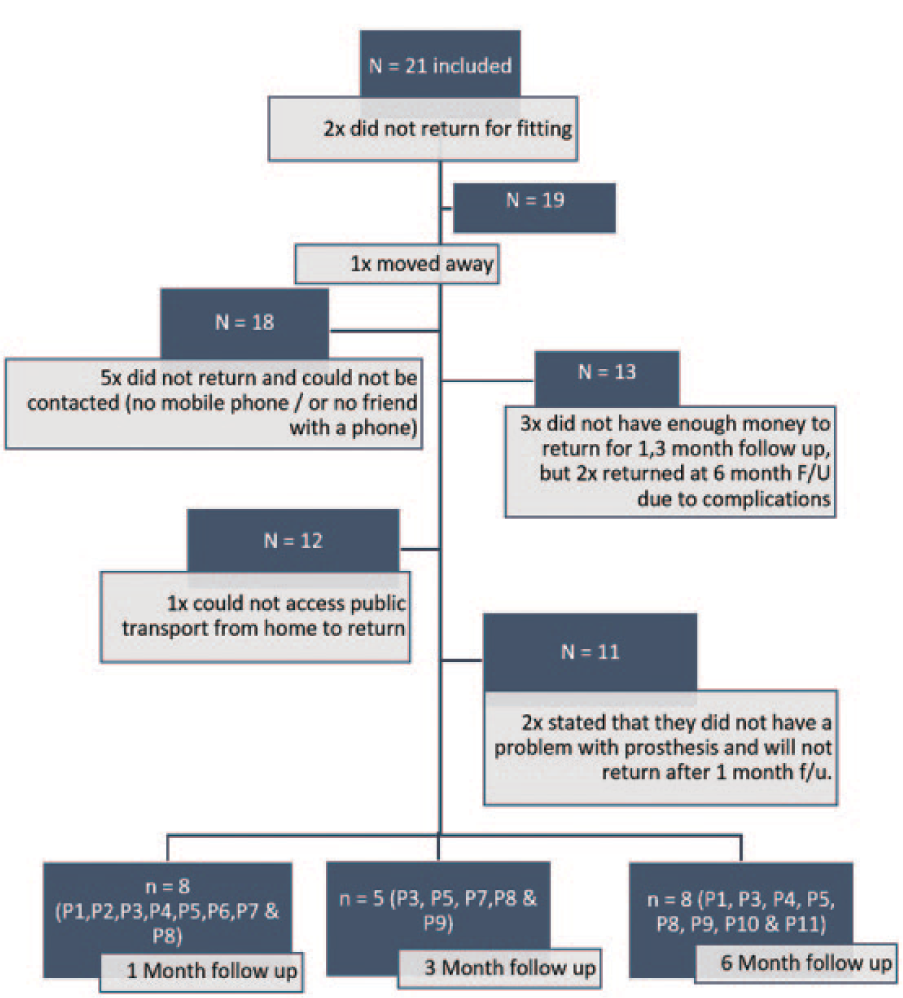
Attrition of study sample.
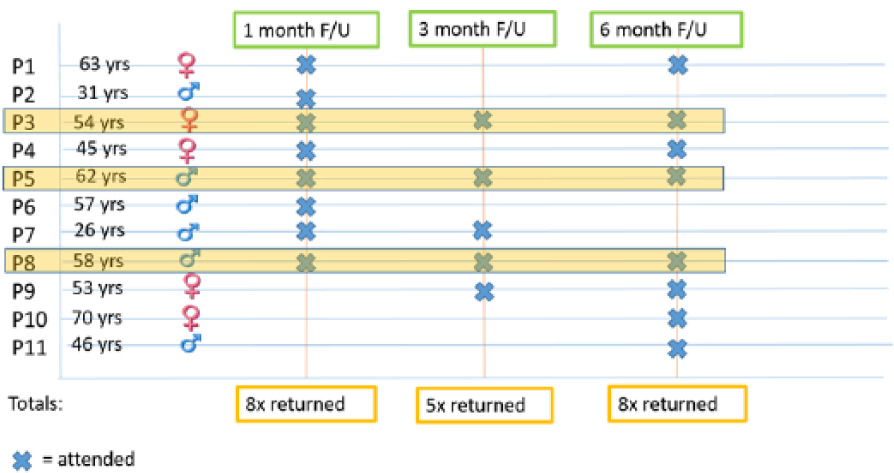
Description of participants who returned for follow-up.
Qualitative data
The FGDs were transcribed verbatim and analysed using Cresswell’s seven-step process of thematic analysis (Figure 4). 14
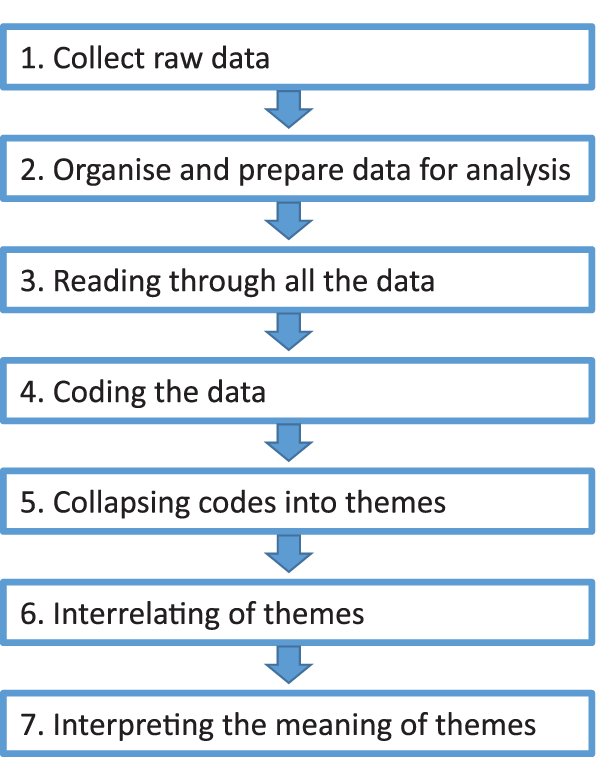
Analysis of qualitative data.
Results
A total of 21 persons with a unilateral trans-tibial amputation were conveniently selected for inclusion in the study group between June 2013 and June 2014. Of these 21 participants who were included in the initial sample, 19 patients were fitted with the DS (Figure 2). Eight returned for the 1-month follow-up, five returned for the 3-month follow-up and eight returned for the six-month follow-up (Figure 3). All participants who did not return for follow up on 1 month were called in order to determine the reason. Five participants could not be reached on the contact numbers that they provided or did not have phones. Three participants stated that they did not have enough money to pay for transport (even though a cash stipend was provided) and one participant was unable to access public transport at all. However, two of the participants who stated that they did not have money returned at 6 months when they had complications with the use of the prosthesis. One participant moved to another province and two others stated that they were happy with their prostheses and subsequently withdrew from the study. The reasons that participants provided telephonically for not returning to the hospital are presented in Figure 2.
The demographic details of participants and problems relating to the use of the prosthesis are presented in Table 1. The main complaints raised were relating to the loss of residual limb volume and sweating and itchiness of the residual limb in the silicone liner.
Demographic details, cause of amputation and problems experienced with prosthesis.
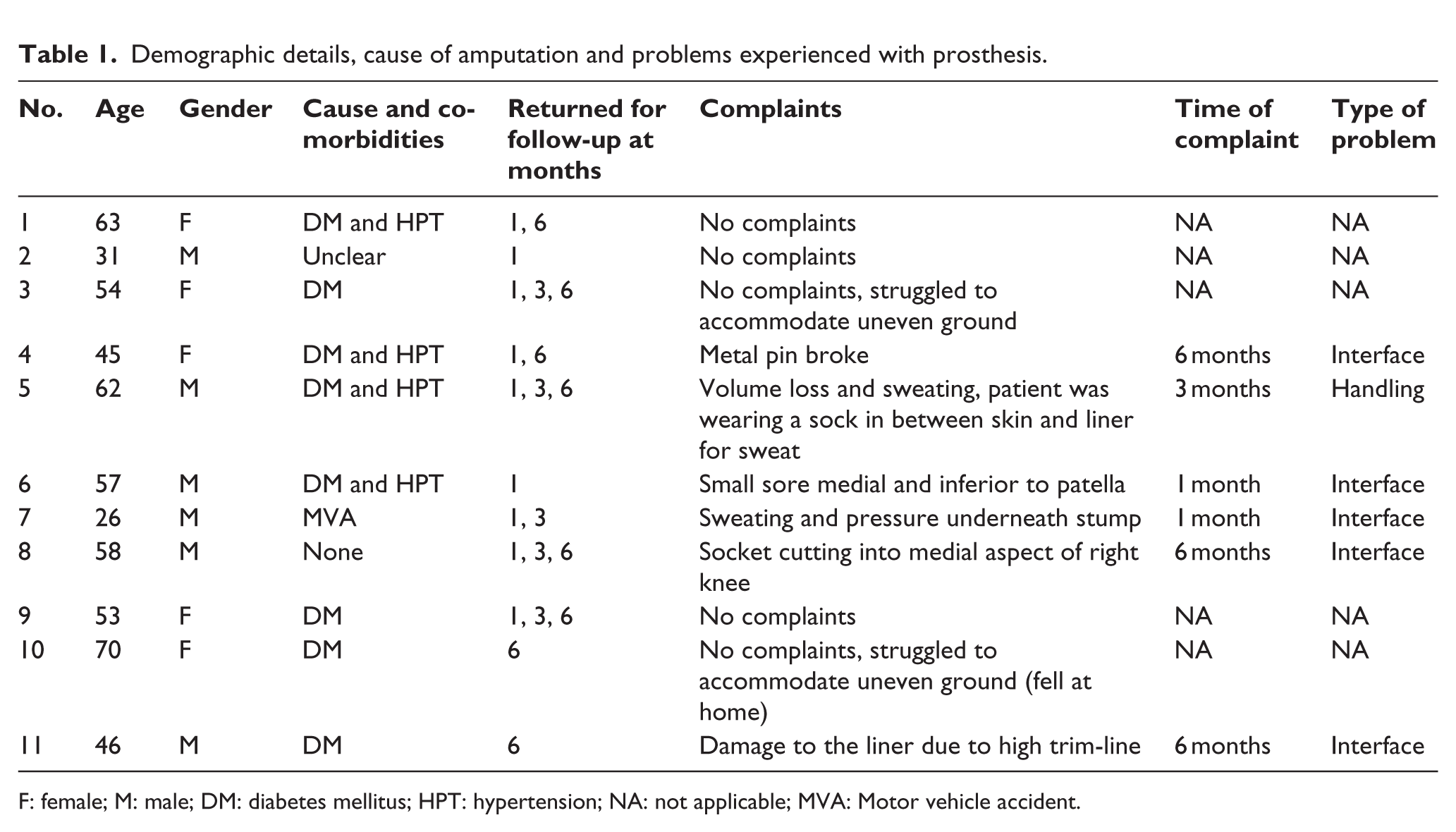
F: female; M: male; DM: diabetes mellitus; HPT: hypertension; NA: not applicable; MVA: Motor vehicle accident.
Quantitative data
Functional status
The module is scored out of 100 and consists of 20 Likert-scale questions. Answers are scored from one (very easy) to five (cannot do this task) based on the ease or difficulty to complete each task. Participant scores for the OPUS were compared to the OPUS norms provided in the scoring guide of the instrument. 10 The norm value is 54 points and is based on the average scores of participants who have previously completed this survey. Participants using the DS scored similarly (M = 54, standard deviation (SD) = ± 6.5 (range, 44–68)) to the OPUS norms on 1-month follow-up: much better than the norm at 3-month follow-up (M = 42, SD = ± 14 (range, 22–61)) and worse than the norm for the 6-month follow-up (M = 54, SD = ± 11.5 (range, 36–68)) (Figure 5).
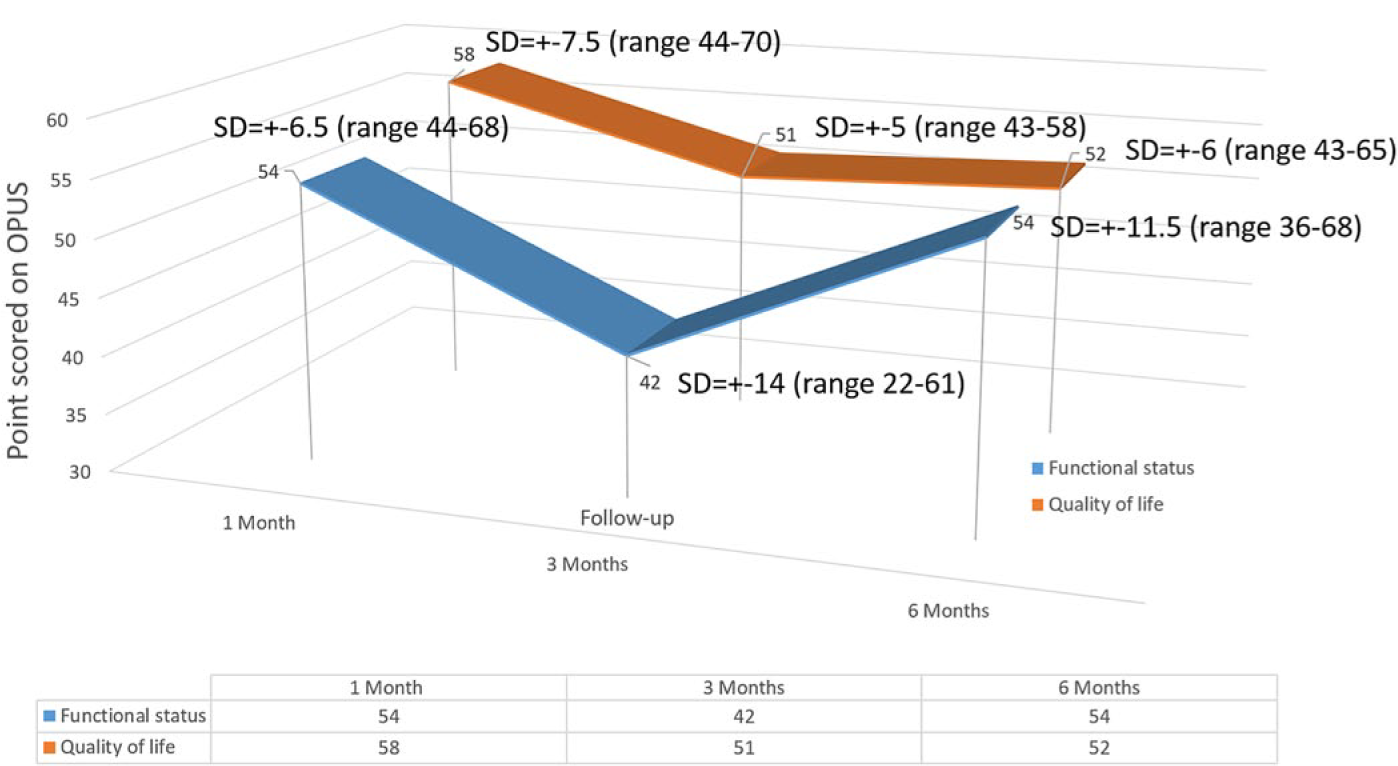
OPUS scores at 1-, 3- and 6-month follow-up.
Quality of life
The quality of life index consists of 23 Likert-scale questions and is scored similarly to the functional status measure, but out of a total of 115. The norm value for this module is 51. Participants scored higher (worse HRQoL) than the norm values for the OPUS at 1-month follow-up (M = 58, SD = ± 7.5 (range, 44–70)), the same as the norm (M = 51, SD = ± 5 (range, 43–58)) at 3-month follow-up and just higher than the norm (M = 52, SD = ± 6 (43–65)) at 6-month follow-up.
Satisfaction with prosthesis
Only six participants completed the ‘satisfaction with prosthesis’ section of the OPUS follow-up questionnaire at 1-month follow-up. This was due to human error in the copying of the survey. Participants’ average score for this section of the questionnaire was 33 points (SD = ± 4.5 (range, 27–38)). This average was 10 points higher (less satisfied) than the norm for this section of the survey (23 points).
Complaints relating to the prosthesis
The problems that were reported during follow-up were sorted into three categories affecting the use of prosthesis, namely, (1) no problem (n = 5), (2) interface problem (n = 5) and a handling problem (n = 1). An interface problem was referred to a problem with the socket, liner or the suspension, and a handling problem was categorised when the complaint is related to the incorrect handling of the prosthesis (Table 1).
Qualitative data
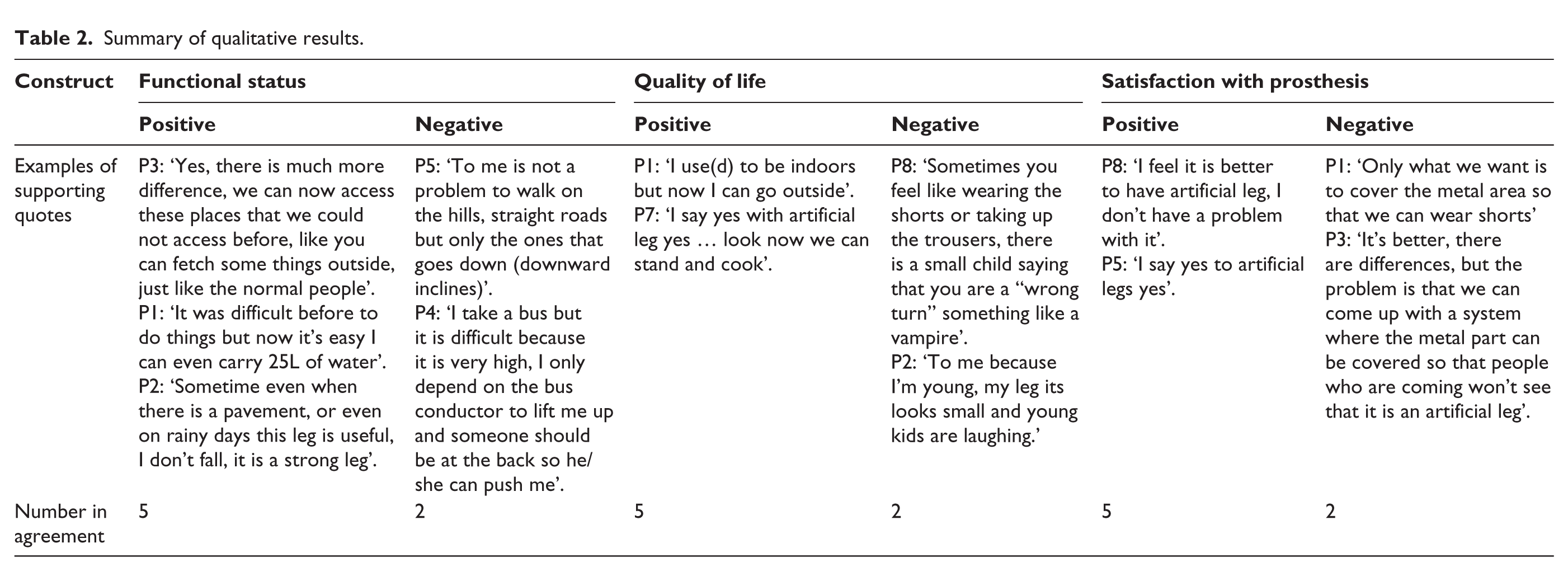
A summary of qualitative results is provided in Table 2.
Summary of qualitative results.
Functional status
Overall, participants reported improved functionality with the use of the prosthesis. Improved independence and the ability to perform tasks such as cooking and fetching water were reported.
The use of a prosthesis assisted participants to become more integrated at home, but not necessarily into their communities. Some participants were able to accommodate busy streets and pavements, but faced challenges accommodating uneven terrain and using public transport.
Quality of life
Participants reported an improvement in psychological well-being and increased functional independence. Qualitative data on HRQoL were mostly positive, but some participants still experienced mocking and stigmatisation from the community.
Satisfaction with prosthesis
The qualitative explanation given for the fairly poor satisfaction rating at 1-month follow-up was that the participants were not happy with the cosmetic appearance of the prosthesis and wanted the metal pylon to be covered with Durafoam in order to more closely resemble their unaffected limb.
There were, however, also patients who reported being satisfied with their prosthesis regardless of its cosmetic appearance.
Complaints relating to the prosthesis
The qualitative data confirmed the quantitative data in that the majority of complaints were related to sweating and itchiness of the stump in the silicone liner initially. This seemed to subside after 6 months. Another concern was the normal shrinkage of the stump in primary prosthetic users after approximately 3 months:
P1: …there is sweat in the leg, so there is a wound coming, and its pain is coming day by day, so it is not comfortable to use the leg. P7: As I said from the beginning I have no problem with my leg, the problem is that the leg (residual limb) is becoming smaller.
Discussion
Participants qualitatively reported improved functionality, independence and an improvement in activities of daily living with the use of the DS prosthesis. Because participants were primary prosthetic users, this finding corresponds with the literature in stating that the use of a prosthesis will minimise some of the barriers to activities of daily living and participation in society. 15 However, in this study sample, the environmental challenges posed by the setting and the public transport system still limited full reintegration into society. Also important to note is that the positive change in function and HRQoL cannot solely be attributed directly to the specific type of socket that was used in this study because there was no control group to compare it to.
After 3 months, the residual limb had shrunk (as expected in primary prosthetic users), negatively affecting patients’ balance and subsequent function. 16 The activities that the participants reported having most difficulty with were walking on uneven surfaces and on steep inclines such as hills. This finding was supported by the qualitative data and corresponds with the literature on functional difficulties among prosthetic users in rural settings.17,18 The question that arises from this finding is how can assistive technology be adapted to accommodate uneven surface and inclines well? A possible explanation for this finding could be the rigid SACH foot that was used in this study. A rigid foot is not ideal for walking on uneven surfaces. A number of attempts have been made to accommodate the uneven surface with more pliable feet such as the Jaipur foot. 19 Further research needs to be done in order to determine the suitability of other prosthetic components, perhaps in combination with the DS that would better suit the environmental demands of rural areas.
At 1-month follow-up, HRQoL scores were much worse than the norm values; at 3 months it improved and stayed fairly constant at 6 months. This finding is consistent with what is expected from the literature that reports an improved quality of life in persons with a lower limb amputation after 6 months, when compared to 1 or 3 months. 20 A possible explanation for the fairly low quality of life scores initially could be the stigmatisation that participants experienced based on the cosmetic appearance of their prosthesis. Other factors that should be taken into consideration when interpreting HRQoL scores in a rural setting are the impact of socioeconomic status and social support on HRQoL. The high levels of unemployment and poverty in this specific area could contribute to an overall lower HRQoL than the norms of the OPUS that was established in an urban setting.
Some patients were very satisfied with the prosthesis, but a major cause of dissatisfaction initially was the aesthetics of the prosthesis. The DS users’ pylon was not covered, so the metal was visible when participants wore shorts. In many rural communities as well as in this community, disability is still stigmatised, and even though participants were satisfied with their function with the prosthesis, the aesthetics of it was a very important consideration. This finding corresponds with the findings of a study on the satisfaction with prostheses in Tehran, Iran. 21 They reported that the highest level of dissatisfaction with prostheses was directly related to cosmetic appearance. This finding is also in line with studies on prosthetic components for use in developing countries which noted that cultural sensitivity is required when fitting prostheses in developing countries. 17 A possible explanation for the stigmatisation of people with disabilities in rural settings could be cultural beliefs regarding the cause of disability. Such cultural beliefs influence health-seeking behaviours and utilisation of rehabilitation services in this specific rural area and contribute to the stigmatisation of disability. 22 All participants who requested their pylon to be covered with Durafoam to create a more realistic lower leg were given the opportunity during the study, which could possibly explain the improved quality of life after 3 months. The cosmetic appearance of prostheses is of utmost importance in many rural communities and should be carefully considered in future studies.
The clinical importance of taking note of complaints of discomfort during prosthetic use is that prosthetic users could potentially discard their prosthesis if it is not comfortable enough, wasting valuable resources. The finding that sweating was the most common complaint corresponds with a systematic review of the literature reporting skin perspiration and itching to be a common occurrence with the use of silicone liners. 23 This study was conducted in a subtropical region, and the heat and humidity in this area might contribute to the sweating and itchiness. Not all households in the rural setting have access to running water, which might contribute to the itchiness if patients are unable to wash the liner regularly. This is important for consideration in a population where diabetes mellitus is the most common cause of lower limb loss, ulcers heal with difficulty and could result in re-amputation. Alternative solutions for a more appropriate skin–socket interface should also be explored.
Field testing a prosthesis is always challenging, but even more so in a rural setting. 24 The main limitation of this study was the large attrition rate and the potential bias that it introduced to the study findings. It does, however, illustrate the patients’ difficulty with follow-up for prosthetic care in a rural setting. The majority of the participants who returned for follow-up mainly did so due to problems or concerns with the prosthesis, and this will negatively bias the functional and HRQoL scores. If experienced prosthetic users were recruited for the study, the scores might have been more positive. From the qualitative data, it became evident from the 6-month follow-up FGD that the drop in functional status scores was as a result of some complaints relating to the fitting of the prosthesis. The prosthetists had little or no prior experience in the application of the DS, and this could have affected the participants’ socket comfort and subsequent functional scores. Even though the quality of the translation of the OPUS was assessed, validity and reliability of the translated instrument were not tested and could bias the findings of the study. Due to the fact that the research assistant made additional copies of the OPUS and accidentally did not copy the last section of the survey (satisfaction with prosthesis), a limited number of participants completed this section of the OPUS. The low follow-up rate experienced throughout this study negatively affects the validity and reliability of the findings and introduced attrition bias to the study findings.
Conclusion
The DS could provide a possible solution for the huge backlog in manufacturing prostheses and prosthetic staff shortages in rural settings. The fact that the DS can be manufactured in one visit can address some of the challenges with accessing prosthetic services.
Footnotes
Acknowledgements
The Grant holder acknowledges that opinions, findings and conclusions or recommendations expressed in any publication generated by the NRF supported research is that of the author(s), and that the NRF accepts no liability whatsoever in this regard.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is based on the research supported in part by the National Research Foundation of South Africa (Grant nr. 84336), and some of the some of the prosthetic components were provided by Ossur South Africa.